
Remember me







The primary objective of this trial is to compare the effect of adherence support interventions on clinical and biological endpoints using an adaptive randomized platform. We hypothesized that in a randomized, adaptive implementation trial, the psychosocial + mHealth support arm will be associated with improvement in a composite MDR-TB and HIV clinical outcome compared to mHealth, psychosocial support, or enhanced standard of care arms.
The primary outcome will be a comparison of the percentage of participants achieving a composite of undetectable HIV viral load, MTB culture conversion, survival, and retention in care at 12 months in each arm. Secondary outcomes will include all components of the primary outcome as well as a quantitative evaluation of adherence on TB and HIV treatment response (Table 1).
Trial designThis study will follow a four-arm adaptive trial design to evaluate four adherence support strategies on a combined endpoint in adults with confirmed MDR-TB and HIV initiating bedaquiline-containing MDR-TB treatment regimens and on ART in KwaZulu-Natal, South Africa (Fig. 1). Interventions arms include Arm 1 enhanced standard of care, Arm 2 psychosocial support, Arm 3 mHealth using cellular-enabled electronic dose monitoring, and Arm 4 combined mHealth and psychosocial support (Table 2). The level of support will be titrated using a differentiated service delivery (DSD)-informed assessment of treatment support needs.
Fig. 1 Table 2 Differentiated service delivery (DSD) elements in the four intervention armsTrial population and setting
Table 2 Differentiated service delivery (DSD) elements in the four intervention armsTrial population and settingEligible participants will be consecutively recruited adult patients (age ≥ 18 years) meeting all of the following inclusion criteria: (1) culture or molecular test positive for TB; (2) molecular test positive for HIV or with a known or documented history of HIV; (3) drug-susceptibility testing by molecular (i.e., GeneXpert MTB/RIF) or conventional testing demonstrating at least rifampicin-resistant TB; (4) initiating treatment with a bedaquiline-containing TB regimen within 4 weeks of enrollment; (5) on treatment with ART regimen, including dolutegravir-containing combination ART regimen, or starting ART within 4 weeks of enrollment; (6) capacity for informed consent in either isiZulu or English. Patients will be excluded from the study if they do not meet eligibility criteria, are prisoners, are pregnant at time of enrollment, or are considered by study team to be too ill to participate in the trial.
Participants will be recruited from MDR-TB treatment facilities and affiliated outpatient TB clinics in Durban, South Africa. Study visits will be conducted within the established research infrastructure at the Durban CAPRISA Springfield Clinical Research Site.
Adaptive randomizationEligible participants will be assigned to one of four intervention arms at baseline using a two-step randomization. Participants will be initially randomized to Arm 1 vs Arms 2–4 in a 1:3 ratio, with randomization stratified by baseline variables (undetectable vs detectable HIV viral load, 6-month vs. extended MDR-TB regimen, inpatient vs outpatient, history of previous bedaquiline exposure). Bayesian adaptation will be accomplished by utilizing a run-in period where the first 40 participants will be randomized without any adaptation. After the first 40 participants have been randomized and achieve preliminary outcomes at 4 months, results will be incorporated in a Bayesian fashion to modify the randomization procedure for subsequent participants weighting randomization toward favorable study arms. A web-based application (R shiny 1.7.4) will be used to perform adaptive randomization in real-time.
Trial interventionsAfter assignment into one of 4 arms as described above, each participant will receive an Arm specific intervention (Table 2).
Enhanced standard of care (Arm 1) will include usual care as administered by hospital and clinic staff, enhanced by study staff providing treatment literacy and extra training for treating physicians, nurses, pharmacists, and social workers prior to trial initiation and periodically with refresher trainings throughout the trial duration.
The psychosocial support intervention (Arm 2) will include discharge or community treatment planning depending on inpatient vs. outpatient treatment status, monthly individual counseling, community adherence support groups, and home visits. The intensity of the support will be calibrated based on monthly assessment by study counselors. Participants will be administered standardized TB and ART adherence assessment questionnaires monthly. Participants with a low standardized adherence score will be considered at risk for non-adherence, will have the intensity of the intervention increased, may include telephonic check-ins by study staff and increased frequency of counseling sessions from monthly to biweekly, and may have a home visit conducted by a multidisciplinary study team. Monthly adherence support groups will not be calibrated.
