
記住我
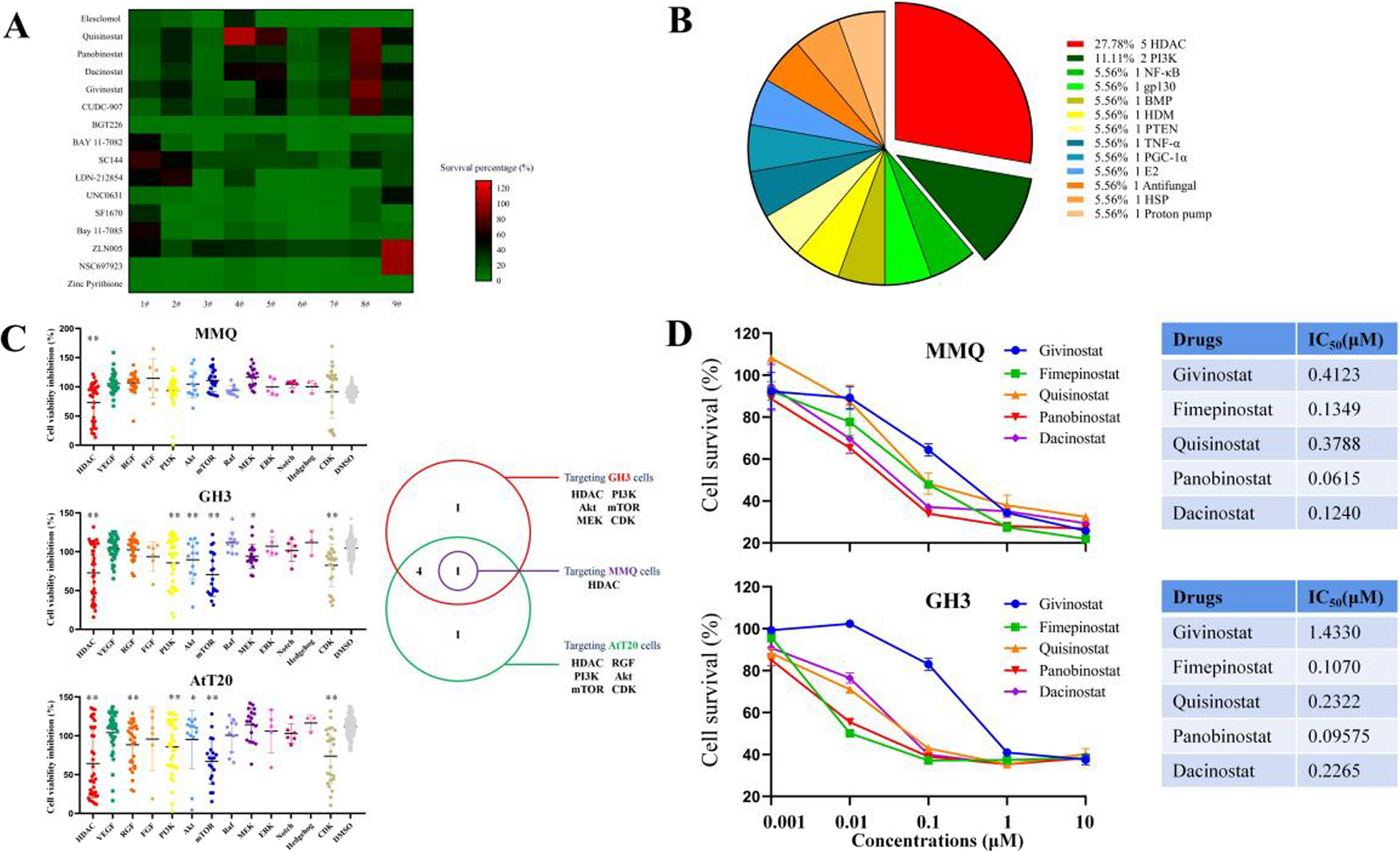
Status quo pathologic workflows assess second resections for presence of atypical cells concerning for proliferative cancer growth and measuring abundances of immune cells and necrosis. We sought to first validate the influence of proliferative stem cell and immune cell activity on survival outcomes in patients experiencing glioblastoma recurrence following primary surgical management with chemoRT. To achieve this, we clustered pathologically confirmed recurrent GB RNAseq samples from the CGGA using an 83-gene signature matrix based on current literature to identify whether (i) recurrent glioblastoma patients clustered into gene signature-defined subpopulations and (ii) determine the extent to which such subpopulations would exhibit differential survival activity (Additional file 1: Table S1; S11). kMeans clustering grouped patients into 3 subpopulations (Fig. 1a). We validated the statistical significance of these groupings by measuring the within cluster distance and between cluster distance of our actual dataset against a scrambled randomized dataset (Additional file 1: Fig. S4; p < 0.001). Kaplan–Meier analysis demonstrated overall patient survival among clusters significantly varied (Fig. 1b). Patients in CGGA cluster 1 (blue) exhibited significantly poorer survival outcomes to those in CGGA clusters 2 and 3 (green and red respectively) (p = 0.0012). Specifically, an approximately 5-month median survival difference was present between CGGA cluster 1 and CGGA clusters 2 & 3 [dotted line]. These results highlight that specific gene signatures related to immune cell activity and cancer cell proliferation both (i) cluster recurrent glioblastoma patients into distinct subpopulations which (ii) exhibit differential survival activity.
