
記住我




The aim of the present retrospective study was to investigate the influence of cantilever prosthetic arm on the marginal bone loss (MBL) around dental implants supporting short partial fixed prostheses.
HypothesisThe null hypothesis of the present study was that there will be no significant difference in MBL between 3-unit implant-supported partial fixed prostheses with and without cantilever prosthetic arm, against the alternative hypothesis of a difference.
MaterialsThis retrospective study included patients treated with dental implants during the period 1980–2018 at one specialist clinic (Clinic for Prosthodontics, Centre of Dental Specialist Care, Malmö, Sweden). This study was based on data collection from patients’ dental records. The implants were placed by specialist dentists in oral surgery, and dentists performing the prosthetic treatment were specialists in prosthodontics.
The study was approved by the regional Ethical Committee, Lund, Sweden (Dnr 2014/598; Dnr 2015/72). The present retrospective study followed the STROBE guidelines for observational studies [14] and was registered at https://clinicaltrials.gov under the registration number NCT02369562. The investigation was conducted according to the principles embodied in the Helsinki Declaration of 1964 for biomedical research involving human subjects, as amended in 2013 [15].
DefinitionsA cantilever prosthetic arm was defined as a pontic which is retained and supported only on one side by the other prosthetic units which are supported by implants.
MBL was defined as loss, in an apical direction, of alveolar bone marginally adjacent to the dental implant, in relation to the marginal bone level initially detected after the implant was surgically placed [16].
For this study, patients smoking a minimum of one cigarette per day (an everyday smoker [17]) were classified as smokers, established at the clinical appointment of the patient when the anamnesis was performed.
The diagnosis of bruxism was established in a previous study [18], in which the patients of the aforementioned database (which the present cohort group of patients was selected from, according to the inclusion/exclusion criteria) suspected to be bruxers were called back for one clinical appointment to get the minimum information to diagnose the patients as ‘probable bruxers’ (self-report/anamnesis + clinical examination).
As the standard protocol in the clinic, the patients’ dental hygiene was followed up by a dental hygienist within 6 months after the final implant-supported/retained restoration. Each patient then attended a dental hygiene recall program based on individual needs.
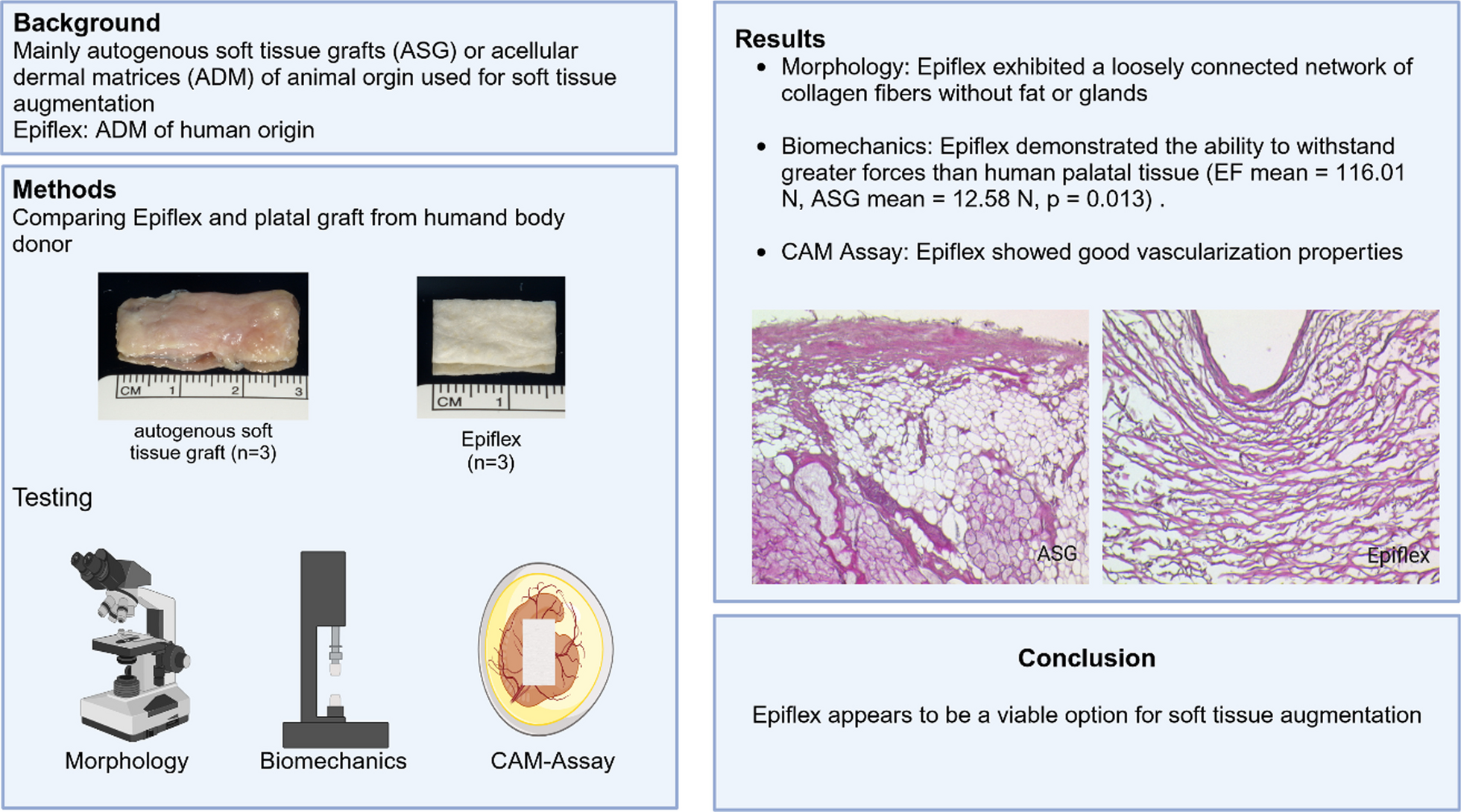
