
記住我
Osteochondritis dissecans (OCD) of the humeral capitellum is a common cause of elbow disorders among young throwing athletes. The progression of OCD can be divided into three stages: the radiolucent stage, the fragmentation stage, and the loose body stage [1]. In the radiolucent stage, the lesions start in the subchondral bone with intraosseous subchondral osteopenia and present as translucency on X-ray. As the disease progresses, a sclerotic ring can be seen that distinguishes the lesion from the surrounding healthy bone, and the lesion is separated from the surrounding tissue as a fragment. As the disease becomes worse, the lesion has completely separated from the surrounding tissue, forming a loose body within the joint. Symptoms of OCD vary depending on the stage of the disease. In the radiolucent stage, few people feel any pain and no symptoms are present. In the fragmentation stage, the elbow may become painful, and the range of motion of the elbow becomes restricted. In the loose body stage, the pain becomes more severe, and irreversible bone deformity may occur [2,3,4]. Various studies have shown that OCD of the humeral capitellum may occur in approximately 3% of adolescent baseball players [5,6,7,8,9].
The treatment of OCD typically involves conservative treatment, but sometimes surgery is necessary. Conservative treatment needs a prolonged absence from sports activity. Activity restriction would have a role in stabilizing the OCD lesion and promoting ossification of the lesion. If successful, the bone will be repaired in about one year and the child will be able to play baseball again. Matsuura et al. [4] reported that osteochondrosis of the humeral capitellum can be successfully treated conservatively if treatment is begun in an early stage of the disease. When 84 patients with the early stage OCD (the radiolucent stage) stopped pitching and underwent conservative treatment, OCD lesions of 76 patients (90.4%) healed, on the other hand, only 4 of 33 patients (12.1%) who did not follow the instruction to stop pitching healed. In the case of 17 patients who were diagnosed as the advanced stage (the fragmentation stage), 9 (52.9%) patients who underwent conservative treatment healed, while none of the 23 patient’s OCD lesions who did not follow the instructions healed. As can be seen from this result, 90% of the patients in the radiolucent stage can be successfully treated conservatively, whereas only about half of the patients in the fragmentation stage had effective results after conservative treatment, indicating that early detection in the early stage (the radiolucent stage) is important for healing of the humeral capitellum OCD in growing baseball players. Surgery is generally required in the fragmentation stage and the loose body stage, and mainly consists of removal of the loose body, resection of the deformed bone, and osteochondral grafting [1]. However, it seems difficult to heal the joint deformity in an advanced stage, so early detection and treatment are important.
Current diagnostic methods for OCD are X-ray, computed tomography (CT), magnetic resonance imaging (MRI), and ultrasonography. Among these, one study reported that CT is the best method of examination for OCD [10]. This is because loose bodies of OCD lesions are often missed on radiographs and MRI scans [10]; whereas, CT can accurately determine the location of the lesion as well as the extent of the lesion [4, 11, 12]. On the other hand, ultrasonography is used as a medical screening because many players do not visit a hospital while they are able to continue competing despite the pain. They visit an outpatient clinic only after their condition has become severe, and medical screening using ultrasonography is needed [7]. Ultrasonography is suitable for screening because it is noninvasive, with no risk of radiation exposure, and can detect subtle changes in subchondral bone in the early stages. Not only have some studies [13] shown the usefulness of diagnosing the presence or absence of OCD from ultrasound images, but some have reported better diagnostic performance than MRI [14]. Therefore, screening for OCD by ultrasonography enables early detection and conservative treatment [7, 8, 15,16,17,18]. In this screening, orthopedic surgeons and sonographers examine baseball player’s elbows using ultrasound. However, medical check-ups for OCD are conducted only a few times a year, and there is a limited number of specialists available to perform these examinations. Furthermore, it is sometimes difficult to detect OCD lesions and the diagnosis may differ among examiners.
A related study of computer-aided diagnosis of ultrasound images that do not use deep learning is that of Acharya et al. [19]. In this study, the classification of the normal thyroid gland and Hashimoto’s thyroid gland was performed by extracting grayscale features of thyroid ultrasound images using wavelet transform, SVM, decision trees, etc. The SVM achieved the accuracy rate of 82.7%, the sensitivity rate of 93.1%, and the specificity of 69.6%. A study by Fujioka et al. [20] is a study using deep learning. This study compared the accuracy of the convolutional neural network (CNN) model, which uses the GoogLeNet model, with that of three radiologists in classifying benign and malignant breast masses based on ultrasound images. The results showed that the CNN model achieved an area under the curve (AUC) of 0.913, which was equivalent or superior to the radiologists’ accuracy.
