
記住我

In practice, the inability to observe supply curves limits the payer’s ability to consider a ‘fair’ price for each medicine independently and provides a rationale for extending the framework to consider a ‘fair’ common price for a unit of health that applies to all medicines collectively.Footnote 2
A collective approach based on a single ‘common price’ has some notable advantages:
1.It provides manufacturers with a clear signal as to the payment they will receive for any additional units of health gain provided by the medicines they develop. This reduces uncertainty as to the manufacturer’s return on investment, which will be considered in Sect. 5.
2.It rewards efficient research and development (R&D). Since manufacturers can ‘price up’ to the common price regardless of their reserve price, they can receive disproportionately large returns if their production costs are low and/or their medicines are highly effective. Conversely, manufacturers who develop costly and ineffective medicines will receive lower returns, disincentivizing inefficient R&D.
In determining a ‘fair’ common price, it is important to consider the total economic surplus arising from all medicines reimbursed at each potential common price, and the distribution of this between patients (consumers) and manufacturers (producers).
4.1 Additional AssumptionsThe collective approach proposed here makes the following assumptions, further to those outlined in Table 1.
1.A single common price for a unit of health, \(\lambda\), is publicly specified by the payer. Given the assumption of a causal relationship between \(\lambda\) and the prices of medicines, reimbursed medicines with a reserve ICER less than or equal to \(\lambda\) are supplied and priced such that the ICER equals \(\lambda\). Medicines with a reserve ICER greater than \(\lambda\) are not supplied.
2.Medicines are considered independent, such that reimbursing (or not reimbursing) a medicine has no impact on the reserve ICERs for other medicines.
4.2 Hypothetical ExampleGiven the confidential nature of manufacturers’ reserve prices in practice, the collective approach will be illustrated using a simple hypothetical example.
There are four medicines, each of which is supplied only if the common price specified by the payer (in £ per QALY) equals or exceeds the reserve ICER reported in Table 2. If a medicine is supplied, it will be reimbursed at the common price and will provide the health gain reported in Table 2. Any costs of reimbursement fall on a public health care budget and diminish the health of other patients; it will be assumed that \(k\) is £15,000 per QALY, in line with UK empirical estimates [16].Footnote 3
