In the present study, we observed the excellent therapeutic efficacy of CT-guided cervical disc RFA for the treatment of neck pain induced by cervical disc herniation, suggesting that method may be a promising treatment. To our knowledge, this is the first report of CT-guided RFA therapy for cervical disc herniation aimed at relieving neck pain by destroying sinuvertebral nerves, and the results showed that this treatment strategy is promising. Although the study was retrospective, the inclusion of > 160 patients makes the results even more convincing.
Cervical disc herniation is one of the most common causes of neck pain [21]. Current clinical treatment includes conservative treatment (medication and physical therapy), epidural injections (interlaminar or transforaminal), minimally invasive techniques and classical surgery (anterior cervical surgery, cervical disc replacement, anterior cervical fusion surgery or artificial cervical intervertebral disc replacement). In most cases, nonoperative treatment is effective. However, some patients do not respond to conservative treatment. For patients with cervical disc herniation, minimally invasive techniques are the preferred choice to reduce risk and reduce hospital stay. Intervertebral discectomy under intervertebral foramen endoscope is widely used for the treatment of patients with cervical disc herniation complicated with radiculopathy, spinal cord compression and/or myelopathy by removing the source of spinal cord compression, resulting in rapid relief of symptoms of axial neck pain and radiculopathy or myelopathy simultaneously. Although for most patients, the intervertebral foramen endoscope strategy is safe and effective, it can induce complications such as scar adhesion and decreased vertebral stability in the long term due to disc destruction and spine structure.
For patients with mild cervical intervertebral disc herniation, the intervertebral foramen endoscope is not the first choice. Many efforts have been made to develop more minimally invasive surgery. Cervical percutaneous discectomy by chemonucleolysis is one of the effective percutaneous disc treatments that aims to partially dissolve the nucleus pulposus, decrease intradiscal pressure and induce disc shrinkage with the advantages of shorter hospitalization, less tissue disruption, less risk, less or no postoperative adhesions, no skin scar, no risk of instability and shorter recovery period. However, chymopapain may induce an anaphylactic reaction [13], and pure ethanol had a short-lived effect with rapid leakage [22].