Fig. 1
Progressive GB clinical outcomes are driven by variations in tumor immune response and cancer cell replication. (a) kMeans clustering of recurrent GB samples based on select gene expression profile. (b) KM curve survival of patients based on cluster. (c) xCell based cell enrichment scores of clusters. (d) Term specific xCell enrichments. (e) WGCNA module eigengene score and representative term based on cluster. (f–h) Process-specific eigengene scores. Initial comparisons were screened by ANOVA and t tests were used for specific groupings: *p ≤ 0.05, **p ≤ 0.01, ***p ≤ 0.001, ****p ≤ 0.0001
While our previous results highlighted the validity of applying proliferative stem cell and immune cell markers to stratify patients, we wished to better understand the driving processes behind CGGA cluster 1’s poor survival and evaluate whether other concurrent biologic processes or molecular functions not represented in our 83-gene signature were varied. All assessed genes [n = 23,987] were passed through both xCell and WGCNA to assess for processes not highlighted in the original 83-gene signature analysis. With respect to immune enrichment, T-cells, myeloid cells, and lymphoid progenitors varied amongst clusters (Fig. 1c). Specifically, significant enrichment in the overall immune score was present in CGGA cluster 3 when compared to either CGGA clusters 1 or 2. Moreover, common lymphoid progenitors (CLPs) or macrophages were most elevated in CGGA cluster 3, but cluster 1 did show a slight increase in enrichment to cluster 2 (Fig. 1d). Taken together, these data demonstrate that CGGA cluster 3 shows strong immune involvement in the tumor microenvironment, with CGGA cluster 1 showing some immune enrichment to a lesser extent but still greater than cluster 2—highlighting a reduced, but active immune involvement in our poor surviving patients. We conclude that these three clusters of glioblastoma patients show differential survival and differential immune cell deconvolution.
With respect to other biologic processes however, WGCNA was used to group genes into color modules based on similar co-expression patterns and related to biologic processes or molecular functions using gene ontology. Quantitatively, module expression is represented by an eigengene value taken from the first principal component of all genes within a module. Through this approach, relative elevation of an eigengene score based on a clinical phenotype against compared groupings signifies enrichment for the represented process among the differentially regulated genes. Amongst those with significant GO enrichment, all modules listed below navajowhite1 showed significant variation across clusters (Fig. 1e). Notably, modules related to immune response [navajowhite1, lightyellow, plum2, lightgreen] consistently showed the highest eigenscore in CGGA cluster 3 (Fig. 1f). However, RNA/nucleobase metabolism [yellow, cyan] or cell cycle activity [pink, honeydew1] showed highest elevation in eigenscore in cluster 1 (Fig. 1g, h). It was additionally noted that when assessing overlapped genes related to lymphocyte (GO:0046651) or macrophage (GO:0061517) proliferation, genes represented in our cell cycle color modules showed little overlap while immune process color modules contained several immune proliferative markers (Additional file 1: Fig. S5). Based on these observations, it became more apparent that while cluster 2 & 3 spatially varied in the tSNE plot, the stratification was associated with immune-based signatures but did not correlate with differential survival between these 2 CGGA clusters. However, in the case of cluster 1 which showed the poorest mean overall survival, while some degree of immune activity was evidenced in the analyses, the strongest processes associated in this group included cell cycle activity—as captured in our 83-gene signature—but also active cellular metabolism. We conclude that cluster 1 recurrent glioblastoma patients show enrichment in cellular proliferation and biosynthesis pathways.