Inclusion and exclusion criteriaOnly implant-supported FPDs with three prosthetic units, either supported by two or three implants, were considered for inclusion. FPDs supported by two implants could had either a prosthetic pontic replacing a tooth between the implants, or a prosthetic arm cantilever (Fig. 1). Only implants not lost and with baseline radiographs taken within 12 months after implant placement and with a minimum of 36 months of radiological follow-up were considered for the analysis of MBL. Negative values of MBL corresponded to bone loss.
Fig. 1
Examples of radiographs of cases included in the present study: 3-unit prosthesis supported by two implants with a cantilever (left column), 3-unit prosthesis supported by two implants with a pontic (middle column), and 3-unit prosthesis supported by three implants (right column)
Patients with all modern types of threaded implants with cylindrical or conical design were included. Zygomatic implants were not included in the study, as well as implants detected in radiographies, but without basic information registered in the patients’ records.
Patients were excluded if they had history of periodontitis and/or were treated for periodontal disease. It is important to take note that as standard, all patients receiving implants at the Specialist Clinic for Prosthodontics were periodontally healthy at the time of implant installation. Patients with either a history or with signs of periodontal disease were treated at the Specialist Clinic for Periodontology, where they later could or not receive dental implants, according to individual needs/indications. These patients were not included in the present study.
Data collectionThe data were directly entered into a SPSS file (SPSS software, version 28, SPSS Inc., Chicago, IL, USA) as the dental records of the patients were being read, and it consisted of several implant-, site-, and patient-related factors. The following data were collected from the patients’ dental records:
Implant-related factors: implant diameter (three groups: < 3.75, 3.75, and > 3.75 mm), system, and implant surface (turned/machined, modified);
Site-related factors: implant region, implant jaw location (maxilla/mandible), anterior or posterior location of the implant (sites from right canine to left canine teeth were considered anterior location), bone quantity and quality of the implant site at the day of the implant installation, according to a classification [19];
Surgery-related factors: open or flapless surgery, immediate installation in extraction socket or in healed site;
Prosthetic-related factors: prosthesis fixation (screwed, cemented);
Patient-related factors: patient’s sex, age of the patient at the implant insertion surgery, diabetes, and behavioral history (bruxism, smoking);
Time-related factors: implant and prosthesis installation date, clinical and radiological follow-up time.
