This is a systematic review and meta-analysis of whether AE has a positive impact on the treatment of chronic musculoskeletal disorders, the results of the study showed that patients who performed AE showed considerable improvements in pain, physical function, and quality of life compared to those who did NE. In the meantime, AE showed a more significant improvement in the vital indicator of pain compared to patients conducting LE but did not show a remarkable advantage in terms of physical function and quality of life. Nevertheless, our review of the included literature showed that overall, the initial number of participants was lower [26] and the rate of follow-up missed during the intervention was higher [11] in the LE group compared to AE, suggesting that patient engagement is higher in AE than in LE and that the effectiveness of an intervention is based on the efficacy of the intervention itself combined with patient engagement, so that subject engagement is critical in assessing the final effect. This is because even if an intervention is very effective, it will not show much of a benefit if the patient's willingness to participate is weak.
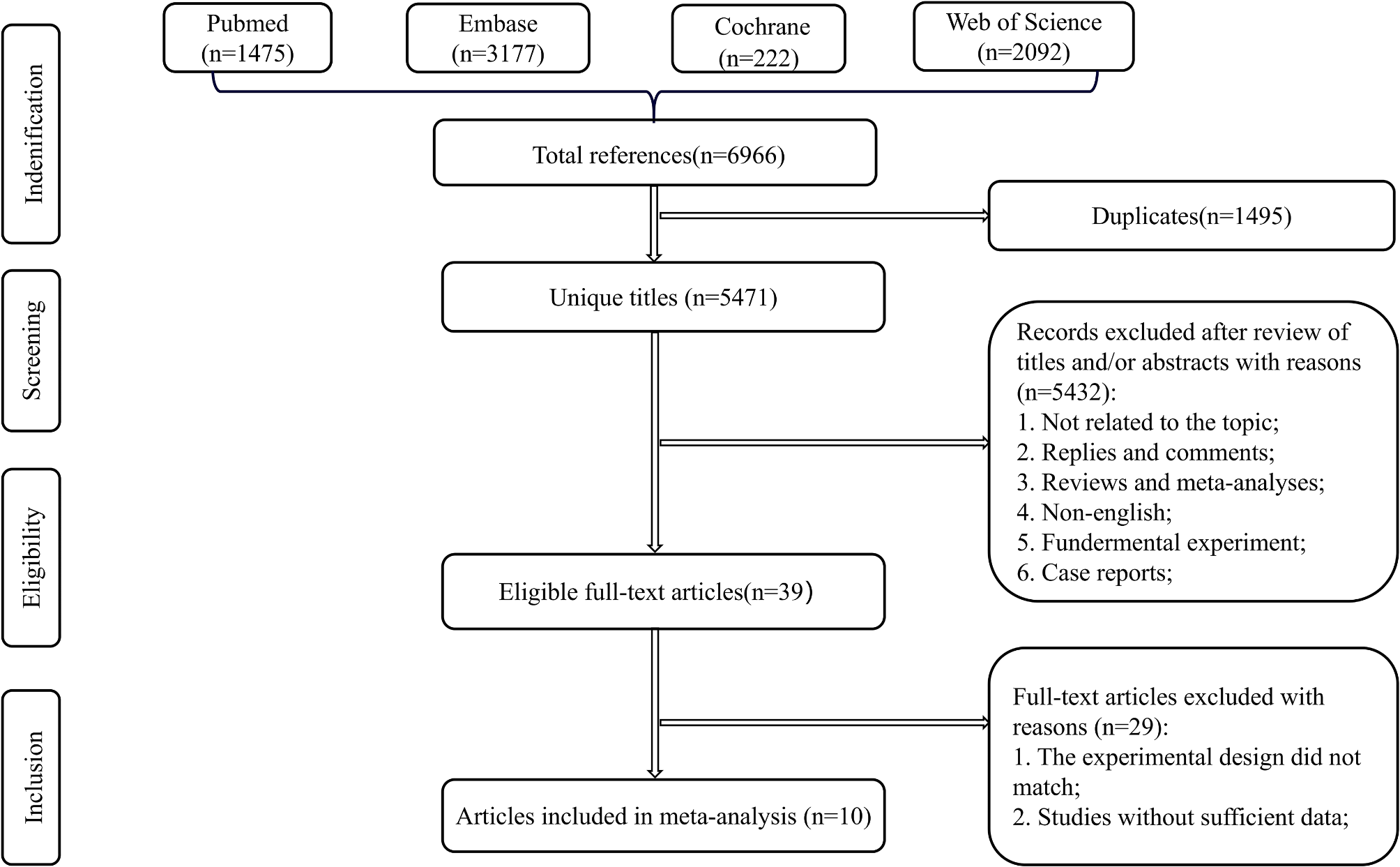
From the authors' investigation, there have been no previous studies on whether AE can improve chronic musculoskeletal disorders, thus this is the first systematic review and meta-analysis of this disease. Meanwhile, we selected important indicators such as pain, physical function, and quality of life, which have a high assessment value for patients' activities of daily living, to ensure the scientific accuracy of the study. Moreover, the total number of patients included in this study was 2200, and the advantage of a large population base makes the study results more credible. Besides, we included and summarized multiple types of chronic musculoskeletal disorders, which makes the study results more applicable to a wider population.