Table 2 Hypothetical exampleTo consider the total welfare at any given common price, consumer and producer surplus must both be valued in a common metric. For this, a ‘demand-side’ threshold (\(v\)) is used. Recent work by Woods et al. [17] considered two different values of \(v\): £60,000 per QALY, based on the value of a statistical life year used by the UK Government [18]; and £30,000 per QALY, a value more closely aligned with recent literature [9, 10, 19]. The same approach is adopted here.
4.3 Consumer SurplusTo begin, the consumer surplus will be calculated at different common prices. To illustrate the key insights of this approach, it is sufficient to consider three common prices within the range of reserve ICERs (£5000, £10,000, and £15,000 per QALY, where the last equals \(k\)), as well as a common price below the range of reserve ICERs (£0 per QALY) and one above this range (£20,000 per QALY).
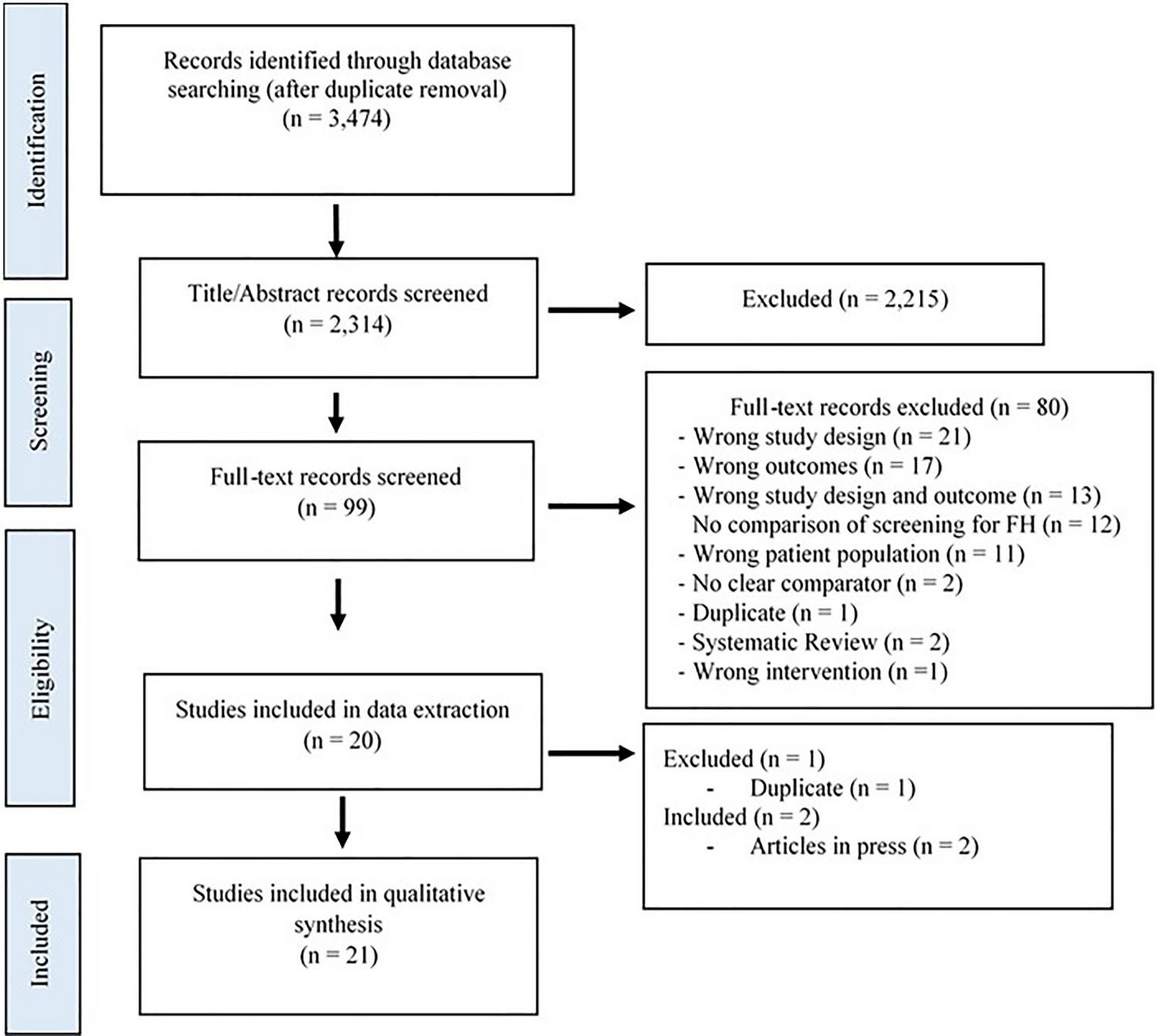
The consumer surplus at each common price is summarized in Fig. 4, with more detailed figures provided in the electronic supplementary material (ESM).
Fig. 4
Consumer surplus at each common price in the hypothetical example. k denotes the health opportunity cost of reimbursing medicines. QALY quality-adjusted life-year
4.3.1 Common Price of £0 per QALYAt a common price of $0 per QALY, no medicines are reimbursed because every reserve ICER lies above the common price. No health gain is provided, but there is also no health loss for other patients, so the net impact on population health is zero. This is illustrated by the grey dot at the origin of Fig. 4 and in the ESM (Fig. 10).
4.3.2 Common Price of £5000 per QALYAt a common price of £5000 per QALY, medicine A is supplied because the common price exceeds its reserve ICER.
The health gain for patients receiving A is 30 QALYs. Although its reserve ICER is £2750 per QALY, it is priced up to the common price of £5000 per QALY. With a health gain of 30 QALYs, and an ICER of £5000 per QALY, it follows that the incremental cost of A is £150,000. Since \(k\) is £15,000 per QALY, the health loss from reimbursing A is 10 QALYs. Reimbursing A at this common price therefore improves population health by 20 QALYs, comprising a 30 QALY gain and a 10 QALY loss.
The remaining medicines are not supplied, providing no health gain but also no health loss. The consumer surplus is therefore 20 QALYs, illustrated by the yellow dot in Fig. 4 and in the ESM (Fig. 11).
4.3.3 Common Price of £10,000 per QALYIncreasing the common price to £10,000 per QALY has two countervailing effects. Medicine B is now supplied and is priced up to £10,000 per QALY. With a health gain of 60 QALYs, and an ICER of £10,000 per QALY, the incremental cost is £600,000. The health loss is therefore 40 QALYs, such that reimbursing B improves population health by 20 QALYs.
