
Remember me










Canada spends less of its total health budget on primary care than the average among Organisation for Economic Cooperation and Development (OECD) countries (5.3% v. 8.1%).
Canada can learn lessons to inform policy on primary care from OECD countries like the United Kingdom, Norway, Netherlands and Finland where more than 95% of the population has a regular primary care clinician or place of care.
An analysis of these countries shows that those with high rates of primary care attachment have stronger contractual agreements and accountability for family physicians, including where they practise, their scope of practice and who they accept as patients.
Countries with high rates of primary care attachment have similar numbers of family physicians, but fewer work in walk-in clinics or specialized areas; family physicians are paid by capitation or salary, work in interprofessional teams and have excellent digital tools and information systems.
Health systems with strong primary care have better outcomes, lower costs and better equity.1 Yet, even at the outset of the COVID-19 pandemic, about 17% of people in Canada reported not having a regular primary care clinician.2 At the same time, Canada is seeing declining enrolment in family medicine as a specialty among medical students,3 and more graduating family physicians are choosing not to practise generalist office-based care.4 The pandemic added further strain, spurring some family physicians to retire early,5 a phenomenon not unique to Canada.6
To distill lessons for Canadian policy on primary care, we identified Organisation for Economic Co-operation and Development (OECD) countries with historically high rates of primary care attachment, compared related health system factors and identified strategies these countries use to achieve high attachment. These lessons range from how health systems are organized to specifics on how primary care is funded, supported and kept accountable. We define primary care attachment as a patient’s perception of whether they have a regular primary care clinician or primary care practice where they get care. In Canada, regular primary care clinicians are either family physicians or nurse practitioners; in other countries, they also include physician assistants. We use the term family physicians interchangeably with general practitioners (GPs), as the latter is more common in some other countries. Key data sources include the 2020 Commonwealth Fund survey, 2 the Health System in Transition reports provided by the European Health Observatory7 and the Commonwealth Fund Country Profiles.8
How does Canada compare with peer countries with high primary care attachment?We identified 9 countries with attachment rates of 95% or higher, namely France, Germany, New Zealand, United Kingdom, Denmark, Netherlands, Finland, Italy and Norway (Figure 1). Other OECD countries may also have high primary care attachment (e.g., Israel), but comparable data were unavailable. We compared Canada with these 9 countries on a range of country, health and health system characteristics (Table 1).
 Figure 1:
Figure 1: Percentage of the population who have a regular health care clinician or place to seek care, by country. Data from the 2020 Commonwealth Survey in response to question, “Is there 1 doctor or place you usually go to for your medical care?”2 *For Finland and Italy, data are from Health Systems in Transition reports.9,10 These countries have 100% attachment, but it cannot be determined what proportion of the population has a regular health care clinician versus a place to seek care.
Table 1:Characteristics of Organisation for Economic Co-operation and Development countries with high attachment rates
In all 9 comparator countries, the vast majority of the population reported having a regular primary care clinician; however, in New Zealand and the UK, 10.8% and 13.9%, respectively, reported having a regular place of care.2 Research has shown that longitudinal, relationship-based primary care with a single clinician is associated with better outcomes,21 but it is unclear whether a regular place of care has similar benefits.
According to the 2020 Commonwealth survey, Canada had an attachment rate of 90.5%, with 82.9% reporting a regular primary care clinician. In Canada, patients are generally attached to a specific clinician, so those 7.6% who reported having a regular place of care may have been referring to a walk-in clinic.2
Canada’s population size, degree of rurality and degree of income inequality were in the middle range relative to comparator countries, as were the age and sex distribution and chronic disease morbidity. Compared with other countries, Canada had relatively high maternal and infant mortality rates in 2020. Canada’s total health spending was in the middle of the range across countries; however, Canada had the lowest proportion of total spending that was public at 70%, a statistic that has been consistent since the 1990s.22 Canada, the UK and Denmark had the lowest number of hospital beds per capita.