Participants randomized into the mHealth intervention (Arm 3) will receive two Wisepill RT3000 cellular-enabled electronic pill boxes (“Wisepill”): one with ART and one with bedaquiline. They will also receive training on pill box loading, charging, and storage. Each Wisepill device will be appropriately marked to avoid confusion and stigma. Pill box openings will serve as a surrogate for adherence to ART and bedaquiline, respectively. Each participant will select a text message reminder from a guided menu of choices. Participants will receive a weekly text message encouraging regular adherence. For bedaquiline, one missed, and for ART, 2 missed EDM openings within a 2-week window (not due to technical issues) will trigger an additional text message reminding the patient to take their medication. For EDM openings recorded outside the EDM dose window or continued missed doses, it will be up to the investigators’ discretion to issue additional text messages or semi-scripted study calls to support adherence. The psychosocial support + mHealth intervention (Arm 4) will include a combination of Arms 2 and 3. Patients will be considered at risk for non-adherence by a low adherence score as described in Arm 2 and/or missed openings recorded by Wisepill devices as described in Arm 3 and increased support will be delivered as described above.
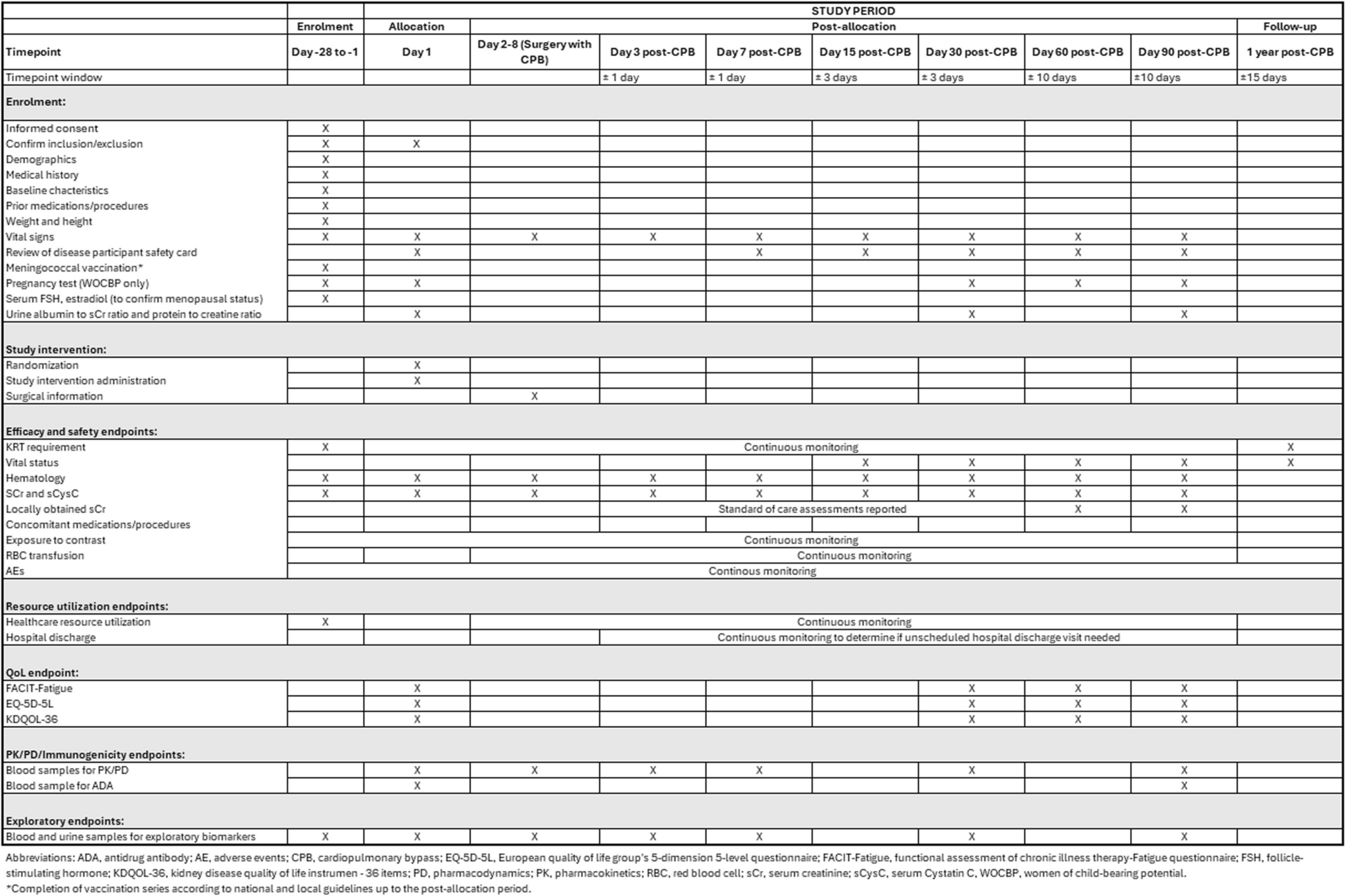
Trial timelineThe trial timeline will include 6 months to train study staff on the protocol, including the randomization strategy and software use. Approximately 4 years will be allowed for enrollment. Participants will be followed monthly through the 6 months of intervention with an additional in-person visit at 12 months to establish the primary outcome, and through the end of treatment (approximately 18 months after treatment initiation) telephonically. Data for the study will be collected at the following visits: (a) baseline (enrollment) visit, (b) monthly clinical visits (months 1–6), (c) follow-up or end of treatment visit, and (d) at community adherence support groups (Fig. 2). Sputum will be collected monthly, and serum for HIV viral load testing will be collected at months 0, 2, 6, and 12.
