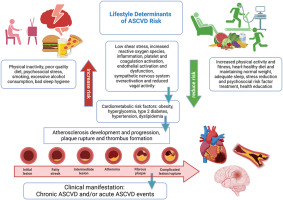
Cardiovascular disease (CVD) accounts for almost 33% of all deaths and 388 million disability-adjusted life years globally [[1], [2], [3]]. The primary driver of CVD mortality is atherosclerosis i.e. narrowing of the arteries resulting in a limited blood flow through them. Atherosclerosis can ultimately lead to myocardial infarction (MI) and stroke, which together account for 85% of all cardiovascular deaths [1,2]. Cardiovascular disease is an overall term for different CVDs with heterogeneous aetiologies. CVDs that have atherosclerosis as the underlying pathophysiology are jointly termed atherosclerotic CVD (ASCVD) and include ischemic heart disease (IHD) such as MI, cerebrovascular disease (e.g. stroke) and peripheral artery disease (PAD) [4]. The pathogenesis of ASCVD is multifactorial and modifiable risk factors include hypertension [5], dyslipidaemia [[6], [7], [8]] and obesity [9,10] which are linked to lifestyle risk factors including smoking [11], high alcohol consumption [12] and physical inactivity [13].
Ample epidemiological evidence shows that CVD aggregates in families. In a meta-analysis of 26 observational studies, a positive parental history of CVD was associated with an approximately doubling in the risk of developing CVD in the offspring [14]. The familial aggregation of CVD is likely a consequence of both genetic and environmental factors as well as their interaction [15]. Offspring with parental CVD may have subclinical disease and adverse risk factor profiles long time before the potential onset of CVD. Identifying individuals with adverse risk factor profiles has important implications for primary prevention. This is especially relevant in individuals at high risk such as individuals with parental CVD.
Studies investigating offspring CVD risk factors in relation to parental history of CVD generally found that offspring with a positive parental history of CVD have more unfavourable risk factor levels [[16], [17], [18], [19], [20]] or a higher prevalence of hypercholesterolemia and hypertension [21] compared to offspring with no parental history of CVD. However, various approaches for defining parental history and the type of CVD have been used and thorough investigation of the risk factors often were not the main priority. Moreover, parental history of CVD often rely on offspring self-report [16,17,19,22] and validation of the parental events is often limited or not done, although offspring self-report may cause recall bias [23,24]. Parental age at onset is important to consider because the risk of CVD is found to differ by parental age at onset [14,[25], [26], [27]] with an early onset composing a higher risk of familial aggregation and believed to reflect stronger inherited influences. Yet, parental age at onset is often not considered when studying risk factor levels [[17], [18], [19],21,22]. Adjustment for potential confounders such as socioeconomic status and lifestyle factors is also limited or not done [[16], [17], [18], [19],21,22]. To our knowledge, no study has taken all these components into consideration although they may be important for improved risk assessment and risk stratification. Therefore, the aim of this study was to investigate if offspring of parents with ASCVD, ascertained through registry linkage, have more adverse risk factor profiles in terms of a higher blood pressure, higher body composition measures (body mass index (BMI), waist circumference, visceral adipose tissue, percentage of body fat), higher levels of several blood lipid fractions (triglycerides, total cholesterol, LDL (low-density lipoprotein) cholesterol, non-HDL (high-density lipoprotein) cholesterol) and lower levels of HDL cholesterol compared to offspring without a parental history of ASCVD at different parental ages at onset.




留言 (0)