Glioblastoma progression and pseudoprogression can be largely stratified by overall cellular proliferation or immune response present in novel lesionsThe neuropathological workflows deployed for the diagnosis of PD versus psPD has been highly debated within the community. The main objective of the neuropathological evaluation is to determine the extent to which novel contrast enhancing lesions are due to reactive changes or neoplastic processes. The workflow performed at our institution is highlighted in Fig. 2a. Although our CGGA findings support that differential survival outcomes are present by assessing cell cycle, metabolism, and immune response signatures in novel lesions, psPD involvement was not assessed within the dataset. Turning to samples retrospectively assessed at James Cancer Center/OSU, we sought to both (i) confirm the efficacy of our disease management of novel enhancement lesions by comparing survival outcomes of patients defined as psPD or PD by the neuro-oncologists, and (ii) objectively assess whether cases reviewed by neuropathology could be stratified by cell cycle, metabolism, and immune response signatures molecularly.
Fig. 2
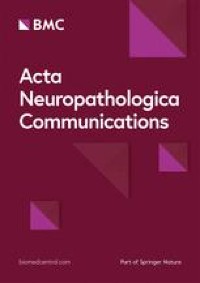
Immune and proliferative stem cell-related signatures accurately distinguish PD and psPD events. (a) IHC representation of pathology utilized to best differentiate PD and psPD. (b) KM survival of GB patients based on PD (n = 27) vs psPD (n = 21) designation following second surgery. (c) Volcano plot differential gene expression of cancer signature based on PD (left) and psPD (right). (d) Gene ontology representation of enriched psPD (left) and PD (right) pathways from differential analysis. (e) IPA network summary of enriched pathways for PD (blue) and psPD (orange) with driving markers based on differential expression analysis. (f) Unsupervised kMeans clustering of samples based on top 150 DEGs from bulk analysis. (g) Enhancement status pseudo-coloring of PD (red) and psPD (blue) in previously clustered cases. Arrows represent samples showing admixed pathology taken for spatial analysis. (h) Distribution of clinical diagnosis within clusters identified in tSNE map. (i) Representative IHC imaging from single case highlighting areas of atypical cellularity (recurrent) and immune infiltration (reactive) within a single lesion. Chi-square: X.2 = 16.11, p = 5.95e-05
As neuropathological guidelines for assessing PD and psPD are ill-defined, final diagnosis by neuro-oncology was used to set our ground truth to group our pathologic specimens. Comparing patient samples used in our accompanying molecular studies, patients designated as psPD showed significantly higher median survival times nearing 5 months following second surgery—with more patients designated as psPD surviving during the duration of the study (Fig. 2b; p = 0.036). Although retrospective, these results highlight the point that using our current neuropathology diagnostic approach in stratifying patients does capture patients who are likely experiencing psPD and who have more favorable prognoses. To compare processes separating PD from psPD (as defined by clinical neuro-oncology), 48 samples were evaluated by bulk gene expression using the nCounter PanCancer360 assay—a gene expression test composed of probes that quantify cancer proliferative and/or immune signature-related genes. This assay’s compatibility with FFPE tissue permits incorporation into current neuropathologic workflows. Differential expression analysis highlighted proliferative/stem cell markers including MKI67 and Sox11 in the direction of PD, while immune signaling markers such as CCL20, ILR2, and CXCL8 were in the direction of psPD (Fig. 2c). In psPD patients, GO terms highlighted several processes focused on neutrophil/myeloid activation and immune signaling. In contrast, GO terms found in PD patients focused on cell division and cell cycle activity (Fig. 2d). This is further recapitulated in ingenuity pathway analysis (IPA), as enriched terms to psPD represent several immune response pathways driven by TREM1, TNF, IFNG, IL1, and IL6 while PD was primarily demarcated by E2F-mediated cancer activity (Fig. 2e). Together, these results highlight the capacity of stratifying PD and psPD using traditional immunohistochemistry (IHC) approaches by focusing on pan-immune activation in psPD events.
