This study tested the hypothesised conceptual model and devised a final structural equation model for the effects of psychosocial factors and DPR variables on oral health impact. The two-step approach in SEM guided modifications of the initial model to the final model with path coefficients for direct and indirect effects, including the mediation of variables on the outcome.
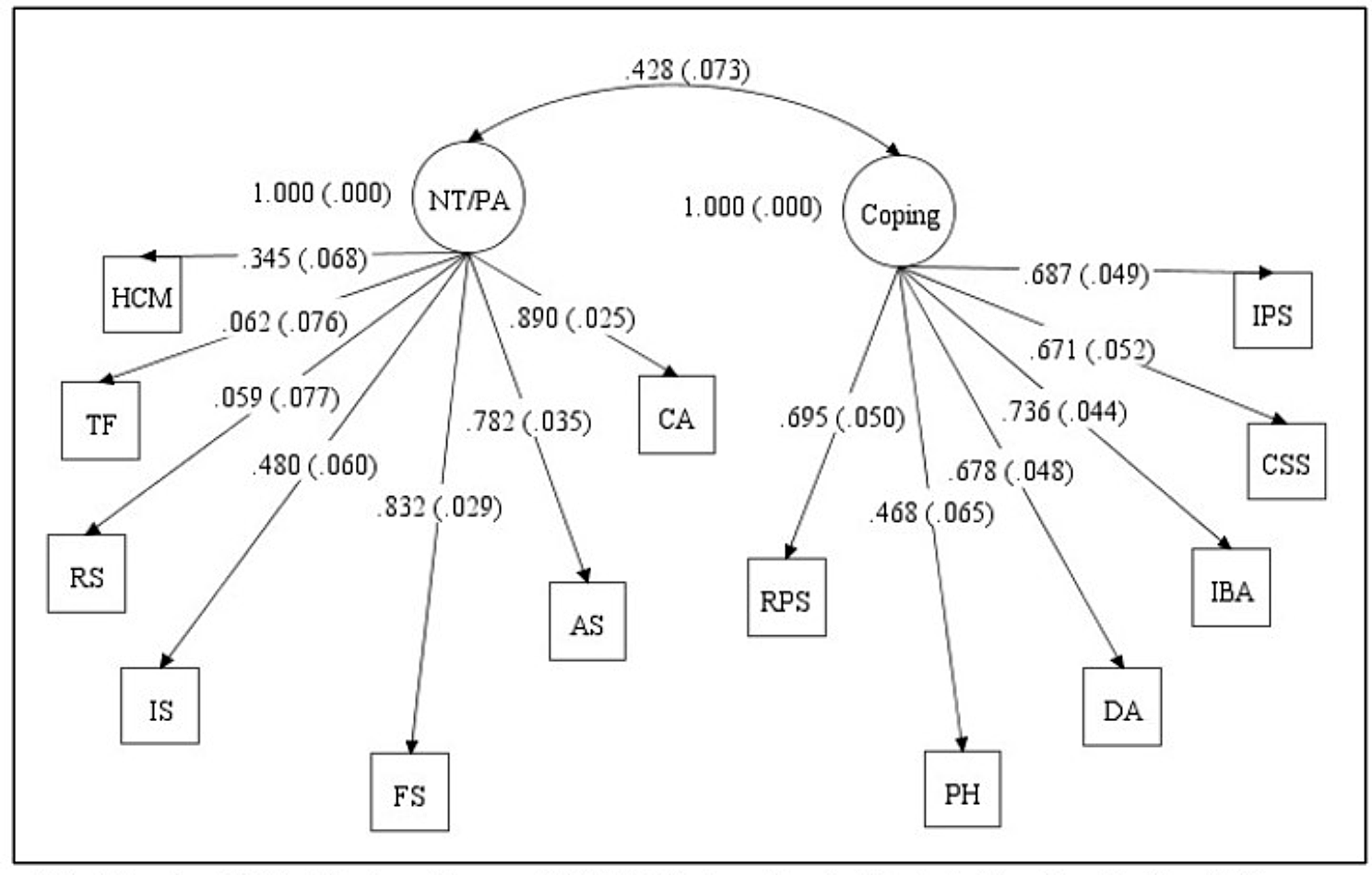
In the first step of SEM, CFA led to measurement models with satisfactory fit indices consisting of each latent variable from each psychometric scale. The results were similar to the findings of previous structural validation between trust and satisfaction with minor variations from different approaches [14]. Reverse-coded items were deleted for low factor loadings from multi-item scales for the acceptable model fit in the first place. Further modifications were predicated on the exclusion of thematically less relevant items and the addition of covariance between analogous items. Those principles were consistently found in CFA for the psychosocial domain, not least self-efficacy, as all items reversely worded were dropped and highly correlated items either deleted or drawn with covariance.
