
記住我





Between December 2016 and December 2021, a total of 5 patients with inadequate left atrial cuff in 84 consecutive lung transplant procedures were analyzed retrospectively. The study protocol was approved by Local Ethics Committee (No: 2022/11/614). The study was conducted in accordance with the principles of the Declaration of Helsinki.
Donor selectionMatching between donor lungs and the recipient was based on blood group compatibility and predicted total lung capacity (pTLC) by height and age. The criteria for donor selection included PaO2/FiO2 value, smoking history, donor age, chest X-ray, tomography, cultures, bronchoscopy findings and sputum characteristics. We described donor management and the selection process in our previous article [4].
Harvesting techniqueLung procurement and preservation followed standard procedures [5]. Harvest is performed by the harvest team of the transplant center in our country. When the harvest team goes to the donor center, they first perform bronchoscopy. If bronchoscopy is appropriate, the operation phase is started. Lung examination begins with standard procedures. Atelectasis-hematomas are detected and performed in the recruitment maneuver. To evaluate elasticity, the collapse test is performed with the help of anesthesia.
A purse-string suture is placed in ascending aorta and the inserted cardioplegia cannula is fixed with the prepared suture. We insert a cannula into the main pulmonary artery just after the pulmonary valve, allowing drainage of the right and left lungs. The reason why we place it close to the pulmonary valve is that our heart team primarily repairs the pulmonary artery after the cannula is removed so that it does not stay in the anastomosis line of the heart team and sufficient tissue is provided in the heart transplant, avoiding unnecessary shaving. Then, an incision is made with a sharp scalpel in the middle of the purulent sutures in the pulmonary artery, the incision is widened, the cannula is inserted, fixed and then washing is started. While the patient is connected to the ventilator, washing at 5 cm H2O positive end-expiratory pressure ensures that the washing solutions are spread more homogeneously and there is no ponding.
The aortic cross-clamping is then placed and both cardioplegia and pulmoplegia lines are opened. Harvesting is started following the completion of lung and heart washings and cooling. First, the inferior vena cava is dissected up to the right inferior pulmonary vein. The heart is exposed by raising the apex to the cephalad position. After the apex is raised to the cephalad position, the incision made from the middle of the left atrium to the left pulmonary vein is widened with a scalpel by paralleling it to the left pulmonary vein.
The inside of the left atrium is best seen by the surgeon on the donor’s left. The left atrial incision is extended to the intra-atrial groove (Waterson). We do this widening cut from the outside. A distance of at least 1 cm should be left for the heart and lungs in the left atrium with an adequate rim. It is very important not to stretch the heart too much during cutting because if it is cut by pulling too much, there will not be enough lung anastomosis tissue when it is released. Scissors should always be held horizontally. During this time, care should be taken not to cut the pulmonary artery.
The heart should be placed in its neutral position and cut to leave enough aorta and superior vena cava tissue for the heart and the two vessels should be carefully separated from the right pulmonary artery. The pulmonary artery is then divided and ascending aorta divided. Pericardial attachments are dissected and the heart, freed from all connections, is placed on the back table and the heart harvest is completed. The pulmonary artery is then divided. After heart harvest, the bilateral lung is removed unblocked. Then, the lung is placed in an organ protection bag.
Repair and reconstructionIn the presence of an inadequate atrial cuff in its anterior and posterior wall, it was augmented with a donor aortic graft. The entire thoracic aorta was routinely harvested from the donor and transferred with the lung in an organ preservation solution for spare graft tissue that we could use for injuries that might occur during harvest or on the back table. The donor aorta was shaped to complete the deficiency from an undamaged and smooth surface with no outflow of spinal arteries after the aortic arch. On the back table, aortic graft and donor pulmonary vein anastomosis were performed using a 5 − 0 polypropylene running suture to form a separate atrial cuff. The new aortic-cuffed atrium was sutured to the recipient’s atrium using a 4 − 0 polypropylene running suture (Fig. 1).