To better assess the predictive capability of these markers, top 150 differentially expressed genes (DEGs) were extracted and used to cluster samples in an unsupervised fashion based on their gene expression profile as measured by the nCounter assay (Additional file 1: Fig. S2). Overall, kMeans analysis identified 2 statistically significant clusters (Fig. 2f; Additional file 1: Fig. S6; p < 0.001). Distribution of PD and psPD related to cluster identity with PD cases representing 85% of cluster 1 and psPD cases representing 77% of cluster 2 (Fig. 2g, h; X2 = 16.11, p = 5.95e-05). This in-silico analysis furthers the point that such stem cell proliferative/immune signatures hold promise in group stratification. However, for cases which clustered near/in the opposing side, it was noted that samples displayed a mixed tissue histology of both immune infiltration and concerning cancer stem cell-like proliferation (Fig. 2i). Thus, intra-lesion heterogeneity may underscore the failure of our clustering to fully stratify both populations. In conclusion, stratification of novel enhancing lesions using cancer-immune signatures successfully stratifies most PD and psPD cases; however, a rarer subset of patients does not fit this approach due to high levels of tissue heterogeneity that obfuscates bulk gene expression analyses.
Immune infiltration abundance and cell morphology separate PD and psPDIn our experience, up to a third of cases present as a mix of treatment effect and tumor which may lead to discordant clinical-pathological correlation [6]. We therefore sought to identify how well our histological approach to stratifying PD and psPD could be identified in specimens that showed marked morphological heterogeneity. To do so, eight samples were selected with tSNE map location in areas where both PD and psPD cases sat in close proximity—highlighting similar expressional profiles (Fig. 2g; arrows). All samples were additionally pathologically confirmed to show mixed presentation and collected for representative H&E, p53, CD163, Ki67, and Olig2 imaging in regions defined by neuropathologist observers as (i) “control” brain (characterized by quasi-normocellular gray or white matter), (ii) “inflammatory” immune reactive brain (characterized by hypercellular gray or white matter without significant neoplastic cells noted on the morphological and immunohistochemical biomarker workup), and (iii) “hypercellular” recurrent cellularity brain within a sample (defined as hypercellular gray or white matter showing neoplastic cells based on the morphological and immunohistochemical biomarker workup) (Fig. 3a; Additional file 1: Table S2). While all samples showed mixed presentation, a ground truth PD or psPD status was designated based on retrospective neuro-oncologic diagnosis [quoted name of regions (“control”, “inflammatory”, and “hypercellular”) will be used to distinguish histology against novel enhancement status outcome (PD, psPD) from here on].
Fig. 3
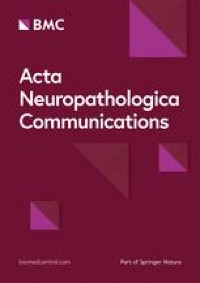
Abundant immune infiltration is preserved in psPD events in spite of admixed presentation. (a) Representative 40 × histology of captured regions of interest showing admixed presentation in a sample. (b) Nearest-neighbor distance schematic of segmented nuclei from hematoxylin layer of H&E images among (c) novel enhancement status and (d) status sub-stratified by tissue histology. (e) DAB to hematoxylin staining ratio calculation schematic using image thresholding for Ki67, p53, and Olig2 while CNN-based segmentation was applied for CD163. Staining ratios among (f) novel enhancement status and (g) status sub-stratified by tissue histology. t test: **p ≤ 0.01, ***p ≤ 0.001, ****p ≤ 0.0001. Mixed effect modeling was additionally performed with post-hoc p value correction. All comparisons in bolded red represent preserved significance with mixed effect correction
We quantified the histologic variation in 8 samples showing heterogenous histological architectures within our workflow by measuring (i) overall tissue cellularity, (ii) IHC staining used in the original neuropathological workflow, and (iii) cell morphology variation based upon ground truth clinico-pathologic designation using automated image analysis workflows. To compare the overall cellularity present between PD and psPD events, H&E images were assessed using a nearest neighbor distance calculation. This approach was accomplished through automated image deconvolution and segmentation of hematoxylin+ nuclei to calculate mean distance of a nuclei from its hundredth nearest neighbor (Fig. 3b). It was found that the mean 100th nearest neighbor distance of segmentations did not significantly vary between PD and psPD events (Fig. 3c). However, when stratified by histology, PD events showed significantly reduced distances in “control” and “hypercellular” regions, while psPD showed reduced distance in “inflammatory” regions (Fig. 3d). It was important to however note the expansion of sample size due to replicates for histologic regions. In consequence, linear mixed effect modeling was performed to control for replicate bias and measure the effect of both our disease status and combined disease status plus histology subtype groupings to our measured outcome. Mixed effect ANOVA highlighted no significant effect of enhancement status to nearest neighbor distance [p = 0.65, η2 = 0.04], but a significant effect when enhancement status and histology were evaluated together [p = 0.03, η2 = 0.03] (Additional file 1: Table S3). Due to the small effect however, post-hoc testing for mixed status and histology groupings did not see preservation of significance in Fig. 3d. Our findings thus suggested that overall presentation of cellularity between PD and psPD events did not vary between groups due to differential cellularity in histologic regions in mixed samples.