However, by increasing the common price, medicine A is now priced up to £10,000 per QALY. Its incremental cost is now £300,000, so the health loss to other patients is now 20 QALYs (compared with 10 QALYs at a common price of £5000 per QALY). Reimbursing A at this higher common price therefore improves population health by only 10 QALYs (rather than 20 QALYs).
Since medicines C and D are not supplied, the total health gain is 90 QALYs and the total health loss is 60 QALYs. The consumer surplus is 30 QALYs, illustrated by the green dot in Fig. 4 and in the ESM (Fig. 12).
4.3.4 Common Price of £15,000 per QALYAt a common price of £15,000 per QALY, medicine C is now supplied and priced up to £15,000 per QALY. With a health gain of 45 QALYs, the incremental cost is £675,000 and the health loss is also 45 QALYs. Reimbursing C has no net impact on population health since the health gain equals the health loss.
Increasing the common price also results in medicines A and B being priced up to £15,000 per QALY. The incremental costs of A and B are now £450,000 and £900,000, resulting in a health loss of 30 QALYs and 60 QALYs, respectively, in each case equal to the health gain. Reimbursing A and B at this higher common price therefore nullifies their net impact on population health.
Medicine D is still not supplied, so the total health gain is 135 QALYs and total health loss is also 135 QALYs, resulting in no consumer surplus, as illustrated by the black dot in Fig. 4 and in the ESM (Fig. 13).
Note that this finding of zero consumer surplus at a common price of \(k\) is generalizable beyond this example: any medicine priced at \(k\) provides no net impact on population health, since the health gains are exactly offset by the health losses. This has critical implications for determining a ‘fair’ common price for medicines in practice.
4.3.5 Common Price of £20,000 per QALYAt a common price of £20,000 per QALY, above the entire range of reserve ICERs, all four medicines are supplied and priced up to £20,000 per QALY; since this exceeds \(k\), all four medicines displace more QALYs through their reimbursement than they provide to patients.
Given their associated health gains (Table 2), the incremental costs are now £600,000 for medicine A, £1,200,000 for B, and £900,000 for each of C and D; the resulting health loss is now 40 QALYs for A, 80 QALYs for B, and 60 QALYs for each of C and D. The total health gain is 180 QALYs and the total health loss is 240 QALYs, resulting in a net loss in population health (i.e. a negative consumer surplus) of 60 QALYs; this is illustrated by the red dots in Fig. 4 and in the ESM (Fig. 14).
4.3.6 Maximizing Consumer SurplusAlthough the greatest consumer surplus in the analyses above arose at a common price of £10,000 per QALY, these five common prices are not exhaustive, and in fact the maximum consumer surplus arises at another common price: £7750 per QALY. This corresponds to the reserve ICER of medicine B, where the consumer surplus is 43.5 QALYs.
It is a general finding that consumer surplus is maximized at a common price below \(k\) corresponding to a reserve ICER for a medicine. The trend in the consumer surplus—initially increasing with the common price, reaching a maximum at a common price below \(k\), then declining to zero at a common price of \(k\)—is also a general finding. These general findings are discussed in Sect. 4.6.
4.4 Producer SurplusThe assumption that manufacturers are unwilling to supply at a loss has the following implications for the producer surplus:
1.If the common price is lower than a medicine’s reserve ICER, the manufacturer will not supply and the producer surplus will be zero.
2.If the common price equals the medicine’s reserve ICER, the medicine will be supplied but the producer surplus will be zero.
3.If the common price exceeds the reserve ICER, the medicine will be supplied and will be priced up to the common price, such that producer surplus will be positive. In this case, producer surplus can be calculated by subtracting the incremental cost of the medicine at the reserve ICER (aggregated over all patients) from the incremental cost at the common price. For example, if the incremental cost is £100,000 when priced at the reserve ICER (where producer surplus is zero) but increases to £300,000 when priced up to a higher common price, the producer surplus is £200,000.
The producer surplus at each common price is summarized in Fig. 5, with more detailed figures provided in the ESM.
Fig. 5
Producer surplus at each common price in the hypothetical example. k denotes the health opportunity cost of reimbursing medicines. QALY quality-adjusted life-year
4.4.1 Common Price of £0 per QALYAt a common price of $0 per QALY, no medicines are supplied because each reserve ICER lies above the common price. Producer surplus is zero, illustrated by the grey dot at the origin of Fig. 5 and in the ESM (Fig. 15).
