LSG failure generally falls into two categories [5, 12]: WLF (either IWL or WR) and GERD. Recent long-term studies of pLSG show higher than expected failure and revisional surgery rates with incidence of WR ranging from 14 to 37%. The pooled revision rates due to WLF and GERD were estimated as 13.1% and 2.9%, respectively [4, 6, 7, 39]. This study focused on two types of revisional procedures post-LSG failure in terms of WL and did not include post-LSG complications.
Multiple explanations have been speculated regarding the GT dilation. Most primary dilation cases are probably due to technical failure during pLSG with incomplete resection of the gastric fundus [12,13,14,15,16, 19,20,21, 40]. Many studies reported that incomplete fundus removal could be the actual cause of the detected dilated fundus and described that complete dissection of the fundus posterior aspect may be technically demanding and almost impossible in some extremely obese patients [20, 40]. In some cases of incomplete fundus removal, a small HH may not be identified during the pLSG, in which some gastric folds may be missed [16, 19, 20, 41]. Secondary GT dilation is usually due to false calibration with a large bougie during pLSG or due to the physiologic GT dilation [12,13,14,15,16, 19,20,21, 40]. Based on radiological studies using CT volumetry, a RGV threshold of 250 cm3 has been proposed as a possible indication for ReLSG below which the conversion to a malabsorptive BP is encouraged [16, 42, 43].
Revisional surgery is often burdened by higher rates of complications [13, 17, 44] and no standardized guidelines have been developed in literature for choosing a RBS after SG failure [13, 15, 17, 45, 46]. In patients with severe GERD symptoms (the main cause for revision), literature confirmed that RYGB should be the ideal option [4, 13, 17, 46]. In compliance with this, we excluded severe GERD patients from having these procedures.
ReLSG has been proposed as a feasible RBS after pLSG failure when a residual fundus is evident or when the GT shape suggests an improper technique [13,14,15,16,17,18,19,20,21]. Some short-term papers reported good WL results comparable to RYGB [41, 47]. Ambiguous data have been reported about ReLSG complications [15]; some series [16, 47] reported high GL rates, while others [21, 41] did not report any. ReLSG offers several advantages (compared with malabsorptive procedures) that encourage its practice: less technically challenging nature of procedure, increased restriction, decreased acid production, maintaining GI continuity, avoiding dumping and decreased risks of anemia, osteoporosis, protein and vitamin deficiency [15,16,17, 20, 21, 40, 48]. The negative effects of ReLSG include the increased risk of gastric leak (GL), the high-pressure system leading to onset/aggravation of GERD. Other disadvantages include the absence of malabsorptive effect and the resleeved GT being prone to re-enlargement with time causing insufficient WL with higher probability of long-term WR [4, 13, 15, 17, 40, 41, 46].
After failure of the restrictive SG, adding malabsorption has been proven an effective means for further WL [4, 13, 17, 22, 23, 46]. OAGB has been introduced and established as a viable alternative to the classic RYGB due to its relative technical simplicity, shorter learning curve and the ease of reversibility [1, 24,25,26,27,28,29,30,31,32]. Long-term studies demonstrated OAGB as an efficient primary BP that provides durable WL with acceptable complication rates [24,25,26,27,28]. Studies comparing primary OAGB to RYGB revealed some advantages with OAGB, such as shorter OT, fewer major complications (leakage and IH) and equal or even higher efficacy in WL [29,30,31,32]. Furthermore, OAGB, specifically with a 200-cm BPL, is believed to cause marked fat and sweets intolerance and is more malabsorptive than standard RYGB owing to its longer BPL, without reaching the malabsorptive dangers of BPD/DS [23, 35,36,37,38, 48,49,50,51].
Recently published systematic reviews and meta-analyses showed that RLOAGB is a valuable choice after failed restriction and that SG conversion to OAGB was technically easier [37, 49,50,51,52,53,54]; this would be particularly useful in handling revisional surgery and could be helpful in higher BMI patients. These studies demonstrated better WL and acceptable incidences of the main complications with RLOAGB compared to those of RYGB.
The current concerns existing for OAGB are the risks of postoperative malnutrition and bile reflux (BR) [25, 29, 36, 53, 55]; both are still debated [53,54,55]. Symptomatic BR, requiring revision, has been reported [23, 27, 36, 38]. Felsenreich et al. [50] study revealed better outcomes for OAGB than for RYGB in terms of acid exposure, even though more OAGB patients suffered from GERD symptoms; this may be a hint for the symptoms not being acid-based, but related to BR. The YOMEGA study [29] reported more reflux in the gastric pouch in RLOAGB compared to RYGB without difference in quality of life (QOL). While De Luca et al. [25] showed that the rates of symptomatic BR were lower than first feared. Tolone et al. [56] study showed significant anti-reflux effects of OAGB compared to SG. A comparative study [31] did not show procedure-specific advantages in GERD remission.