Although the number of GPs per capita in Canada was near the average, Canada had the lowest total number of physicians per capita (Figure 2). Figure 3A and Figure 3B examine the crude association between the proportion of the population that was attached with the number of GPs and the total number of physicians per capita. The proportion of GPs does not seem to be associated with the rate of primary care attachment (r = −0.098); however, countries with a higher number of physicians per capita appear to also have higher rates of primary care attachment (r = 0.78). The physicians who are classified as GPs may differ by country, influencing comparisons.23
 Figure 2:
Figure 2: The total number of physicians and the number of general practitioners (GPs) per 10 000 people by country. Data on physician totals from the World Health Organization (WHO).19 The number of GPs per 10 000 people was calculated by dividing the total number of GPs retrieved from the WHO20 by the country’s total population, retrieved from the Organisation for Economic Co-operation and Development.11
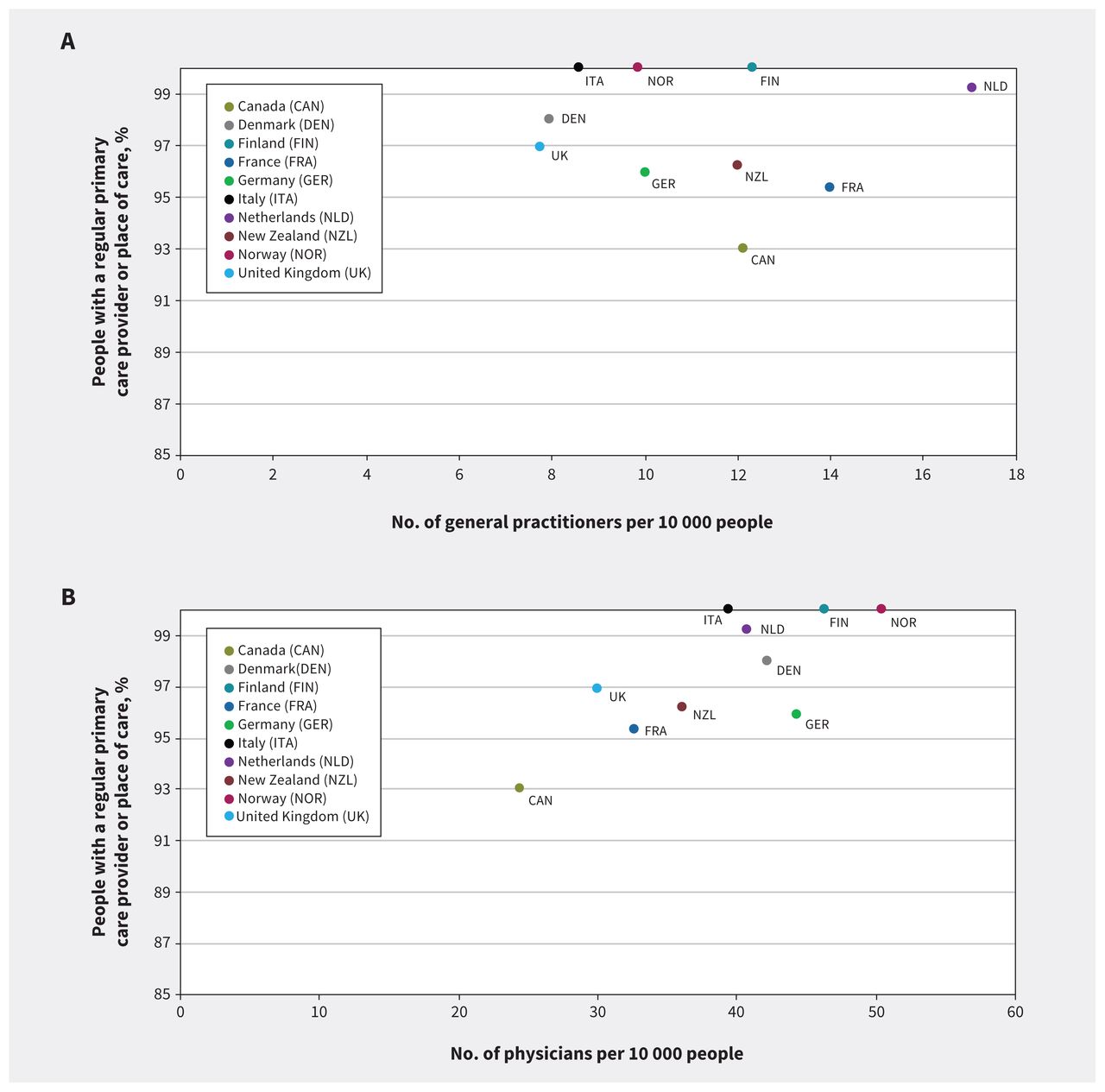 Figure 3:
Figure 3: (A) Rates of primary care enrolment relative to the number of general practitioners (GPs) per 10 000 people by country (r = −0.098, r2 = 0.0096, p = 0.79). (B) Rates of primary care enrolment rates relative to the total number of physicians per 10 000 people by country (r = 0.78, r2 = 0.60, p < 0.05). Data on enrolment from 2020 Commonwealth Survey in response to question, “Is there 1 doctor or place you usually go to for your medical care?”2 The number of general practitioners per 10 000 people was calculated by dividing the total number of GPs (retrieved from the World Health Organization)20 by the country’s total population (retrieved from the Organisation for Economic Co-operation and Development).11
An analysis done by the World Health Organization found that Canada spent less of the total health budget on primary care services than the average among 21 OECD countries (5.3% v. 8.1%, not including dental care expenditures);24 data for Canada and 4 of the comparator countries with available information are presented in Figure 4.