The main concept of the framework, ‘distal-to-proximal’ associations, was supported by the final structural model. Psychosocial factors had indirect effects on oral health impact via DPR variables as mediators, along with their unique contributions of direct effects. The rationale of the ‘proximity’ concept can also be countenanced by the larger effect sizes of DPR variables – the more proximal domain to the outcome. The total effects of DPR variables (|β| from 0.14 to 0.19 in Table S5) were much larger than that of more distal psychosocial factors (|β| from 0.01 to 0.12). This mechanism was also demonstrated within the same DPR domain. Trust, as for the general dental context (e.g. trust in general dentists), was entirely mediated by satisfaction and dental fear, as in specific clinical settings (e.g. satisfaction with the dental care at the last visit and fear with a descriptive/evocative question of clinical practice) [9]. Therefore, the theory-based framework suggested in the introduction is empirically verified.
For detailed tests of hypotheses and paths of variables, all differences from the initial conceptual model were observed in the psychosocial domain. Well-being was directly associated with OHIP, losing the hypothesised paths to satisfaction and trust. The association of social support was drawn with satisfaction instead of trust initially presumed. Self-efficacy had an additional association with trust in company with a direct effect on OHIP. The positive/negative directions of the paths were all as expected in the hypotheses except for the inverse correlation between well-being and social support. In general, better psychosocial and DPR variables led to lower dental fear and oral health impact. The individual total effects of predictors on the outcome were also in agreement with the findings from the literature review [3,4,5, 9, 15, 34]. Well-being and self-efficacy were significantly and substantially associated with OHIP (β = − 0.12 and − 0.10 in Table S5), whereas social support was associated with a significant yet negligible amount (β = − 0.01) similar to weak or non-significant results from previous studies [3,4,5]. Satisfaction and dental fear directly accounted for a considerable amount of variance in OHIP (β = − 0.14 and 0.19, respectively), whereas trust contributed only as an indirect effect. The mediation of trust by satisfaction has already been hypothesised [9] and reported to affect the compliance [35] and loyalty [36] to their physician. Despite its sole indirect associations, trust had a comparable size of the total effect on OHIP (β = − 0.15), which warrants the importance of trust for OHRQoL along with satisfaction and fear.
Multi-group analyses of the final model achieved consistent model invariances across different groups of participant characteristics aside from the ‘last dental visit’ variable. The characteristics in the tests were selected considering the substantial role of SES as a determinant of health [1, 3, 5] and dental service variables for oral health-specific outcomes [3, 5, 9, 15]. For those whose last dental visit was 12 months ago or more, paths with statistical significance in difference showed higher coefficients together with similarly greater β in four paths out of the remaining six (Table S6). Inasmuch as two thirds (65.0% in subsample A) of those whose last visit was less than 12 months ago were for regular check-ups, non-regular dental patients are likely to put more weight on psychosocial and DPR variables for OHRQoL. This claim may need to be verified as a priori hypothesis from this secondary interpretation.
This study has some limitations. First, the direct/indirect effects in the final model need to be interpreted with caution due to the nature of the cross-sectional data. For example, the effect of well-being on OHRQoL can be interpreted in reverse, as those with oral health impact/conditions tend to feel lower satisfaction with life, as reported [37]. Second, a few important variables as either predictors or confounders were missing in the conceptual diagram. Both positive traits and negative aspects of psychosocial factors are supposed to be related with oral health outcomes such as psychological stress [3, 4, 7]. In the DPR domain, communication and patients’ involvement in clinical encounters are considered essential [11, 12] other than those included. Although invariance tests were performed on SES characteristics, income and education may need to be incorporated as functional components in the model for their potential confounding. Next, modified psychometric scales for each latent variable in the CFA may represent slightly different or more specific constructs compared with pre-validated original scales. For example, a modified oral health impact may not comprehensively represent the outcome of the original OHIP-14 by losing some dimensions initially conceived. In this regard, parcelling or total summed scores of items in path analysis can be supplementarily considered for robust results. Finally, data collected entirely from self-complete questionnaires are inherently subject to method biases in empirical studies. Despite our efforts with imputed composite scores to minimise the consequences of CMB, acquiescence bias and social desirability bias might have influenced the results. Also, slight differences in sociodemographic characteristics in the study sample compared to the population data might have resulted in higher trust and satisfaction for females and the elderly, and lower trust for the individuals with higher education, to a limited extent considering the absolute sample size [9]. The results of the study may also need to be interpreted considering these differences.
The findings of the study have several practical implications. The final model shows that psychosocial and DPR values at clinical encounters can contribute to the improvement of oral health outcomes. For example, instead of didactic chairside oral hygiene instructions, a programme to establish a trustful relationship in dental encounters and improve oral health literacy for patients’ health self-efficacy can be more beneficial. Subjective psychosocial factors may need to be considered as much as objective socioeconomic determinants to understand the social gradient of health [3]. This can be vindicated by the common risk factor approach [38] that psychosocial values can be applicable to extensive social milieu as determinants beyond oral and general health. Further studies are advised to establish rigorous causality in a longitudinal design and the general application of the findings to different/diverse outcomes in relevant fields.



Comments (0)