
Remember me

The enrolled patients involved 104 (57.8%) males and 76 (42.2%) females with male to female ratio 1.37:1, with a mean age of 41.35 ± 44.36 months. One hundred (55.67%) patients were living in urban regions, while the remaining 80 (44.4%) were living in the rural regions. The mean weight for the included patients was 1.42 ± 11.29 kg.
Respiratory conditions like pneumonia and adult respiratory distress syndrome (ARDS) were the most frequent cause for admission to the PICU among the studied CIP accounting for (36.7%), followed by neurological conditions like cerebral palsy and Guillain-Barré syndrome (GBS) (22.8%), infections (20.6%), perioperative (17.2%), and shock (16.7%).
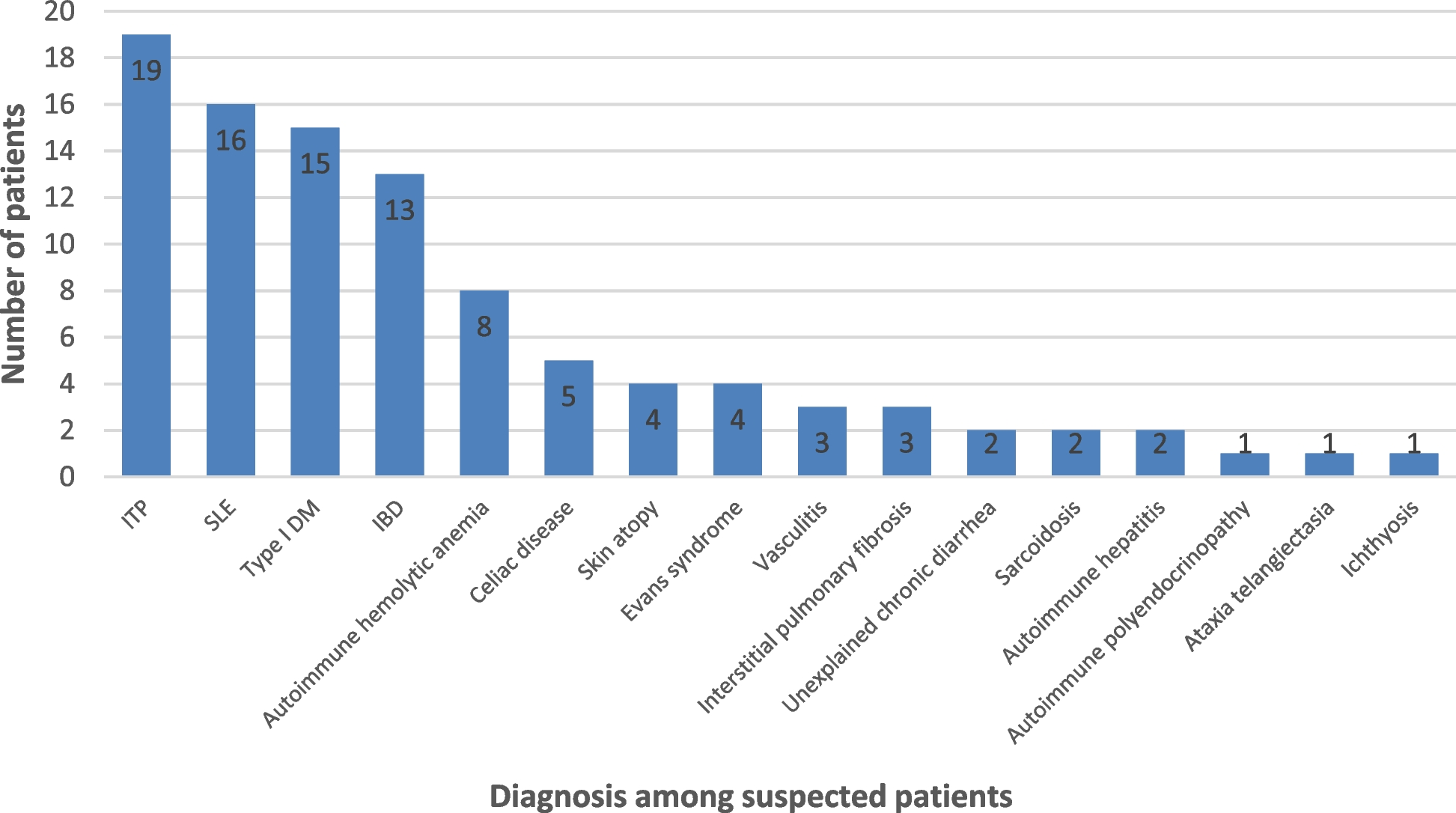
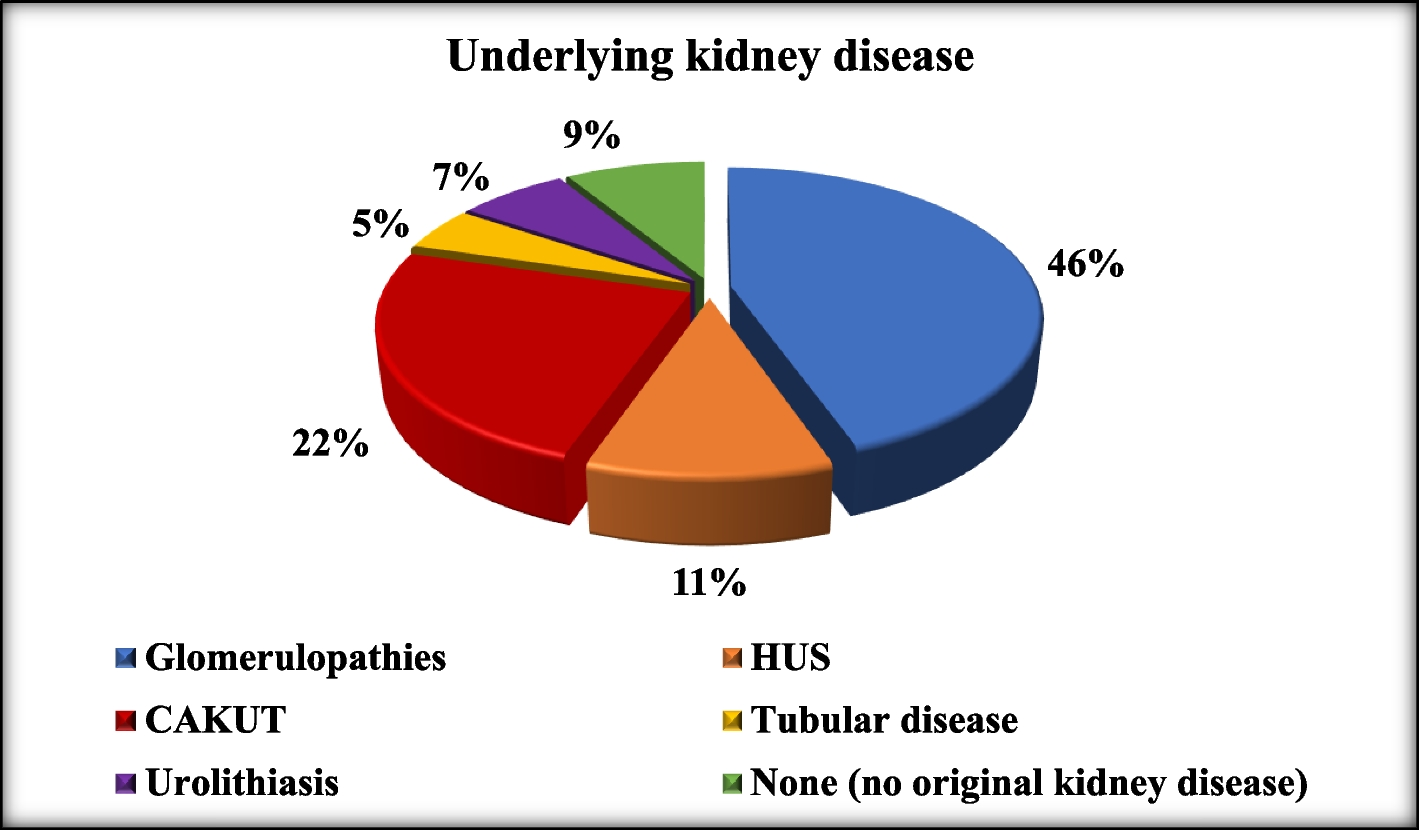
Thirty percent of the studied population received plasma transfusion for moderate illness followed by critical illness (23.3%). Hypoalbuminemia and physician conceptions accounted for 22.8%, and 12.8% of the indications for plasma transfusion in the current study as presented in Fig. 1.