 Figure 4:
Figure 4: Primary care spending as a share of total health care spending. Primary care spending is measured as general outpatient curative care (e.g., routine visits to a general practitioner [GP] or nurse for acute or chronic treatment), home-based curative care (e.g., mainly home visits by GPs or nurses) and preventive care services (e.g., immunization or health check-ups). Data only from countries for which data were available from the Organisation for Economic Co-operation and Development’s policy brief on spending on primary care.24
What system strategies enable high primary care attachment in comparator countries?To analyze health system strategies that enable high primary care attachment, we supplemented key comparative literature2,7,8 with author expertise on primary care in 4 of the comparator countries representing varied geographies, systems and cultures — namely the UK (M.A.), the Netherlands (E.B., V.L.L.C.B.), Norway (I.S.S.) and Finland (J.A.) — and consulted relevant country-specific resources.
In all 4 comparator countries, most primary care is paid for through the publicly funded system, although some have parallel employer or private-pay systems. The national government sets health care priorities, with local authorities tailoring priorities to their context and organizing provision of services. In all 4 countries, GPs play a strong gate-keeping role, mediating access to specialty care. Most GPs practise longitudinal, comprehensive office-based care and are mostly paid by capitation or salary. Use of interprofessional teams varies, although increasing responsibility is being shifted to nurses and other health professionals.9,25–27 Publicly covered walk-in clinics are almost nonexistent and, in all 4 comparator countries, GPs provide after-hours care, which may be mandated (e.g., Norway) or commissioned (e.g., in the UK, GP practices can outsource after-hours care to GP cooperatives or private companies who pay their GPs a sessional rate).9,28–30 Importantly, registration with a GP is either automatic, mandatory or strongly supported, with the system encouraging people to connect with a GP near their place of residence. All countries are experiencing human resource challenges in primary care related to increasing physician workloads, more GPs working part-time, clinician burnout and challenges with recruitment and retention of GPs.31–34
FinlandIn Finland, residents are automatically registered with the health centre that is closest to where they live. Residents have the ability to change their health centre once per year. General practitioners are salaried and receive paid vacation and a pension. In addition to seeing outpatients, GPs at the health centre also provide care in inpatient wards, long-term care, maternity and pediatric primary care clinics and schools. An after-hours clinic is integrated with the hospital emergency department, except in a few rural areas.9 Historically, GPs had their own roster of patients;35 however, the model changed in the 2000s such that patients are provided with the first available appointment to see a physician, which has resulted in a drop in relational continuity.36 Over the past 20 years, health centres have focused on developing better access and interprofessional collaboration in teams that include GPs, physiotherapists, psychologists and nurses with a range of specializations from mental health to chronic conditions.37 Nurses are the first point of contact when a patient calls the health centre. They make the first assessment and provide the patient with further instructions, whether that be at-home instructions or scheduling an appointment to see a health professional at the health centre. In addition to the health centres, occupational clinics are available to serve working residents. All residents can access an integrated health record through a central website.
NetherlandsResidents in the Netherlands must purchase health insurance from private insurers. A strict gatekeeper system exists whereby patients can only be reimbursed for hospital and specialist care if they provide insurers with a GP referral. No co-payments exists for GP visits but are applied for other parts of the system. Patients are encouraged to pick a GP whose practice is close to their home38 and are supported in this process.29 Some GPs restrict acceptance to patients who live in their vicinity.25 If practices refuse patients because rosters are full, health insurance companies are then responsible for finding patients a clinician. General practitioners are paid using 3 different methods, including capitation-based payments that incentivize large roster sizes, payments for contribution to interprofessional care pathways (i.e., type 2 diabetes management) and through performance incentives, for example, for chronic disease management and patient experience.39 A highly organized network for after-hours GP care provides access to primary care 24 hours a day, reducing both the workload for individual GPs and the burden on hospital emergency departments. 40 Information technology supports practice. For example, 58% of Dutch practices allow patients to book appointments online and 22% allow them to view their own health record.33 Most practices have 1 or more GPs supported by clerical staff and, sometimes, trained medical assistants who support, for example, chronic conditions management.41 Current challenges include a relatively low average time spent per patient and a high demand for care that GPs consider “unnecessary.”33
NorwayThe National Regular Practitioner scheme ensures that all residents are automatically assigned to a GP; residents are free to choose a different GP up to twice a year as long as the GP of choice has capacity. Patients who choose not to register are required to notify local authorities.42 General practitioners, who are individually contracted by the municipalities, are typically self-employed and work in groups, usually with 2–6 physicians who share auxiliary personnel such as health secretaries and, occasionally, nurses.28 They are funded through 3 sources, including capitation-based payments from municipalities, out-of-pocket payments from patients (co-payments) and fee-for service payments from the national insurance system.26 Walk-in clinics are not publicly funded and require private payment.28 After-hours care is highly organized, with a national medical helpline for ambulance services and another for out-of-hours medical services. As in the Netherlands, patients will typically connect with a nurse by phone who will assess whether the patient needs an ambulance or should be visited by the GP either at home or at the after-hours clinic.26,28 General practitioners are also required to have timeslots available during the day for patients coming in with urgent concerns. They are gate-keepers for hospital admission; patients seeking care in the emergency department must be either referred by a physician or brought in by an ambulance.35 Providing accessible primary care in rural areas is an ongoing challenge.