Impact of AE on pain
The study used a pain assessment scale that allowed the assessors to determine whether AE had a positive impact on the improvement of pain values. The combined results showed that in a comparative analysis of AE versus NE and LE, AE was found to have a significantly better improvement in pain values than NE and LE. Also, the corresponding subgroup analysis showed that in all subgroups, the comparison between AE and NE showed a statistical difference, which can be interpreted in light of how AE affects the process of pain production. Pain is a sophisticated physiological phenomenon and as the main clinical manifestation in patients with osteoarthritis, fibromyalgia, etc., it is generated for complex reasons. In the normal population, the central nervous system balances the level of excitation and inhibition, so that no pain is generated, but in patients with chronic pain, this balance is disrupted [49]. In Baraniuk's study [50], it is known that the MEAP (Met-enk-Arg6-Phe7) in the cerebrospinal fluid of patients with fibromyalgia and low back pain compared to the normal group concentrations were significantly altered, and this suggests that altered levels of central nervous system opioid may cause or exacerbate fibromyalgia. Therefore, the consumption of opioids before and after the intervention can be used to determine the degree of pain reduction or worsening [51].
It is well established that physical exercise, a cost-effective and safe rehabilitation therapy, reduces pain levels by enhancing neurological 5-HT (5-hydroxytryptamine) neurotransmission, decreasing 5-HT transporter protein expression, and increasing 5-HT receptor expression through low-intensity aerobic training [52]. One step further, physical exercise in an aquatic environment may be more beneficial for pain relief. The pain-relieving effect of AE may stem from the combined effect of exercise, warm water, and buoyancy on thermoreceptors and mechanoreceptors [17], water pressure, water viscosity, and water temperature stimulate the senses during AE, promoting the triggering of thermoreceptors and mechanoreceptors and blocking the conduction of nociceptors (nociceptors are small-diameter nerve fiber endings that respond to the tissue environment) [53]. At the same time, the temperature and pressure of the water stimulate the skin, and while submerged in water, methionine encephalin plasma levels rise and reduce plasma levels of β-endorphin, corticotropin, and prolactin [53]. It deserves to be mentioned that the process of muscle activity produces several cytotoxic substances, the continuous accumulation of which activates sensitizes, or awakens nociceptors thereby producing pain, cytotoxic substances including histamine, serotonin, bradykinin, adrenaline, etc. [54], some research has reported increased levels of glutamate in fibromyalgia patients, which as a neurotransmitter transmitting pain stimulates the nociceptors, while the bradykinin stimulates the release of norepinephrine and prostaglandins to sensitize the nociceptors further. Hence, the improvement of pain can also be explained by the mechanism that the association of water pressure and temperature produces competing stimulation of nerve endings [55], thus being able to reduce injury from the periphery, and that hydrotherapy can also relax muscles, reduce their tension and decrease pain.
Effect of AE on physical function
In assessing this indicator of patients' physical function, the majority of studies used the SF-36 (Medical Outcomes Study 36-Item Short-Form Health Survey) scale [12, 22, 28, 29, 31, 48], while some of them chose the WOMAC (Western Ontario and McMaster University Osteoarthritis Index) and FIQ (Fibromyalgia Impact Questionnaire) scales [30, 37, 44]. Because the assessment scales are much more similar, the results are also more accurate. Physical function is significant as an important indicator to evaluate the effect of AE on patient improvement. Patients with chronic musculoskeletal disorders show low physical function in several aspects, for instance, patients with fibromyalgia syndrome are prone to fatigue and dyspnea, which may be related to changes in the respiratory system, and according to clinical observations, patients have lower respiratory muscle endurance, inspiratory muscle strength, and chest mobility [56]. It was also found that the patient's heart rate was significantly elevated, cardiovascular sympathetic nerve activity showed increased, vagal nerve activity decreased, and the regulation of the sinus node was reduced, and thus, improving the patient's physical function was most significant in improving cardiovascular and respiratory function. Several studies have demonstrated that aerobic exercise can improve neurological disorders as well as cardiopulmonary function [57] and that the aquatic environment can reduce cardiovascular stress in patients, allowing for more intense training. A study by Zamunér et al. [58] demonstrated that aquatic therapy not only increased patients' aerobic capacity but also improved cardiac autoregulation; meanwhile, it was also reported in the paper that AE increased patients' oxygen uptake at rest and during exercise, as evidence of a certain degree of improvement in cardiopulmonary function [59].
For the subgroup analysis of physical function, AE compared with NE showed statistically significant differences in all subgroups. Therefore, this result further suggests that AE has a significant improvement in physical function compared to NE in most categories of chronic musculoskeletal disorders. While the comprehensive results of AE compared to LE showed no statistical difference, this result suggests that AE and LE are similar in terms of their effectiveness in improving the physical function of patients. When comparing the intervention methods of the studies in each group, it was found that more trials provided more differences in the training programs for AE and LE. The differences are not limited to the training period and intensity, and the variations in the training program will have an impact on the final results, so more research is needed to verify the final results of AE and LE.
