It is well-known that the mylohyoid originates from the mylohyoid line, and this is what is stated in all textbooks. Although Gray’s Anatomy describes the anterior mandibular attachment below the mental spines as located at the “symphysis menti,” [16], and Zdilla et al.’s paper also describes this site as the “mandibular symphysis” [17], these are very minor mentions in comparison with the mylohyoid line. In the present study, the mandibular symphysis was the origin of the anterior mylohyoid muscle fascicles in all specimens. The mandibular symphysis also played the role of the anterior attachment point of the mylohyoid raphe, and it was connected to the posterior hyoid by the mylohyoid raphe. This showed that the mandibular symphysis thus plays an important role as the location of the anterior mylohyoid attachment to the mandible. However, the anterior muscle fascicles of the mylohyoid were generally very thin, and their attachment tended to be weak.
The present results showed that, in about half of mylohyoids, the mylohyoid line was not continuous with the mandibular symphysis, and that, in the anterior part, there was bilateral communication between the sublingual and submandibular spaces. Whereas sublingual gland herniation was apparent in 23.0% of all cases, superior–inferior penetration caused by loose muscle fascicles was present in 57.3%. The mean thickness of the central muscle fascicles adjacent to the mylohyoid raphe was less than 1.0 mm, whereas in the vicinity of the mylohyoid line, it was approximately 1.7 mm, and there was a tendency for it to be thinner closer to the midline, but there was no evidence at all of a split in the mylohyoid raphe itself. Penetration was most commonly seen in the central muscle fascicles, being present in 36.4% when both sides were included. From the above results, it should be considered that there are numerous routes of superior–inferior communication between the sublingual and submandibular spaces. The present study suggested that the mylohyoid functions only weakly as a septum on the lingual side of the premolar region, and that it may be a vertical route of communication, particularly for bleeding or infection in the sublingual area.
In contrast, the posterior muscle fascicles formed a thick sheet in the vicinity of both the origin and the terminus, with no evidence at all of superior–inferior penetration. The posterior fascicles preserve their thickness up to the posterior margin of the mylohyoid, and further posterior to this posterior margin there was complete communication between the sublingual and submandibular spaces via loose connective tissue. In some cases, the mylohyoid raphe was clearly visible as tendinous tissue, whereas in others, it was apparent as the union of the left and right mylohyoids, but in all specimens, the mylohyoid raphe was always continuous from the mandibular symphysis to the hyoid. The fasciae covering the mylohyoid were generally thin, and at sites where the muscle fascicles were disrupted the submandibular and sublingual spaces were separated only by loose connective tissue. The mylohyoid muscle fascicles can be broadly divided into those that terminate at the hyoid and those that terminate at the mylohyoid raphe, and this structure means that a gap can readily appear at the boundary between these two types of muscle fascicles. In addition, the sublingual glands are often herniated within this gap. This means that sublingual gland herniation and perforation are frequent in the central part of the muscle even at sites, where the muscle fascicles are thick. The mylohyoid is also known as the “oral diaphragm,” and it is generally considered to provide a complete division between the sublingual and submandibular areas above and below. However, what supports its role as a septum is its attachments to the mandible and the hyoid. The above results suggest that, despite the fact that the mylohyoid functions only weakly as a septum, and that routes of communication may be present between the sublingual and submandibular spaces in both its anterior and central parts.