United KingdomResidents are encouraged to register with a local practice of their choice on websites designed to highlight nearby health centres according to their postal code.27,43–46 A strong culture of registering with a GP practice exists. For instance, newborns must be registered with a local practice within 6 weeks of birth, otherwise patients are contacted by health visitors to establish the factors behind lack of registration and to suggest suitable GP practices.27 Practices typically do not reject patients unless patients reside out of the practice boundary or they have no capacity.27 When patients move areas, they are encouraged to register with a local practice but are not automatically deregistered from their previous practice. National policy dictates that all patients must have a named GP,47 although patients frequently see different GPs or health care professionals in a practice, even during the same illness. Continuity of care has reduced over the last 2 decades,48 given trends such as more GPs working part-time, incentives to ensure patients receive same-day appointments, increasing size of GP practices49,50 and broader roles for allied health care professionals including pharmacists, physiotherapists, advanced nurse practitioners, social prescribers and health and well-being coaches.51 General practitioners primarily work in longitudinal office practices but opportunities also exist for GPs to work with specialists to run additional outpatient clinics.52 Information on a practice’s quality of care is posted publicly, including patient experience measures related to timely access.53 Although attachment rates are high, the UK is currently experiencing GP shortages and implementing measures such as expanding the number of GP training places, greater use of teleconsultation or online triage systems, task-shifting with allied health care professionals and streamlining processes for foreign-trained graduates to practise in the UK50,54–56 to attempt to address the issue.
What lessons can Canada draw from comparator countries to increase primary care attachment?Canada’s vast geography and diverse population is a contextual factor that must be considered. Proximity to the United States also influences expectations of both clinicians and patients, and related cultural norms.57 Canada’s systems may already be aligned to countries with high rates of primary care attachment, for example, with respect to regional funding of physician services by governments, overall health spending and the use of primary care as a gatekeeper to other parts of the health system. However, historical factors have also influenced Canada’s current system, particularly physicians’ negotiation at the advent of Medicare to remain autonomous, private clinicians who bill the system fee-for-service.22 Canadian health systems can still draw important lessons from countries with higher rates of primary care attachment (Box 1). We propose related actions that can be taken by governments, professional associations and clinicians; special consideration needs to be given to enhancing access in rural areas, which is not specifically discussed.
Box 1: Lessons Canada can learn from OECD countries with high rates of primary care attachmentAccountability
Funding
Higher proportion of total health spending that is public
Higher proportion of total health spending on primary care
More physicians per capita
System organization
Information systems
Practice organization and physician payment
Responsibilities of other health care professionals (e.g., nurses, physiotherapists)
GPs paid by salary or capitation (or practices paid by capitation)
Organized after-hours care
Limited walk-in clinics
AccountabilityIn countries with high rates of primary care attachment, GPs have contractual arrangements and accountability to government, insurers or both. In contrast, most family physicians in Canada are private contractors who carry no obligations or accountability for the breadth of services they provide, the location of their practices, their hours of operation, their staffing mix, the patients they accept or their ability to meet local population needs. In turn, they often receive little support from health systems for infrastructure needs such as information technology, system coordination or interprofessional team members.
Notably, countries with high attachment have GPs working almost exclusively in office-based, generalist practice. In contrast, nearly one-third of Canadian family physicians work in a focused practice, including emergency medicine, hospitalist work, sports medicine and psychotherapy.58 Emergency medicine and hospitalist work are important system functions, and staffing these appropriately would require increases in training of physicians overall. Other types of work, such as exclusive practices for sports medicine and psychotherapy, would likely not be authorized by insurers in comparator countries; professional associations and provincial and territorial governments need to consider how to make office-based, longitudinal practice the career path of choice for family medicine graduates. Clinicians and professional organizations should consider whether bringing physicians into the system may have benefits for both physicians and the public, given current challenges.