Impact of AE on quality of life
Quality of life is a very sophisticated metric that assesses a wide range of aspects, including patient mood, fatigue, perceived ability, and mental health, all of which can influence a patient's ability to live a normal life. Given the complexity of this index, the scales used to assess patients' quality of life varied across studies, and we, therefore, included the corresponding data by selecting scales with relatively similar assessment methods and criteria after due consideration. Quality of life is the best indicator of a patient's normal life, so the emphasis on improving the quality of life for patients is overwhelming. With AE intervention, warm water can put the patient's muscles in a relaxed state and reduce the pressure of gravity on the joints, in addition, exercise can promote the release of β-endorphin and dopamine in the patient's body [60], β-endorphin is a kind of endogenous morphine-like substance in the human body, which has a strong analgesic effect, dopamine is the most abundant catecholamine neurotransmitter in the brain, which transmits signals of excitement as well as happiness, and it plays an important role in human movement and learning. The increased release of these two substances has a calming and analgesic effect on the subjects, as well as relieving anxiety and achieving the effects of antidepressants. In the meantime, the aquatic environment provides a relaxing and comfortable atmosphere for patients, which can increase their pleasure [28], relieving their depression or irritability caused by their disease and the pain it brings. Besides, water exercise can also be considered as a kind of water immersion method, which affects some physiological responses of the body, such as changing the fluid in the cells and blood vessels, reducing edema, increasing blood flow by diastole, and increasing cardiac output, which can relieve fatigue and have psychological benefits for the participants [61].
The meta-analysis of the quality of life indicator showed a significant improvement in AE compared to NE, but no statistically significant difference when compared to LE, which may be due to the short intervention period in some of the studies resulting in similar changes in various aspects of the subjects, as a result, no significant difference could be revealed between the two programs. Meanwhile, we also found statistics showing that patients with osteoarthritis have lower physical mobility compared to the general population, and nearly 50% of patients will be reluctant to perform additional exercise training due to pain [14, 62]. So there is a problem of low patient willingness to treat and low participation rate, while the level of participation of patients in both groups will also affect the final results. Subgroup analysis showed that the low back pain subgroup showed no statistical difference in the AE versus NE comparison, and this is most likely due to the small number of literature with two articles, which makes it biased from the actual situation.
Limitations and future research
There are several limitations of this systematic review and meta-analysis. Firstly, this study only included RCTs published in English, and some high-quality articles published in languages other than English were excluded, so future meta-analyses should include these excluded high-quality articles as well as some valuable studies that may not have been published yet; secondly, because the number of included literature within some subgroups was found to be small when subgroup analysis was conducted in this study, which could lead to a large heterogeneity in some subgroup analysis and make the results of meta-analysis differ from the actual results. Thus, the number of included literature should be increased as much as possible in future studies to further improve the reliability of the study; the third is that the intervention protocols are not identical across studies, so the intervention intensity, as well as the intervention period, can vary, both of which can affect the final intervention effect; in the fourth, there is a placebo effect for aquatic therapy, and most of the literature included in this paper lacked a placebo control, so the placebo effect could not be excluded [33].
Considering the limitations mentioned above, future meta-analyses should carefully consider the period of interventions included in the paper, either too long or too short could adversely affect the final results, and the intensity of interventions needs to be kept as similar as possible between studies, in addition to further evaluation of the placebo effect of AE to determine whether it affects the results and to what extent. In other words, most of the AE therapies in the studies included in this article require the supervision of professional physiotherapists and the development of exercise programs for patients that are appropriate to their physical conditions, but there is still much space to improve the popularity of AE because of the limited space and related exercise facilities available for AE. Therefore, in the foreseeable future, more achievable and affordable AE programs should be developed for the stakeholders to increase their popularity, allowing patients to receive treatment in a safer and more comfortable environment, reducing pain, and improving their quality of life. Moreover, since AE applies to a wide range of groups and there are some differences in treatment measures and contraindications among different diseases, it is recommended that future studies should address individual differences and disease differences. For instance, AE showed significant improvement in physical function compared to NE in patients with osteoarthritis and fibromyalgia, but not in patients with low back pain. Therefore, it is essential to develop exercise programs for different patients that match their intervention objectives, physical conditions, and personal activity habits to maximize patient participation and intervention effects [63].
Given the positive relationship established in this meta-analysis that AE has a positive effect on the treatment of chronic musculoskeletal disorders compared to NE, future research is required to explore whether there is a positive effect of AE in areas other than the indicators studied here. Moreover, AE has been found to have a significant improvement in pain compared to LE in patients with chronic musculoskeletal disorders, but the efficacy has not yet been demonstrated in terms of physical function and quality of life, so more studies are needed to compare its efficacy in other aspects.





Comments (0)