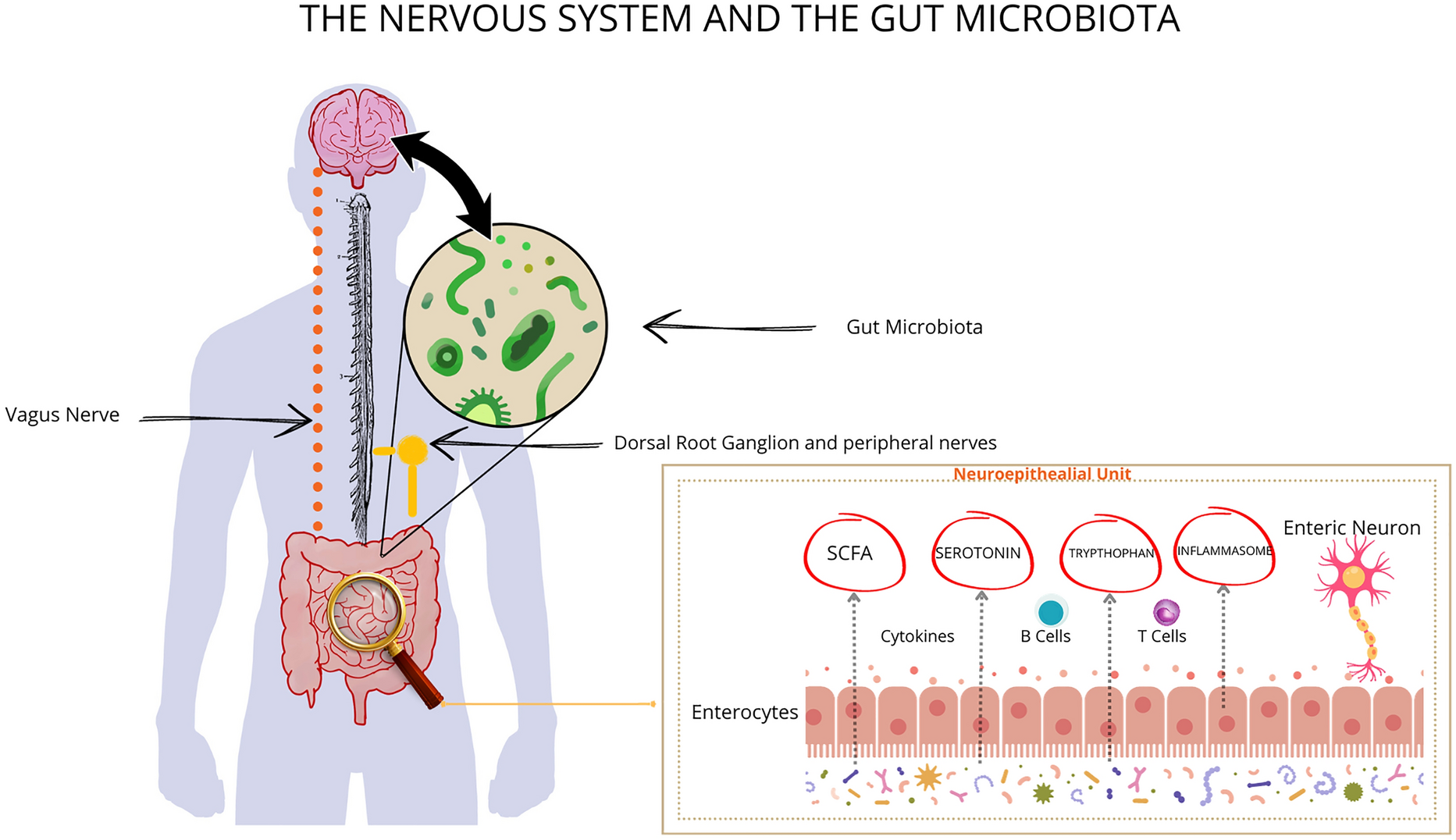
Cervical discs receive innervation posteriorly from sinuvertebral nerves, laterally from the vertebral nerve and anteriorly from sympathetic trunks [16, 23].
According to anatomy textbooks, the sinuvertebral nerve arises bilaterally from the ventral ramus of each spinal nerve just distal to the dorsal root ganglia, supplying both proprioceptive and nociceptive fibers. It is formed by the union of a somatic root from the ventral ramus and an autonomic root provided by the gray ramus (A). The sinuvertebral nerve takes a recurrent course and reenters the spinal canal through the intervertebral foramen. Kojima et al. reported that the nerve divides into superficial and deep networks around the longitudinal posterior ligament, providing sensation to the posterior annulus [24]. In healthy patients, the sinuvertebral nerves are located in the three outer layers of the annulus fibrosus, penetrating about 3 mm through the anulus [25, 26]. However, in degenerative discs, sinuvertebral nerves penetrate into the inner one third layer of the annulus fibrosus, even the nucleus pulposus [1, 27]. Sinuvertebral nerves have been found to be associated with discogenic low back pain in most previous research [18, 19]. In recent years, researchers have found that sinuvertebral nerves were associated with cervicogenic headaches [28, 29].
RFA, known as radiofrequency ablation, was first described by Kirschner in the early 1930s with thermocoagulation of the Gasserian ganglion for the treatment of trigeminal neuralgia [30]. The continuous radiofrequency current created a focal thermal lesion in a neural pathway with the goal of interrupting nociception. RFA has been widely applied for the treatment of specific pain syndromes. For example, Lord et al. demonstrated that percutaneous radiofrequency neurotomy could be used successfully for chronic cervical zygapophyseal joint pain [31]. RFA is also used for the treatment of back pain induced by degenerative disc disease. Kim et al. reported that RFA of the sinuvertebral nerves relieved paravertebral muscle spasms in patients with chronic discogenic back pain.