FundingFederal and provincial and territorial governments could increase the proportion of health spending that is public; for example, Medicare coverage could be extended to include prescription medications, dental care and more mental health care, thereby reducing reliance on physicians to fill related gaps. A higher proportion of the total health budget should be spent on primary care, which would enable needed infrastructure and workforce investments. Canada also needs more physicians per capita. Fewer physicians overall means that family physicians need to step in to support other parts of the health system (e.g., hospital-based care), which leaves less of the workforce oriented toward office-based care. It also means that family physicians are less likely to get timely access to other specialists, which increases practice burden. Wait times to see a specialist in Canada are noted to be especially high, compared with other countries.59
System organizationLocal or provincial and territorial governments could move to a system whereby residents are automatically registered, or have the right to register, with a group practice close to home. These group practices would provide primary care services paid for by the government and would need to be resourced to meet population need. Shifting GP tasks to other health team members such as nurses, physiotherapists and psychologists could theoretically increase workforce capacity, especially if nonphysician team members could be the first point of contact. Other countries could provide models on how to integrate non-health professionals such as trained medical assistants in practice. Guaranteeing access to primary care may result in a trade-off with relational continuity and timely access for nonurgent care — but such trade-offs may be better than the status quo of high levels of nonattachment to primary care in Canada.
Information systemsGovernments could invest in information systems that can improve practice efficiency and thereby increase capacity, for example, by streamlining patient communication with tools such as online booking and secure communication. Moreover, Canadian jurisdictions need to implement a single health record that can be accessed by patients and clinicians in different parts of the health system.
Practice organization and physician paymentProvincial and territorial governments and professional associations could work to increase uptake of salary or capitation payment for GPs, as such payment mechanisms can help to ensure greater population coverage. Capitation provides a set payment per patient that is usually adjusted for patient age, sex and medical or social complexity, and inherently incentivizes larger patient panels. Currently, most family physicians in Canada are paid through fee-for-service.60 National professional organizations have been advocating strongly for payment reform that includes blended capitation payments that account for patient complexity.61
Comparator countries have far fewer walk-in clinics and instead have standards or accountability for timely access, including public reporting of patient experience measures. After-hours care is organized and supported regionally, which simultaneously ensures populations have access to urgent care while reducing the practice burden on GPs (i.e., GPs work fewer after-hours shifts because shifts are shared regionally among a larger pool of physicians and after-hours care is supported by a team). Having fewer walk-in clinics allows more of the primary care workforce to deliver generalist, continuity-based, office-based care. The COVID-19 pandemic led to a rise in urgent care models in Canada, many of which are profit-driven; instead, governments and professional associations should consider regulating and limiting resources spent on episodic — as opposed to longitudinal — care.
ConclusionPrimary care is the front door of the health care system, yet almost 1 in 5 people living in Canada did not have a primary care clinician at the outset of the pandemic, and the situation is poised to get worse if left unaddressed. Canada can learn from OECD countries such as the Netherlands, Norway, the UK and Finland, where more than 95% of people have a primary care clinician, near-universal insurance coverage exists, the proportion of health spending that is public and spent on primary care is larger than Canada’s and GPs are organized better in teams and are more accountable for the care they must provide. These international examples can inform bold policy reform in Canada to advance a vision of primary care for all.
FootnotesCompeting interests: Erica Barbazza reports funding from Horizon 2020 Marie Skłodowska-Curie Actions and consulting fees from the World Health Organization. Tara Kiran reports funding from Health Canada, and honoraria from the Ontario Medical Association, Ontario College of Family Physicians, Ontario Ministry of Health, Canadian Medical Association and Canadian College of Family Physicians. No other competing interests were declared.
This article has been peer reviewed.
Contributors: Richard Glazier and Tara Kiran conceived of the study. Heba Shahaed, Richard Glazier and Tara Kiran designed the study, gathered the data and conducted the analysis. All of the authors helped interpret the data. Heba Shahaed and Tara Kiran drafted the manuscript. All of the authors revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: Tara Kiran and Richard Glazier are supported as clinician scientists by the Department of Family and Community Medicine at the University of Toronto and at St. Michael’s Hospital. Tara Kiran is the Fidani Chair of Improvement and Innovation in Family Medicine at the University of Toronto. This analysis was supported by funding from the Fidani Chair and the Canadian Institutes of Health Research (no. SOP 162662).
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
Comments (0)