We next quantified staining in our samples using a DAB to hematoxylin pixel ratio calculation (Fig. 3e). Total DAB+ pixels were divided by hematoxylin+ pixels in an image to generate a staining ratio which would control for variable cellularity between collected images and pixel size of images. Notably, neither Ki67 nor Olig2 showed significant differences in staining ratio between novel enhancement statuses; however, both p53 and CD163 showed increased staining ratio towards psPD (Fig. 3f). Staining ratio was additionally assessed between histologic subtypes (Fig. 3g). Neither Ki67 nor Olig2 were found to show significant differences in IHC staining in “inflammatory” and “hypercellular” regions. Moreover, mixed effect ANOVA showed no significant effect on staining ratio for status or combined status plus histology groupings in Ki67 and Olig2 (Additional file 1: Table S3). In contrast, p53 showed significant elevations in “control” and “inflammatory” regions, but not in “hypercellular” sites where the stain is applied to evaluate cancer cell mutations. Moreso, enhancement status showed no significant effect on p53 staining ratio [p = 0.2, η2 = 0.26], but significant effect by status and histology [p = 1.4e-5, η2 = 0.09] (Additional file 1: Table S3). Assessment of histology however showed p53 staining in absence of nuclei with atypical Olig2 staining and Ki67 staining (Additional file 1: Fig. S7). In contrast, both PD/psPD status and combined status with histology showed significant effect on CD163 staining ratio [Status-alone: p = 2.2e-16, η2 = 0.44; Status-Histology: p = 2.2e-16, η2 = 0.02]. A strong effect of enhancement status to CD163 staining was thus highlighted as CD163 was shown to have significant staining elevation among all histologic subtypes in the direction of psPD. Post-hoc testing additionally found significance was only preserved between pairwise groupings in CD163 [Bonferroni corrected p < 0.0001 in all groupings] (Fig. 3f, g). Thus, while the dominant staining of CD163 was present in psPD events, we conclude that standard IHC biomarkers are minimally effective to confidently claim a lesion as psPD.
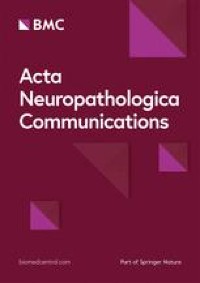
It was additionally apparent that morphologic variability was present across stains (Additional file 1: Fig. S7). We assessed morphologic variation within stains by generating cellular clusters based on cell morphology-extracted features and measured whether the distribution of these morphologic subpopulations varied between PD and psPD. We accomplished this by evenly extracting 16,000 segmented cells from both PD and psPD events from hematoxylin and other IHC stains to cluster samples based on their cell morphology features using UMAP (Fig. 4a). Across stains, multiple clusters were generated with variation from an even distribution (Fig. 4; dotted line). Interestingly, across all stains we found significant distribution changes based on chi-square analysis [Hematoxylin: X2 = 11.88, p = 0.0026; Ki67: X2 = 1828.8, p < 2.2e-16; p53: X2 = 2136.8, p < 2.2e-16; Olig2: X2 = 107.59, p < 2.2e-16; CD163: X2 = 399.13, p < 2.2e-16], but the degree of deviation from even distribution varied. Within hematoxylin+ segmentations, only 3 clusters were identified with the majority of nuclei falling into cluster 1 (large round nuclei) and 2 (slim ellipsoid nuclei). Additionally, a slight increase of psPD distribution was represented in cluster 3 which represented smaller nuclei with variable shape (Fig. 4b). Similarly, within Olig2+ segmentations, while several clusters were identified the predominance of nuclei fell within clusters 1 and 2 (round nuclei reminiscent of oligodendrocytes with variable size) which showed close-to even distribution. However, two subpopulations in cluster 4 and 5 representing small, variably shaped nuclei