Evaluation of radiographsReproducible intra-oral periapical radiographs were used. When there were no available digital radiographs from the baseline appointment, the analogue periapical radiographs were scanned at 1200 dpi (Epson Perfection V800 Photo Color Scanner; Nagano, Japan).
MBL was measured after calibration based on the inter-thread distance of the implants. Measurements were taken from the implant-abutment junction to the marginal bone level, at both mesial and distal sides of each implant, and then the mean value of these two measurements was considered (Fig. 2). MBL was calculated by comparing bone-to-implant contact levels to the radiographic baseline examination. The Image J software (National Institute of Health, Bethesda, USA) was used for all measurements.
Fig. 2
Measurement of the distance from the implant-abutment junction (black line indicated by the white arrow) to the first visible bone-to-implant contact, on both mesial (a) and distal (b) sides on periapical radiographs. Calibration was based on the inter-thread distance of the implants (c)
The sets of radiographs for every patient were codified and the authors who performed the radiological measurements (S.A.K, J.A.K.) were blinded to the patients’ identification.
CalibrationAn initial calibration concerning MBL was performed between the authors. The process was done for 10 random samples from the cohort group, and verified after the measurement of each sample. At the end of the process the measurements from the different individuals were considered enough approximate from each other, with agreement between examiners set at > 90% of the distance in millimeters.
Sample size calculationA calculation of the sample size was not conducted. The reason is that the database from which the eligible cases for the present study were originated had a certain number of patients and dental implants, namely, approximately 2800 and 11,000, respectively, and it would not possible to recruit more cases, as the database already included all patients treated with dental implants during the aforementioned period in the specialist clinic.
Instead, all the 3-unit implant-supported FPDs were initially considered eligible for inclusion, to get the maximum number of cases available, namely, the largest sample size possible from this database, provided that these cases would fulfill the inclusion criteria, i.e., baseline radiographs taken within 12 months after implant placement and with a minimum of 36 months of radiological follow-up.
Statistical analysesThe mean, standard deviation, and percentages were presented as descriptive statistics. Kolmogorov–Smirnov test was performed to evaluate the normal distribution of the variables, and Levene’s test evaluated homoscedasticity. The performed tests for two independent groups were Student’s t test or Mann–Whitney test, one way ANOVA or Kruskal–Wallis test for three independent groups, and paired-samples t test or Wilcoxon signed-rank test for two dependent groups, depending on the normality. Pearson’s Chi-squared test or Fisher’s exact test was used in the analysis of contingency tables of categorical data of independent groups. Correlation and linear regression were performed to check the relationships between MBL and time of follow-up.
Univariate linear regression models were used to compare MBL over time between clinical covariates. The estimation of MBL over time (dependent variable) was expressed in a single linear regression equation, for each of the categories of each independent variable (smoking, diabetes, bruxism, sex, age, jaw, jaw region, tooth region, implant diameter, implant surface, prosthesis type, prosthesis fixation). For the present study, the linear regression equation was expressed as
where ‘y’ is the estimated MBL over time. ‘b’ is the estimated intercept at the y-axle in the scatter plot. ‘a’ is the estimated MBL per every 1 month of follow-up. ‘x’ is the number of months of follow-up.
Thus, if one would like to estimate the MBL of a certain category of a certain variable at, for example, 100 months of follow-up, ‘x’ is replaced by the value of 100 in the equation given for that particular category and variable.
To verify multicollinearity, a correlation matrix of all of the predictor variables was scanned, to see whether there were some high correlations among the predictors. Collinearity statistics obtaining variance inflation factor (VIF) and tolerance statistic were also performed to detect more subtle forms of multicollinearity. A linear mixed-effects model was built with all variables that were moderately associated (p < 0.10) with MBL in the univariate linear regression models. Mixed-effects model was used to take into consideration that some patients had more than one implant-supported prostheses, as multiple observations within an individual are not independent of each other. Multiple testing corrections for p values were performed by the Bonferroni adjustment.
The degree of statistical significance was considered p < 0.05. Data were statistically analyzed using the Statistical Package for the Social Sciences (SPSS) version 28 software (SPSS Inc., Chicago, IL, USA).
留言 (0)