Fig. 1
Indications for plasma transfusion in the study group
According to the indication for plasma transfusion, there was a significant decrease in PTT after plasma transfusion with p-value = 0.025 being more PTT change in critical illness and transfusion according to physician conceptions as presented in Table 2.
Table 2 Change in the bleeding profile after plasma transfusion according to the reason of plasma transfusionIn the studied patients, the mean number of plasma transfusions per patient (2.51 ± 1.75 transfusion), volume of transfused plasma (14.19 ± 2.25 ml/kg), and time interval between admission and time of 1st transfusion (3.24 ± 3.49 days), respectively, are presented in Table 3.
Table 3 Data of plasma transfusion in the study groupFor assessment of severity of illness, the MODS score was computed using the clinical and laboratory data from the first day of admission. The MODS score varied from 2 to 16 with a mean score of 14.56 ± 2.32. Forty-two percent of CIP had PaO2/FiO2 in the range of 226–300, platelet count 103/mm3 > 120 (60.0%), pressure adjusted heart rate 0–10 (58.3%), Glasgow Coma Scale 13–14 (41.1%), serum creatinine in mg/dl (µmol/L) < 1.1 (51.1%), and serum bilirubin < 1.2 mg/dl (67.2%).
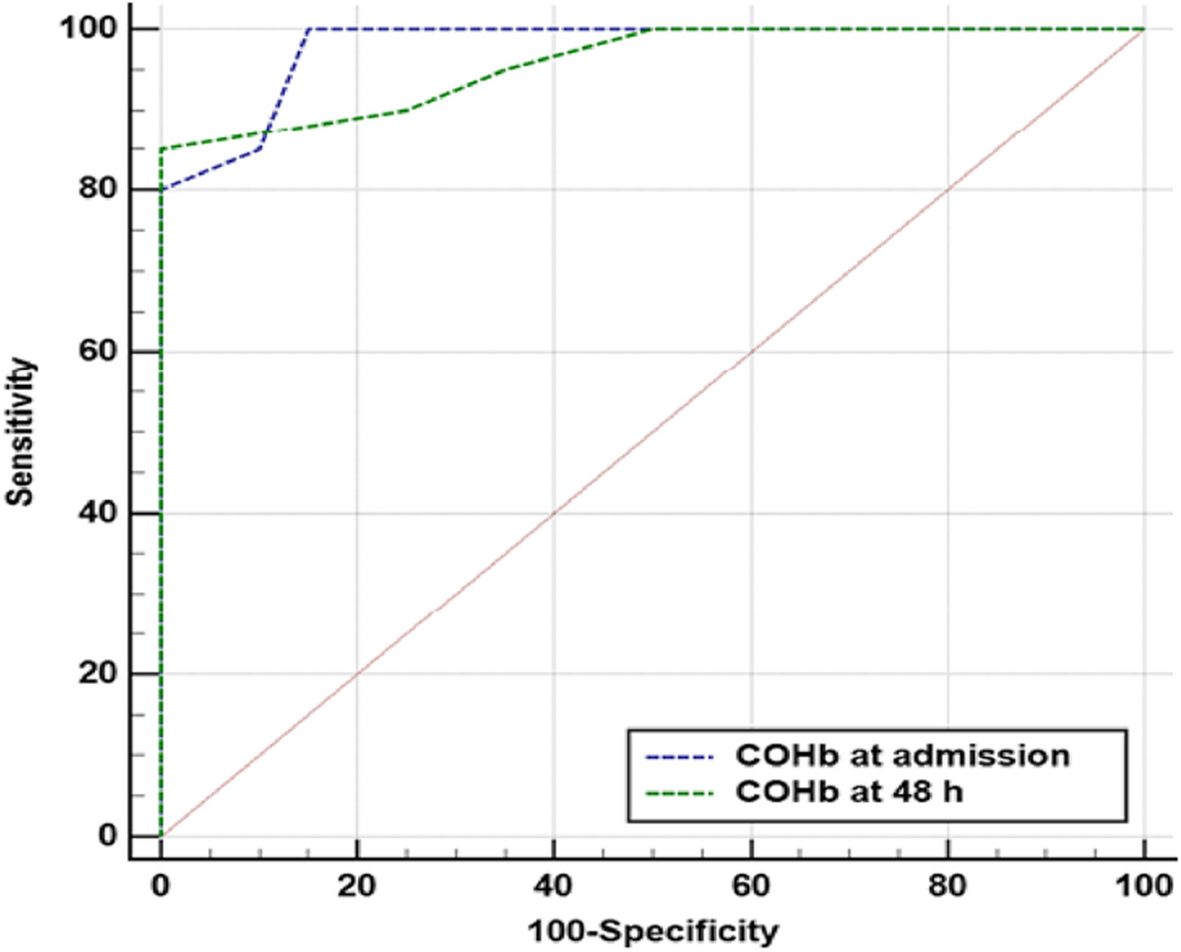
There was statistically significant positive correlation between total MODS score and total number of plasma transfusion with p-value = 0.001. MODS score for assessment of disease severity among CIP who received plasma transfusion has cut-off point 9 with 88.6% sensitivity, 96.4% specificity, 95%CI, area under the curve = 0.970, and p-value < 0.001 as presented in Fig. 2.