Fig. 2
Schedule of study evaluations
Informed consentResearch assistants will recruit and enroll participants. Screening of participants is done at hospital and clinic facilities primarily at King Dinuzulu Hospital and KwaMashu community clinic. If a participant meets the protocol eligibility criteria, an informed consent procedure is conducted and the participant is then enrolled. A member of the study staff will explain the protocol and informed consent documents, with opportunity to ask questions, prior to seeking informed consent in the preferred language of the potential participant (English or isiZulu). Enrollment can occur on a different day from screening.
Statistical analysisThe study is powered to enroll a total of 400 participants, who will be randomly assigned to one of four trial arms (Table 2). A Bayesian adaptive randomization algorithm will be used to assign interventions to participants to improve the power of detecting any superior arm(s) and to increase the number of participants treated in the better arm(s) during the study. We varied the estimated success rate, based on prior observational data in the same population, between 70 and 90% with power as low as 74% and as high as 98% depending on differences in success rates (Table 3). Family-wise error rate, the probability of erroneously declaring any non-superior arm(s) superior, will be between 0.005 and 0.020 depending on treatment success in the various arms.
Table 3 Adaptive study design power analysis showing two possible effect estimates and various scenariosData managementPrior to enrollment, all research staff will participate in Human Subjects Protection training/Good Clinical Practice training to ensure sensitive data confidentiality. Informed Consent Forms and all forms containing patient identifiers will be kept separate from study forms in a secure, locked location. Upon enrollment, participants will be assigned a unique study identifier (PID) assigned by the CAPRISA Data Management Center, which will be used on all case record forms (CRFs) to identify the participant for the duration of the study. RedCap software will be utilized for the development of study forms, data entry, and data management of electronic data. Electronic data will be kept securely on encrypted and password-protected end point devices with support from the CAPRISA Data Management Core. Users on the study team will have access to the study database with individual login credentials including username and password. Only designated members of the study staff will have access to the key linking the study PID data to patient identifiers.
Data safety monitoring and reviewAs a single-center study, there is no coordinating center. The trial steering committee is comprised of the co-investigators of the study, abbreviated from the author list: M.O., J.Z., R.P., K.N. Meetings are occurring weekly at CAPRISA along with a steering committee meeting occurring monthly for the duration of the trial. Quality checks will be performed on the data entered into the RedCap database and completed CRFs will be checked by the quality control officers. CAPRISA data managers will verify and validate patient data and ensure Quality Control reports are produced and approved per CAPRISA data management Standard Operating Procedures (SOPs). The CAPRISA laboratory manager will ensure that all involved laboratories are compliant with Good Laboratory Practice. The CAPRISA pharmacist will provide oversight for the preparation of the electronic pillboxes and pill counts. Quality assurance/quality control of data will be undertaken according to established CAPRISA SOPs.
Community involvementEngagement with the provincial department of health and local health personnel has been initiated. Community engagement through the CAPRISA community program and a study community advisory board (CAB) is ongoing.
Ethics and disseminationThe study will be conducted in compliance with South African, US, national, and local regulations and guidelines applicable to research involving human subjects, and in accordance with the International Conference on Harmonization/Good Clinical Practice. This is a minimal risk study in which investigational products or devices are not being used. Adverse events, or serious adverse events, are submitted to the University of KwaZulu-Natal (UKZN) Biomedical Research Ethics Committee (BREC) for review within standard guidelines. The trial protocol has received approval from the IRB at Columbia University and UKZN BREC. The Trial Steering Committee and CAPRISA data managers will meet to review trial conduct quarterly throughout the trial period. Protocol amendments are generated by the study team led by the PI and subsequently submitted for review to BREC (CAPRISA, South Africa) and the Columbia University Human Research Protection Office prior to implementation. The revised protocol will be maintained in the Investigator Site File and updated in the clinical trials registry. Deviations from the Protocol will be fully documented and a record kept at both CAPRISA and Columbia sites of all amendments and renewals that occur. The funder will be notified of protocol updates through protocol reporting. Results of this study will be made available and communicated to participants, healthcare professionals, and the public via publication and trial registry.
Comments (0)