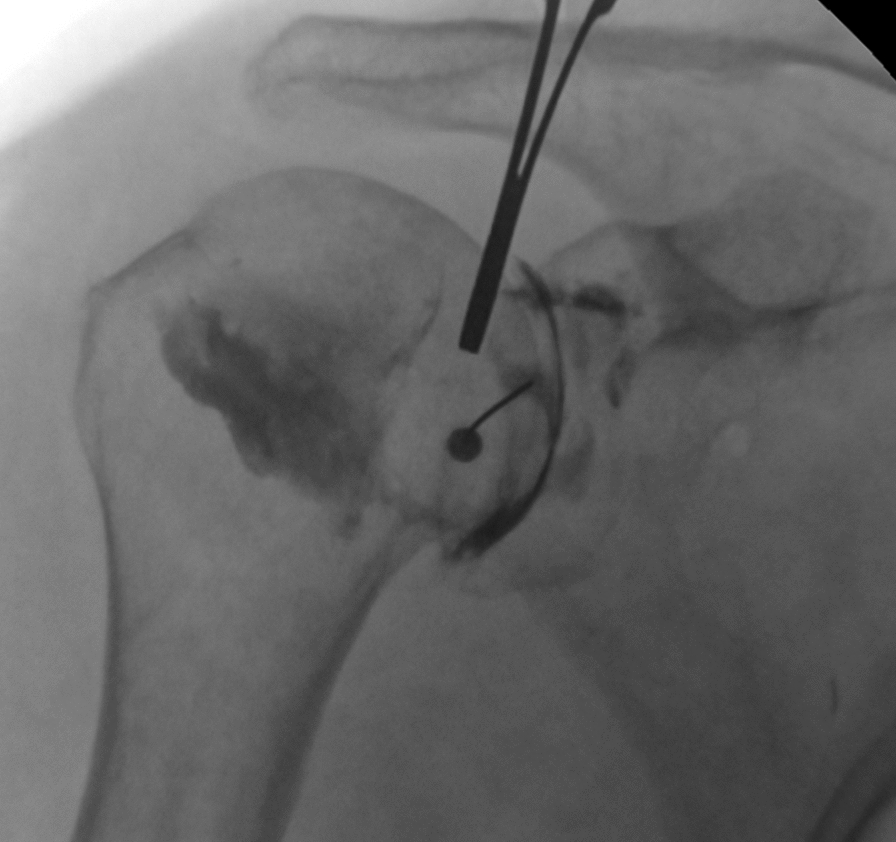
Compared to interventions for lumbar back pain treatment, neck pain treatment is challenging because of surgically related anatomic limitations and the risk of technique-associated thermal injury to the cervical nerve root [18, 20]. With the development of the image, CT guidance provides a clear review of the vessels and intervertebral discs, allowing for precise and safe positioning of a needle tip during the RFA procedure. The application of CT-guided interventional therapy for the treatment of neck pain induced by cervical disc degeneration has been widely accepted. However, few studies have evaluated the pain relief and complications of CT-guided RFA by targeting sinuvertebral nerves for the treatment of neck pain induced by cervical disc herniation.
Complications such as nerve root injury during the procedure were the major concern regarding its application at the cervical level. In the present study, none of the patients showed signs of nerve root injury symptoms during or after RFA treatment. A total of 18 patients reported soreness at the needle insertion site, but it disappeared 2 weeks postoperatively, suggesting that it is not associated with nerve root injury. Some limitations of the study need to be acknowledged. First, we only followed up all patients for a 6-month postoperative period, so we cannot claim that the technique was effective at relieving this kind of pain for a much longer period. Second, although the NRS score pain rating system was widely used as a gauge, we cannot eliminate the subjective preference of patients for their own pain ratings.


留言 (0)