were shown to have slight increase in psPD distribution as well (Fig. 4e). In contrast, Ki67, p53, and CD163 generated several clusters with many smaller clusters omitted due to the rarity of segmentations present in those groups. Within Ki67+ segmentations, the majority of nuclei grouped into cluster 1 (large, abnormally shaped nuclei reminiscent of cancer cells) which predominately was composed by PD samples. However, both cluster 2 and 4 (smaller, round nuclei morphology reminiscent of immune cells) showed a heavy predominance from psPD events (Fig. 4c). In p53+ segmentations however, distribution of several clusters (clusters 1, 2, 4, and 5) were all shown to be primarily from PD related events with highly irregular morphology reminiscent of cancer cells. Only cluster 3 (rounder nuclei morphology) was observed to predominately originate from psPD events (Fig. 4d). Finally in CD163+ segmentations, the predominance of cells were found in cluster 2 (large branching cells with highly variable shape) with a slight predominance toward PD; moreover, smaller clusters from 3, 5, 6, and 7 showed similar distributions with overall similar morphology to cluster 2. However, other small clusters (1 and 4) showed stronger predominance of psPD with morphology showing smaller punctate staining with variable shape (Fig. 4f). Overall, hematoxylin was observed to have the least morphologic clustering while other IHC stains generated several morphologic subclusters. Interestingly though, within our analysis it was seen that several clusters—particularly those from Ki67 and p53—showed subpopulations of nuclei with distinct morphologic features that more predominated in PD or psPD events. In consequence, while the overall staining of IHC markers targeting proliferative cancer cells was not significantly varied between novel enhancing events, morphology of segmented cells may help identify subpopulations that vary between groups. While these findings support the ability to stratify populations using our current histology workflow, the challenge for a pathologist will likely increase due to the high background staining found within CD163 coupled with the need to annotate rare morphology to accurately find landmarks representative of PD and psPD.
Fig. 4
UMAP clustering of IHC stained cell morphology. (a) UMAPs of segmented cells based upon cell morphology features with accompanying cluster distribution of segmentations from PD (red) and psPD (blue) events for (b) hematoxylin, (c) Ki67, (d) p53, (e) Olig2, and (f) CD163. Representative cell morphology for each cluster is shown to the right of UMAPs. Expected even distribution of diagnosis is represented by the dotted line. Chi-square.: Hematoxylin: X2 = 11.88, p = 0.0026; Ki67: X2 = 1828.8, p < 2.2e-16; p53: X2 = 2136.8, p < 2.2e-16; Olig2: X2 = 107.59, p < 2.2e-16; CD163: X.2 = 399.13, p < 2.2e-16
Cancer immune activity varies in PD and psPD events despite admixed histologyAlthough our image analysis found the preserved efficacy of CD163 immune abundance and use of morphologic variation to stratify novel enhancing lesions, the inability to stratify whether cancer cells present in tissue are proliferating prevent a pathologist from confidently claiming a lesion as psPD. We sought to identify more objective differences between PD and psPD related samples by assessing the spatial variability of expression signatures with respect to the histologic regions shown in Fig. 3a to uncover novel molecular changes across histology. Using the same 8 mixed samples from our image analysis, we immuno-fluorescently labeled slides to identify areas of immune infiltration (CD68+) or stem cell presence (Sox10+) coupled with overlayed clinical IHC imaging to generate RoIs in “control”, “inflammatory”, and “hypercellular” histology regions (Fig. 5a; gray circles).