Shinohara et al. proposed a detection model using deep learning for OCD of the humeral capitellum which has been demonstrated [21]. It evaluates the entire image and classifies into OCD or normal. The classification model was constructed by transfer learning of three models, ResNet50, MobileNet_v2, and EfficientNet, on images of 40 subjects, and achieved the accuracy rate of 0.818, 0.841, and 0.872, respectively. In addition, object detection of OCD lesion location is performed using YOLOv2. The mAP, which indicates the percentage of matching with the bounding box of the true value, achieved 0.83.
The purpose of this study is to propose a deep learning-based OCD detection method that automatically determines the presence or absence of OCD in ultrasound images. The detection method aims to support medical professionals without specialized expertise to screen patients for OCD using ultrasound images, solving the problem of OCD screening and increasing the possibility of early detection of OCD. The proposed method first detects the humeral capitellum of the elbow, a common site of OCD, by using the YOLO object detection method, and then classifies the detected bounding box into OCD or normal by using VGG16. We hypothesize that restricting the region of interest (ROI) on the humeral capitellum will improve the accuracy of predicting OCD compared to models built using the entire ultrasound image captured by ultrasonographic devices.
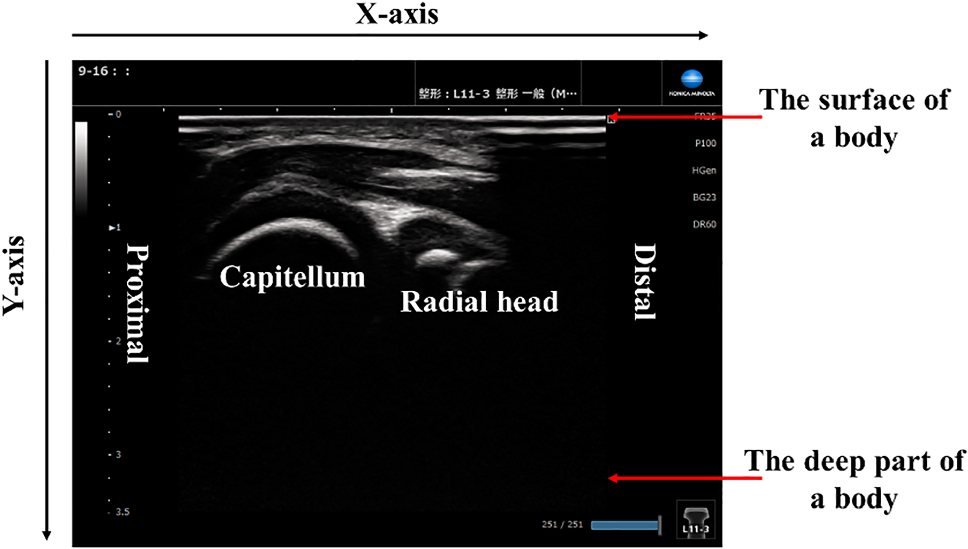
Subjects and materialsThe ultrasound images used in this experiment were taken by physicians experienced in medical check-ups of OCD using the five ultrasound systems shown in Table 1. The ultrasound images of the elbow were taken in the lateral posterior long-axis directions. Figure 1 shows ultrasound images of the elbow, where the humeral capitellum of the elbow is located on the x-axis and y-axis. The upper side of the image represents the surface of a body; while, the lower side represents the deeper part of the body (Table 2).
Table 1 Ultrasonographic devicesFig. 1
Ultrasound images of the elbow in lateral, posterior, and long-axis imaging directions
Table 2 Number of subjects used in the experimentSubjects used in this study were all male, 67 with OCD (11.7 ± 1.9 years old) and 91 with normal (10.2 ± 1.3 years old). The OCD diagnosis was confirmed by senior orthopedic surgeons using radiographs of the elbow in 45° flexion in the frontal plane. Although there were various stages of OCD cases, all were regarded as the same OCD group. Two types of data were used in the experiment: movies and still images. Movies were archived in avi format, and divided into frames, which were then used as still images in bmp format. We analyzed only images that include the humeral capitellum, a common site of OCD, but excluded images of the same location, leaving only one image. Still images were also stored as bmp files, and only images including the humeral capitellum were used. Therefore, the number of images varied from subject to subject, with a minimum of 1 and a maximum of 80 images for normal subjects, and a minimum of 1 and a maximum of 48 images for OCD subjects. The size of the images varied from subject to subject, ranging from 400 to 500 pixels in both height and width. This study was conducted with the approval of the ethics committees of the Department of Orthopaedics Graduate School of Medical Science Kyoto Prefectural University of Medicine and the Graduate School of Engineering, University of Hyogo.
留言 (0)