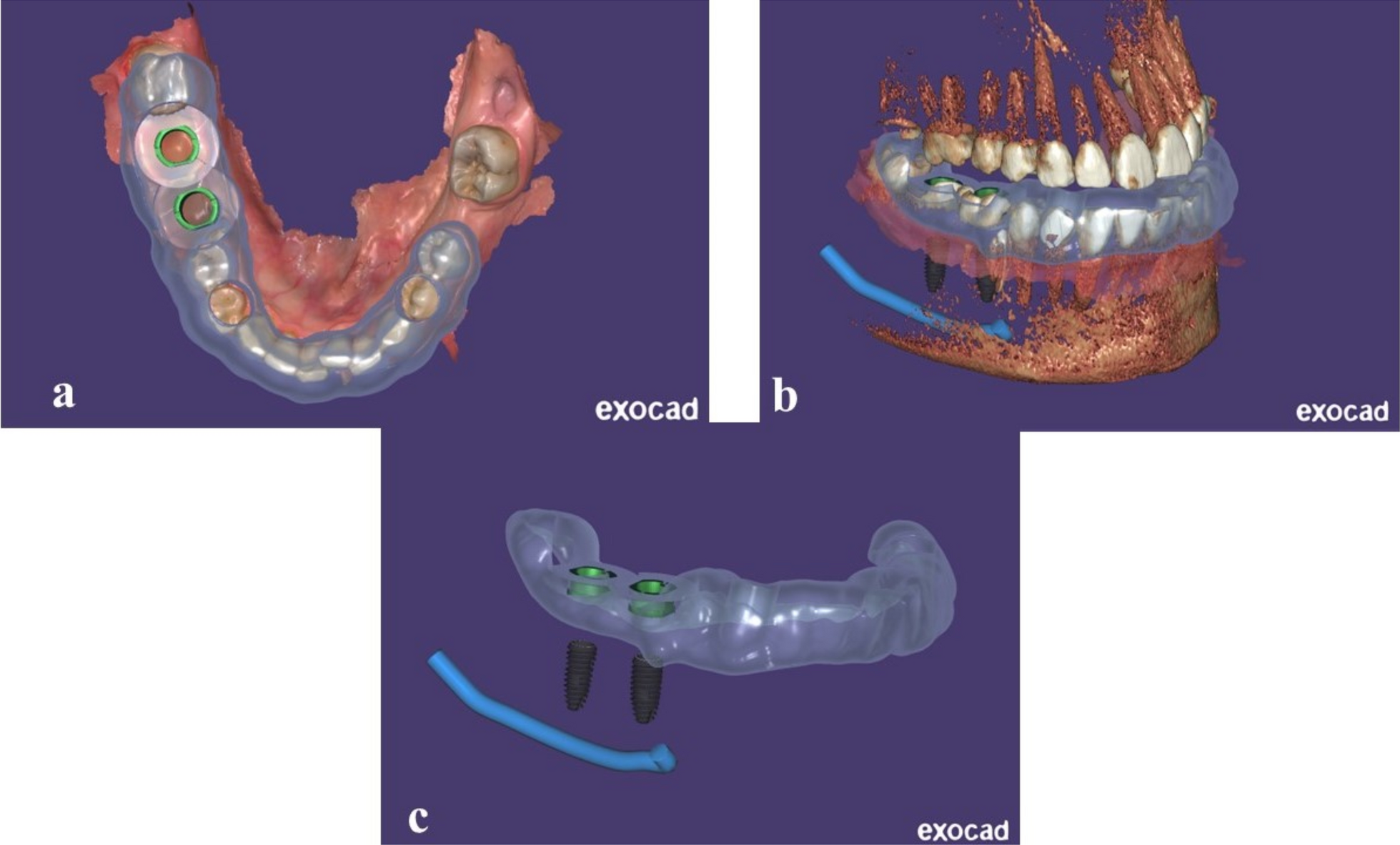
The most frequent complications of implant surgery are infection, implant rejection, implant migration and implant fracture [18,19,20]. As is known, dental implant migration into the maxillary sinus is a complication sometimes encountered in implant treatment [21, 22]. In addition, Cariati et al. reported a very rare case of displacement of a normally placed implant body into the sublingual space [22]. The authors suggested that the implant displacement was caused by the resorption of the internal jaw cortical. The reason for this is that during the first surgery the implant was severely medially inserted. Consequently, the lack of primary implant stability is the major cause of this complication. If the implant strays into the sublingual space, antibiotics must be administered to prevent Ludwig’s angina and the implant must be removed promptly in the operating room. Furthermore, Choi et al. reported that post-oral surgery sublingual hematoma leading to life-threatening airway obstruction requires immediate recognition and prompt management [23]. Most dental implant specialists are alert to the possibility of perforation of the lingual-side cortical bone by the implant as an accidental complication during oral implant insertion in the area from the mandibular incisal region to the premolar region [9, 24,25,26,27]. In a cadaver study, Fujita et al. also suggested that because the sublingual and submental arteries run through the sublingual space, if an implant perforates the lingual-side cortical bone, it may blindly damage these arteries and cause arterial bleeding, which may result in airway obstruction or other fatal complications [8]. Therefore, we reaffirmed the importance of carefully confirming the placement direction using a surgical guide when performing implant placement in the mandibular anterior region.






Comments (0)