WGCNA assessed whether known or novel biologic pathways or molecular functions varied between groups and were consistently changed irrespective of histology. It was seen the primary processes which varied amongst sampled regions included nerve/glial cell development (turquoise, pink), biosynthesis/metabolism (greenyellow, magenta, brown), and immune processes (red) (Fig. 5b). Specifically, nervous system development related modules significantly increased in PD events compared to psPD event in “control” and “hypercellular” regions within the turquoise module. Additionally, “inflammatory” regions displayed increased eigenscore in the pink module for PD (Fig. 5c). Overall, these findings support true PD processes show increased cellular differentiation with particular regard to glial populations (pink) in not only “hypercellular” regions concerning of cancer recurrence, but also sites which may appear as more normal “control” brain or largely “inflammatory” under histology. This point is furthered when evaluating more biosynthetic/metabolically relevant modules, with particular regard to the greenyellow module. Irrespective of histology, PD had significant increased eigenscore for cellular biosynthesis (greenyellow) (Fig. 5c). Interestingly, converse elevation in immune activities (red) was not significantly varied in either “control” or “hypercellular” histology and, in fact, significantly elevated in the PD cases for “inflammatory” histology (Fig. 5c). Mixed effect ANOVA demonstrated across color modules that no significant main effect on eigengene score was seen with status alone, but significant effect was present with status and histology combined (Additional file 1: Table S4). Post-hoc testing however found that several pair-wise groupings did not retain significance, but magenta module eigengene differences in “hypercellular” regions between PD and psPD approached significance [Bonferroni corrected p = 0.07] and red module eigengene differences in “inflammatory” regions remained significant [Bonferroni corrected p = 0.005] (Fig. 5c). Taking these observations, elevations in biosynthetic activity in “hypercellular” regions for PD trended but were limited by sample size. Elevation in immune system processes for PD in the inflammatory region may indicate fundamentally different immune pathways present in psPD inflammatory regions.
Fig. 5
Admixed novel enhancement lesions are stratified by immune cell subtype infiltration. (a) Representative capture schematic of GeoMx machine. Gray circles represent locations of RoI collection. (b) Representative enriched GO term in WGCNA color modules with (c) eigengene score compared across histologic subtypes. Differential analysis of PD and psPD events with respect to (d) “hypercellular” and (e) “inflammatory” histology. (f) Overall immune population comparison among stratified groups. (g) Specific boxplot comparisons of clusters for neutrophil enrichment, naïve CD8 T-cell enrichment, non-classical monocyte enrichment, and macrophage enrichment. Initial comparisons were screened by ANOVA and t tests were used for specific groupings: *p ≤ 0.05, **p ≤ 0.01, ***p ≤ 0.001, ****p ≤ 0.0001. Mixed effect modeling was additionally performed with post-hoc p value correction. All comparisons in bolded red represent preserved significance with mixed effect correction
As WGCNA did not show a global elevation in immune response within psPD events across histology, we posited that the lack of congruency between our findings may be due to differential infiltration of immune cells between groups. Although CD163 was noted to be significantly enriched in “hypercellular” events towards psPD, the log change was relatively low (Fig. 5d). In contrast, markers of immunosuppression polarization in myeloid cells were observed to be enriched in “inflammatory” PD events including TREM2, APOC1, APOE, and LGALS3 (Fig. 5e; [51]). “Control” regions showed fewer significantly enriched genes, but neuronal markers such as ENO2 were seen elevated towards PD (Additional file 1: Fig. S8). To examine this further, immune deconvolution was performed over the dataset to evaluate predicted immune infiltration across these groupings (Fig. 5f). Particular variation was present among neutrophil, monocyte/macrophage, and CD8 T-cell populations (Fig. 5g). To be specific, both “control” and “hypercellular” regions had elevated neutrophil enrichment in psPD cases when compared to PD cases of matching histology. Furthermore, “inflammatory” regions showed enrichment of CD8 T-cells in psPD events, while enrichment for monocyte/macrophage populations was elevated in PD events. Mixed effect ANOVA additionally found that enhancement status alone did not have significant effect on immune enrichment, but significant effect was present in combined status and histology groupings in our particular cell populations (Additional file 1: Table S4). Post-hoc testing highlighted mixed effect-corrected significance was maintained in neutrophils in “control” regions [Bonferroni corrected p = 0.047], non-classical monocytes in “inflammatory” regions [Bonferroni corrected p = 0.024], and macrophages in “inflammatory” regions [Bonferroni corrected p = 0.0002] for Fig. 5g, Overall, while a global elevation in immune response was not seen across histology for psPD, psPD displayed elevations of certain cellular population such as neutrophils amongst specific histologic regions. Moreover, while a surprising elevation in immune response was detected in PD events, our results highlighted a domination of myeloid enrichment with biomarkers associated with pro-tumoral polarization. In summary, despite the blunted efficacy of our cancer-immune signatures in admixed tissue samples, significant variation in immune microenvironment activity in spite of similar histology is present between PD and psPD.
留言 (0)