4.4.2 Common Price of £5000 per QALYAt a common price of £5000 per QALY, medicine A is now supplied. At its reserve ICER (£2750 per QALY), medicine A would have an incremental cost of £82,500. Instead, it is priced up to £5000 per QALY, so the incremental cost is £150,000. The increase in its incremental cost (£67,500) represents the producer surplus accruing to the manufacturer at this common price. Since no other medicines are supplied, the total producer surplus is £67,500, illustrated by the yellow dot in Fig. 5 and in the ESM (Fig. 16).
4.4.3 Common Price of £10,000 per QALYAt a common price of £10,000 per QALY, medicine B is now supplied. Both A and B are priced up to £10,000 per QALY. At their reserve ICERs, the incremental costs of medicines A and B are £82,500 and £465,000, respectively. At this common price, their incremental costs are £300,000 and £600,000, resulting in a producer surplus of £217,500 and £135,000, respectively. No other medicines are supplied, so the total producer surplus is £352,500, illustrated by the green dot in Fig. 5 and in the ESM (Fig. 17).
4.4.4 Common Price of £15,000 per QALYAt a common price of £15,000 per QALY, medicine C is now supplied. Medicines A, B, and C are all priced up to £15,000 per QALY. At their reserve ICERs, the incremental costs of medicines A, B, and C are £82,500, £465,000, and £551,250, respectively. At this common price, their incremental costs are £450,000, £900,000, and £675,000, resulting in a producer surplus of £367,500, £435,000, and £123,750, respectively. Since medicine D is not reimbursed, the total producer surplus is £926,250, illustrated by the black dot in Fig. 5 and in the ESM (Fig. 18).
4.4.5 Common Price of £20,000 per QALYAt this common price, above the entire range of reserve ICERs, all four medicines are now supplied and priced up to £20,000 per QALY. At their reserve ICERs, the incremental costs of medicines A, B, C, and D are £82,500, £465,000, £551,250, and £866,250, respectively. At this common price, their incremental costs are £600,000, £1,200,000, and £900,000 for both C and D, resulting in a producer surplus of £517,500, £735,000, £348,750, and £33,750, respectively. The total producer surplus is £1,635,000, illustrated by the red dot in Fig. 5 and in the ESM (Fig. 19).
4.5 Total WelfareThe consumer surplus calculated in Sect. 4.3 can be converted into monetary terms using the demand-side threshold (\(v\)). The total welfare at each common price is the sum of the monetary value of the consumer surplus and the producer surplus calculated in Sect. 4.4.
Table 3 summarises the consumer surplus, monetary value of the consumer surplus, producer surplus, and total welfare for each common price considered above, for each of \(v\) = £30,000 per QALY and \(v\) = £60,000 per QALY.
Table 3 Consumer surplus (CS), producer surplus, and total welfare, at each common price in the hypothetical exampleIn the example here, for each of \(v\) = £30,000 per QALY and \(v\) = £60,000 per QALY, total welfare is maximized at a common price of £7750 per QALY, below \(k\) and coinciding with the reserve ICER for medicine B; this is summarized in Table 3 and highlighted in bold.
This is a generalizable finding (see Sect. 4.6); under the reasonable assumption that \(v>k\), total welfare is maximized at a common price below \(k\) coinciding with the reserve ICER of a medicine. Note that if \(v\) is only slightly greater than \(k\), the welfare maximizing common price will coincide with the highest reserve ICER below \(k\) (in the example here, if \(v\) = £16,000 per QALY, then total welfare is maximized at a common price of £12,250 per QALY). Where the difference between \(v\) and \(k\) is larger, the welfare-maximizing common price may coincide with another reserve ICER further below \(k\), as in this example where \(v\) = £30,000 or £60,000 per QALY.
It should also be noted that \(v\le k\) is implausible in practice, given the costs associated with administering both taxation and the public health care system, and the unwillingness of individuals to pay as much (or more) in taxes to generate a marginal population QALY as they are willing to pay for a marginal QALY for themselves [20]. Nevertheless, for completeness, the implications of assuming \(v\le k\) are considered in the ESM.
4.6 Generalizable FindingsSome of the findings of the example provided here are generalizable. These are summarized in the following sections and in Fig. 6.
