Disproportionality analyses were performed on de-duplicated spontaneous safety reports collected in VigiBase® as of 31.05.2023. Drugs of interest, selected as active ingredients, included suspected monoclonal antibodies erenumab (targeting CGRP receptor), galcanezumab, fremanezumab and eptinezumab (targeting CGRP-ligand), and gepants ubrogepant, rimegepant, and atogepant (all targeting CGRP receptor). Events of interest were captured by using the Standardized Medical Dictionary for Regulatory Activities (MedDRA®) Query (SMQ) “pregnancy and neonatal topics” (version 26.0). Safety reports reporting as suspected drug(s) sumatriptan, naratriptan, zolmitriptan, rizatriptan, almotriptan, eletriptan and/or frovatriptan were used for the single comparator group (Supplementary Fig. 1), to control for confounding by indication [14], and because, in the absence to date of migraine-specific preventive drugs proven safe in pregnancy, use of triptans in pregnancy appears safe [15]. Safety reports with additional suspected/interacting drugs beyond those of interest and safety reports lacking specific terms referring to drug exposure in pregnancy (including “maternal exposure before pregnancy”, “foetal exposure during pregnancy”, “maternal exposure during pregnancy”, “maternal exposure during breastfeeding”, “paternal exposure during pregnancy”, “maternal exposure time unspecified”) were excluded from the study cohort.
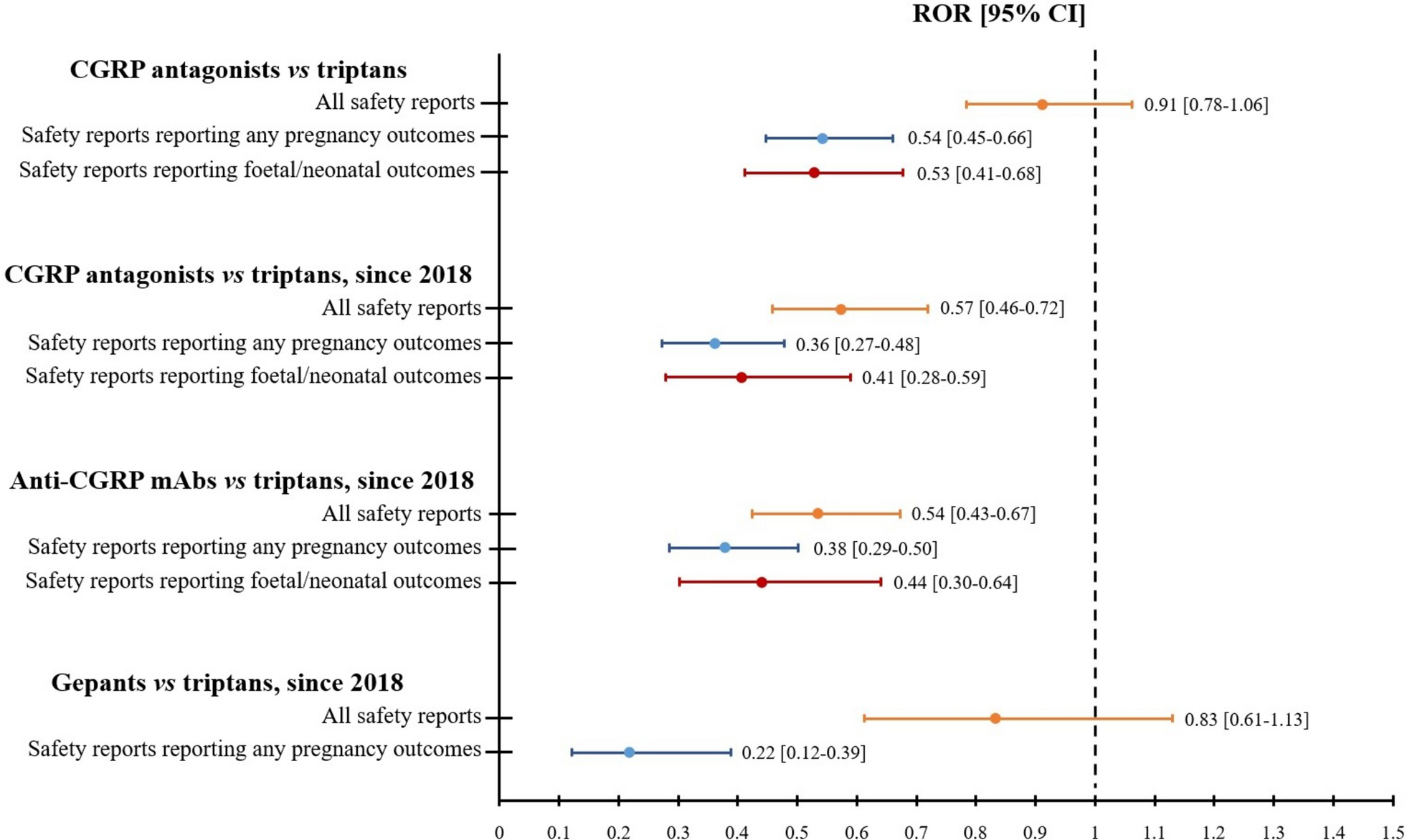
Reporting Odds Ratio (ROR) was used as disproportionality measurement along with its 95% confidence interval (CI) and computed when a minimum number of 5 safety reports of interest was present to reduce the likelihood of false positives [16]. Threshold for the detection of a signal of disproportionate reporting was set with 95% CI lower limit > 1 [16]. The primary outcome was to detect signals of disproportionate reporting for pregnancy exposures to CGRP-A regardless of the reporting of pregnancy outcomes in addition to drug exposure.
The secondary outcomes were i) to detect signals of disproportionate reporting for pregnancy exposures to CGRP-A reporting any pregnancy outcomes (maternal and/or foetal/neonatal); and ii) to detect signals of disproportionate reporting for pregnancy exposures to CGRP-A reporting foetal/neonatal outcomes.
The following sensitivity analyses were performed to control for confounding: i) temporal restriction, starting from 01.01.2018 (when the first in class erenumab received marketing authorization); and ii) temporal restriction and subgroup disproportionality analyses by therapeutic modality (i.e. monoclonal antibodies versus gepants). Data management and analyses were performed with Statistical Analysis System Software (version 9.4; SA Institute, Cary, NC).
According to the Human Research Act (810.30, of 30 September 2011 - status as of 1 September 2023, Art. 2), from the Federal Assembly of the Swiss Confederation, ethical approval and written informed consents were not required.




留言 (0)