Fig. 2
ROC curve analysis of MODS score in assessment of disease severity in critically ill children who received plasma transfusion
As the respiratory conditions were the commonest reason for PICU admission, it was mandatory to study the need for respiratory support, as well as its degree and duration. Out of the enrolled 180 CIP, 145 required respiratory support either as mechanical ventilation (MV), continuous positive airway pressure (CPAP), or nasal prong. Mechanical ventilation was initiated in 81.1% of the studied patients with mean duration of 8.58 ± 4.64 days. Meanwhile and through-out their LOS, 53.9% and 12.8% of the enrolled CIP were in need for CPAP and nasal prong with mean durations of 2.74 ± 1.42 and 3.41 ± 1.85 days, respectively.
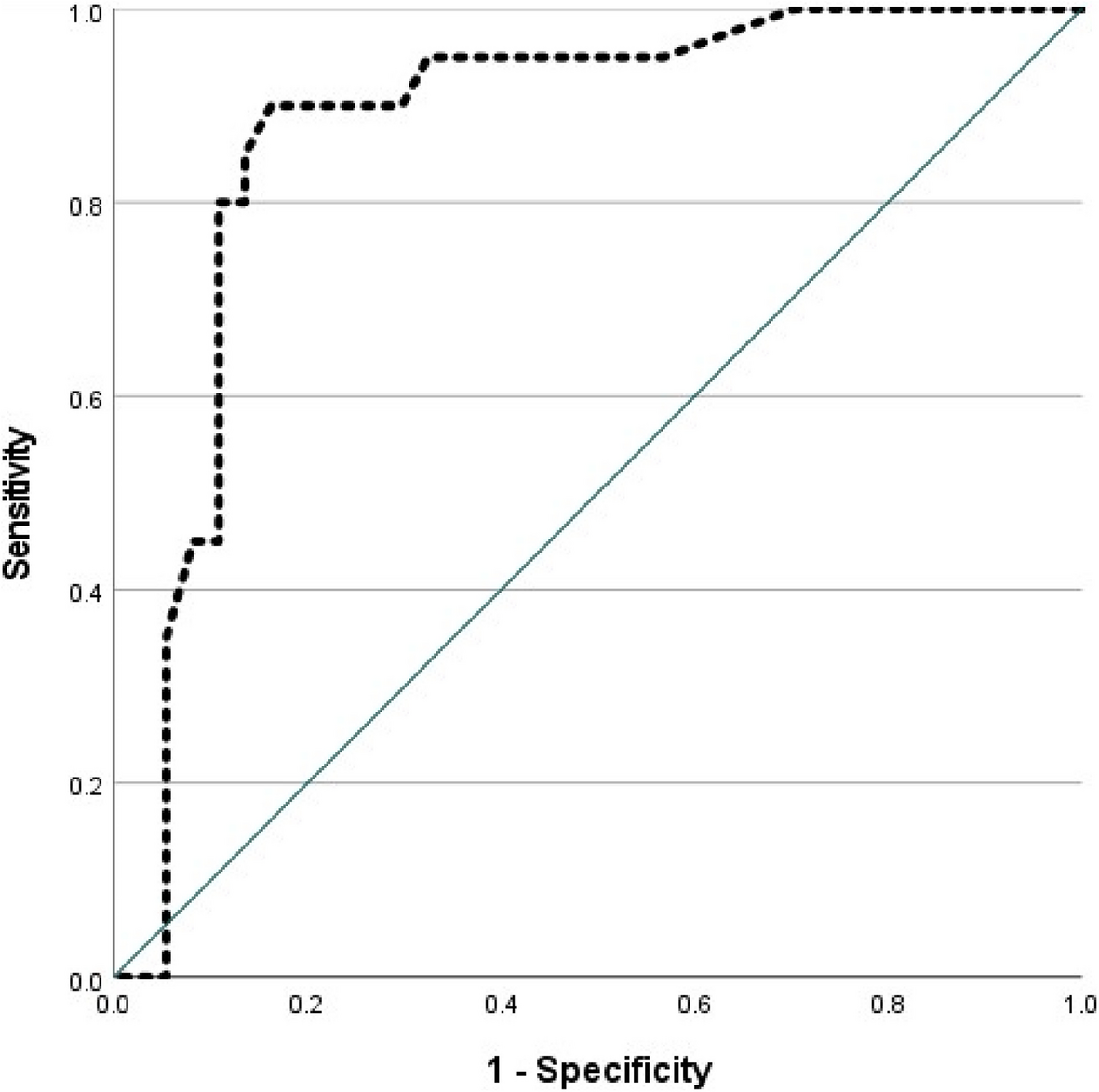
The mean LOS in the PICU was 10.36 ± 5.05 days. There was no statistically significant difference between children with coagulation disorders and children with no coagulation disorders regarding LOS with p-value = 0.605. There was statistically positive correlation between time interval between admission and 1st plasma transfusion and LOS with p-value < 0.001 as presented in Fig. 3.
Fig. 3
Correlation between the time interval from admission to the first plasma transfusion and length of stay
Regarding the outcome of plasma transfusion in the studied CIP, 110 (61.1%) survived till the time of discharge from the PICU, while 70 (38.9%) died. There was a statistically significant difference among survived and died CIP as regarding the total number of transfusions (being more in children who died later) and volume of transfusion (more in survived children) with p-value < 0.001 as presented in Table 4.
Table 4 Relation of number of plasma transfusion and outcomeThere was a statistically significant difference between survived and died CIP who received plasma transfusion regarding Hb, PLT, PT, and INR before plasma transfusion with p-value = 0.016, 0.004, 0.038, and 0.009, respectively. There was a statistically significant difference between survived and non-survived CIP who received plasma transfusion regarding PLT, PT, and INR after plasma transfusion with p-value < 0.001, 0.004, and < 0.001, respectively. Survived CIP experienced more increase in platelet count and decrease in PT and INR after plasma transfusion than dead children as presented in Table 5.
Table 5 Relationship between the outcome of plasma transfusion and laboratory results in the study group before and after plasma transfusionThere was a statistically significant difference between survived and non-survived CIP who received plasma transfusion as regards the total MODS score and duration of MV being more in died CIP with p-value < 0.001 and = 0.004, respectively as presented in Table 5.
Comments (0)