Fig. 1
Intraoperative photographs showing inadequate left atrial cuff and aortic graft reconstruction. (a) Insufficient left atrial cuff; RPA: right pulmonary artery, LPA: left pulmonary artery, RAt: right atrium, LAt: left atrium. (b) Left atrium repaired with aortic graft, AG: aortic graft, RAt: right atrium
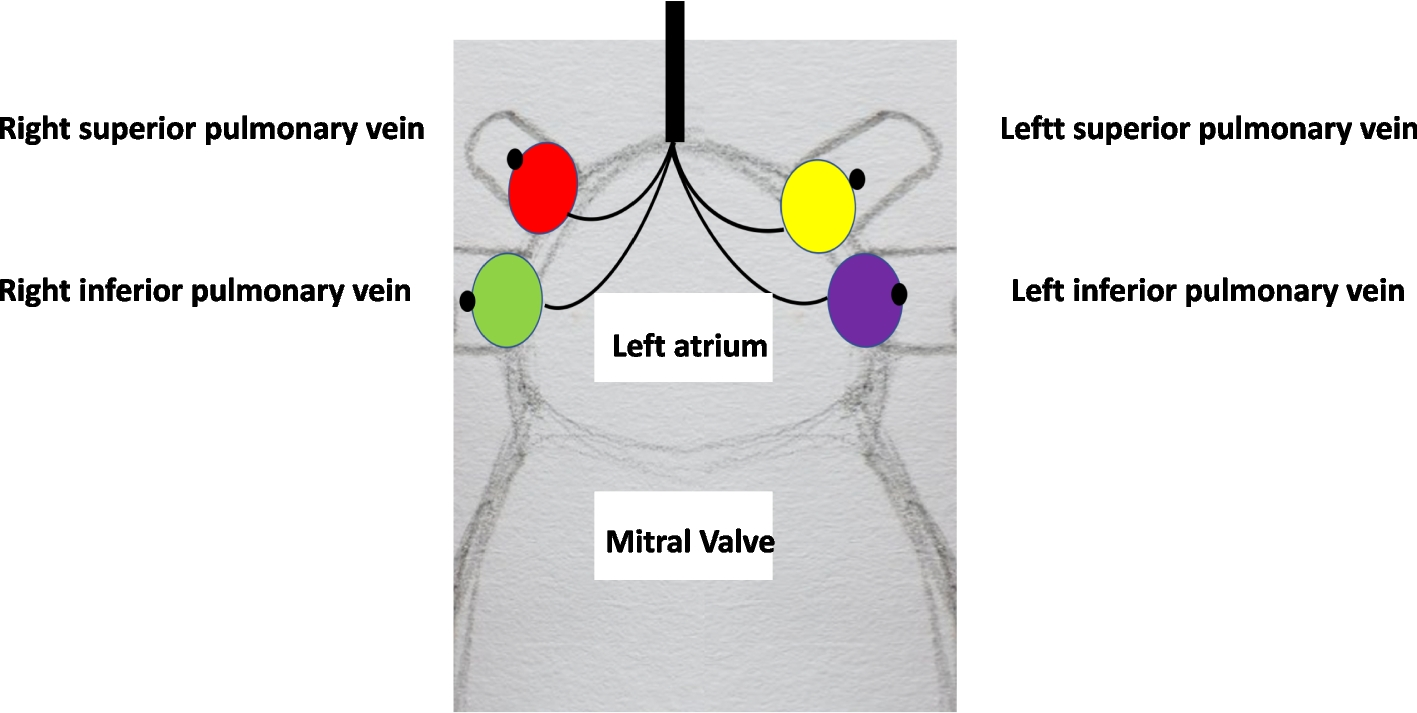
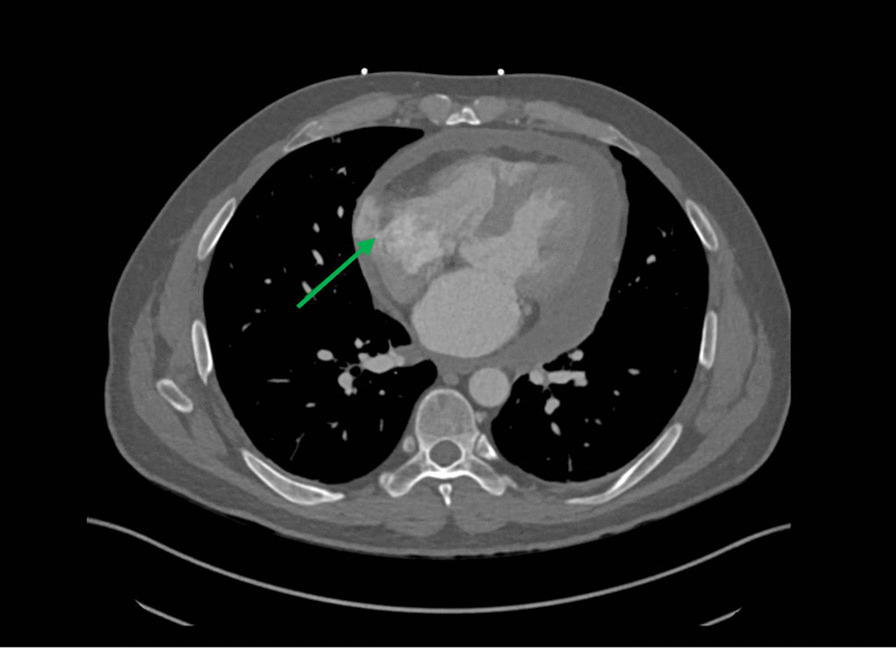
A bifurcated Y-shaped Dacron conduit (Hemagard knitted vascular graft; Maquet) patch was used to separate the superior and inferior pulmonary veins. The anastomosis was performed on the back table by cutting the Dacron graft limb to the appropriate length to obtain the additional length of both the inferior and superior pulmonary veins. The reconstructions were performed using a 5 − 0 polypropylene running suture. Anastomosis between the Dacron graft common body and the recipient’s atrium was performed using a 4 − 0 polypropylene running suture. During the completion of the anastomoses, retrograde and antegrade air evacuation was performed. All anastomoses were then carefully examined to detect any tension, twisting, narrowing, or bleeding. Transesophageal echocardiography was performed perioperatively for anastomosis control and control was obtained with pulmonary CT angiography in the postoperative period (Fig. 2).
Fig. 2
Inadequate cuff, intraoperative photographs showing reconstruction with dacron mash, and postoperative Pulmonary Computed Tomography Angiography images. (a) Insufficient left atrial cuff: RIPV: Right inferior pulmonary vein, LPV: Left pulmonary vein, MPA: main pulmonary artery, RSPV: right superior pulmonary vein. (b) Left atrium repaired with Dacron Mash, RIPV: right inferior pulmonary vein, PV: left pulmonary vein, MPA: main pulmonary artery, RSPV: right superior pulmonary vein, DG: dacron graft. (c) Anastomosis line (arrow) in the third month postoperative Pulmonary Computed Tomography Angiography
Anticoagulant therapy was not given in the patient we used for the aortic graft and acetylsalicylic acid was used in the patient we used for the Dacron mesh.
留言 (0)