Fig. 6
General shape of the consumer surplus, producer surplus, and total welfare curves, assuming the lower bound of the distribution of reserve incremental cost-effectiveness ratios (ICERs) is zero. λC and λmax represent the common prices that maximize consumer surplus and total welfare, respectively. k denotes the health opportunity cost of reimbursing medicines. If the lowest reserve ICER is above zero, the consumer and producer surplus will be zero for all common prices below that reserve ICER (such that the curves will be flat along the horizontal axis until that point). Alternatively, if the lowest reserve ICER is negative (i.e. there are medicines that dominate their comparator at their reserve price), these will be supplied (and provide a positive consumer and producer surplus) even at a common price of zero, such that the curves both intersect the vertical axis above the origin
4.6.1 Consumer Surplus 1.Consumer surplus is zero at any common price below the lowest reserve ICER of any medicine. This is because no medicines are supplied, so there is no health gain nor health loss, and so no impact on population health.
2.Consumer surplus is positive for common prices above the lowest reserve ICER but below \(k\). Within this range, a marginal increase in the common price may give rise to two countervailing effects:
a.An increase in consumer surplus due to one or more new medicines being supplied since the common price now equals the respective reserve ICER(s). Since these new medicines are priced below \(k\), their reimbursement improves population health.
b.A decrease in consumer surplus due to medicines already supplied being priced up to the new common price, diminishing population health.
At low common prices, where few medicines are supplied, the first effect generally outweighs the second, so a marginal increase in the common price improves consumer surplus (such that the green curve in Fig. 6 slopes upwards).
As the common price (and the number of medicines supplied) increases, the relative magnitude of the second effect grows, eventually equalling that of the first. At this common price (denoted as \(_}\)), the consumer surplus is maximized and the green curve in Fig. 6 peaks. This point always corresponds to the reserve ICER of a medicine.Footnote 4
At common prices above \(_}\) but below \(k\), marginal increases in the common price result in a declining (but still positive) consumer surplus, with the second effect outweighing the first (causing the green curve in Fig. 6 to slope downwards).
3.At a common price of \(k\), the consumer surplus is zero. This is a critical finding and arises because the health gains from any supplied medicines are exactly offset by the health losses that result from their reimbursement. The green curve in Fig. 6 intersects the horizontal axis at this point.
4.Above a common price of \(k\), consumer surplus is negative, and becomes more negative as the common price is increased. This is because all medicines are priced sufficiently highly that their health gains are outweighed by the health losses resulting from their reimbursement, and because any new medicines supplied as a result of increasing the common price are also priced such that they diminish population health outcomes.
4.6.2 Producer Surplus 1.Producer surplus is zero at any common price below the lowest reserve ICER of any medicine. This is because no medicines are supplied.
2.For common prices above the lowest reserve ICER of any medicine, producer surplus unambiguously increases as the common price increases. This is due to two complementary effects:
a.An increase in producer surplus due to one or more new medicines being supplied since the common price now meets or exceeds the respective reserve ICER(s).
b.An increase in producer surplus due to higher pricing for medicines already supplied, which are now priced up to the new common price.
4.6.3 Total Welfare 1.Where \(v>k\), total welfare is maximized at a common price at or above \(_}\) but below \(k\), coinciding with the reserve ICER for a medicine. This is plotted as \(_}\) in Fig. 6.
2.If \(v\) is only slightly greater than \(k\), the welfare maximizing common price coincides with the highest reserve ICER below \(k\). If \(v\) is considerably greater than \(k\), the welfare maximizing common price may coincide with another reserve ICER further below \(k\).
4.7 Establishing a ‘Fair’ Common PriceAs in earlier sections, a ‘fair’ price requires that consumer and producer surplus are both positive. When pricing medicines collectively, consumer and producer surplus are both positive at all common prices greater than the lowest reserve ICER of any medicine but below \(k\).
Nevertheless, an important finding of the framework is that consumer and producer surplus both increase up to a common price of \(_}\), so there is mutual interest in setting the common price at least as high as \(_}\). The most relevant range for establishing a ‘fair’ common price is therefore between \(_}\) (where consumer surplus is maximized) and \(k\) (where consumer surplus is zero).
At any ‘fair’ common price, there will generally be some medicines with low reserve ICERs for which the manufacturer receives substantial profits, and others with higher reserve ICERs for which most of the economic surplus for that medicine is allocated to patients. This is inevitable when setting a single common price for all medicines collectively. There will also generally be medicines with reserve ICERs above the common price but below \(k\). This raises a number of issues and is considered further in the ESM.
留言 (0)