Two recent meta-analyses [53, 54] showed that OAGB has different effects on GERD where GERD resolution after converting restrictive surgery to OAGB was described by some studies, while others described de-novo emergence of GERD and BR in patients with no preoperative GERD symptoms. However, the incidence of severe BR requiring conversion to RYGB was low. In addition, most symptomatic patients experienced marked improvements by medications [53, 54].
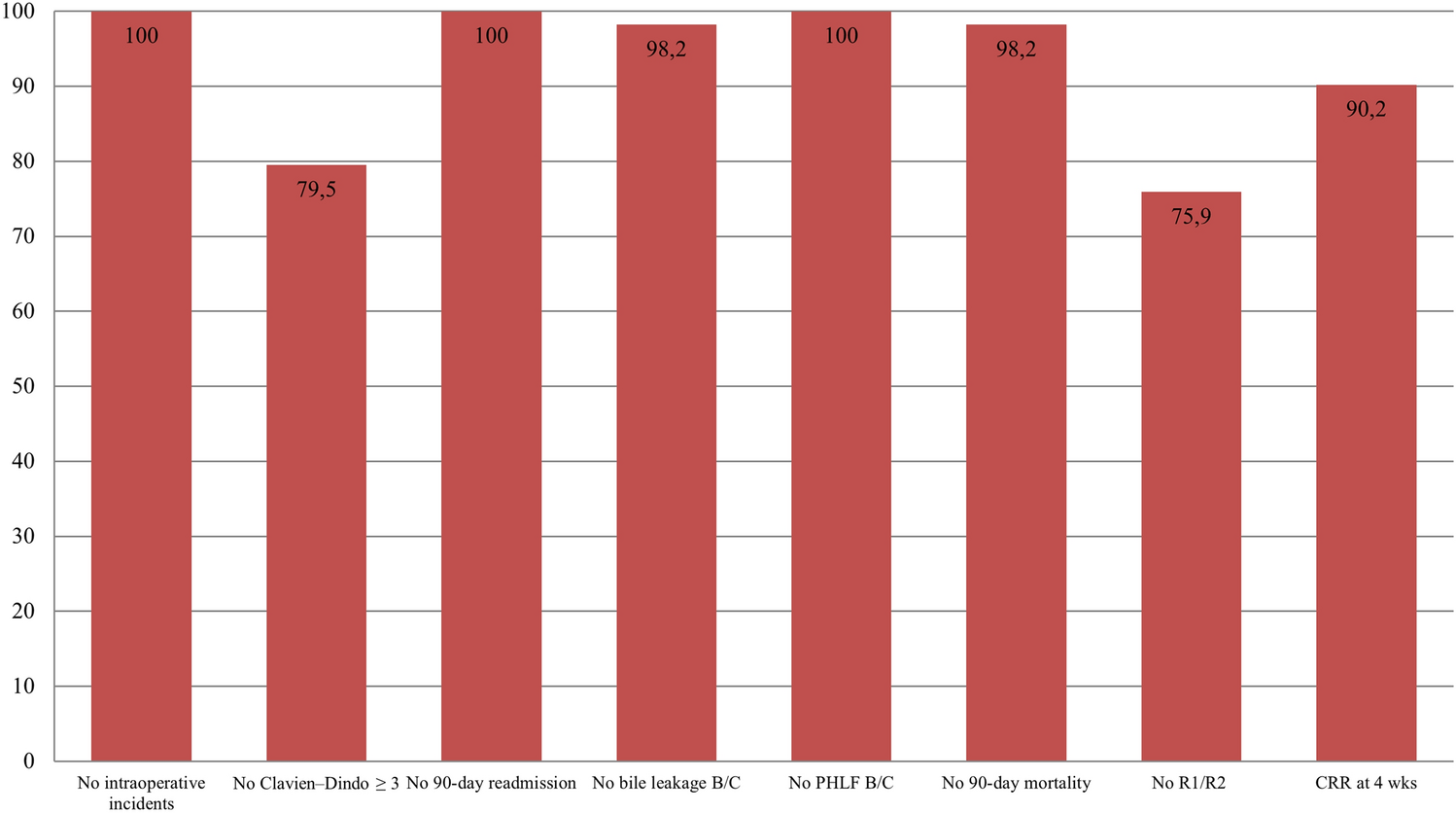
In our study, three patients in each group (12% with RLOAGB and 11.1% with ReLSG) encountered seven postoperative intra-abdominal complications. Significant hemorrhage occurred in three patients (two with ReLSG and one with RLOAGB). With RLOAGB, two patients (8%) had anastomotic leakage. With ReLSG, also two patients (7.4%) had GL. Leakage cases were managed successfully with adequate drainage and optimization of general conditions. Our complications rate was considered relatively high when compared to other similar studies; this may be explained by the wide variability in experience of the operating surgeons. AlSabah et al. [41] and Omarov et al. [21] studies showed no early postoperative complications with ReLSG while Antonopulos et al. [47] series showed GL of 8.2%. With RLOAGB, Chiappetta et al. [37] and Jamal et al. [34] s


留言 (0)