In the current prospective long-term follow-up analysis, we described the outcome of 400 CNO patients up to 4 years, disease trajectories, and factors associated with the outcome.
We compared the NPRD to other published CNO cohorts [2, 4, 6,7,8,9, 16]. We found a slightly lower proportion of patients with multifocal disease as a potential marker of disease severity (clinically 48% of patients and MRI defined 65% of patients compared to 57–93% [7, 16] in other cohorts (Additional file 3)). Patients with active disease at final follow-up range from 22 to 66% in the Huber and Wipff cohort, compared to 38% in the current analysis [7, 16].
Measuring disease activity
For the individual patient and in this prospectively followed cohort, the PedCNO score seems to be a reasonable tool for estimating ongoing changes in disease activity and treatment response. The initial findings of Beck et al. could be confirmed [10]: as shown in Table 5, the percentages of patients reaching certain levels of PedCNO score improve over time are consistent with the number of patients with decreasing activity of disease over time (as defined by MRI counted lesions; clinical lesions; PDGA). Forty percent of the patients with active disease reach a PedCNO70 during the following year. We conclude that best predictive and significantly changing parameters for disease activity estimation during follow-up inside the PedCNO score are MRI-defined lesions and the PGDA over time, in addition to the C-HAQ (Figs. 2b and 3). Even though the latter has not been designed or validated for CNO, the components of patients’ global disease estimation and pain contribute significantly to this score [17]. The C-HAQ score is known to have a ceiling effect in patients with juvenile idiopathic arthritis (JIA) and CNO [18, 19]. In our cohort, it still documents changes over time and, thus, was responsive in about half of the patients—albeit in a low score range. Patient global and pain scores alone were not responsive after 1 year of therapy and during further follow-up (Fig. 4) [20].
Pustular skin disease is a relevant component or comorbidity of CNO [4]. In the registry, the number of patients with pustulosis/acne-like skin disease did not change over time, while the proportion of IBD in CNO patients even raised during disease course.
The definition of remission in CNO is still unclear. In addition, it is unresolved, whether potential criteria for such a definition—solely or combined—would reliably describe the absence of disease activity over years. There is a definite clinical need to find a reliable and hopefully easy to use clinical severity scoring system including. We analyzed different single scores or criteria possibly describing inactive disease from both patients’ and physicians’ perspectives:
Patients’ pain score < 1
During 4 years of follow-up, about half of the patients reported absence of pain. As reported previously, this item changes rapidly in the first few weeks after NSAID therapy is instituted [10]. After 1 year, no further changes were noted in this low range of symptom severity. This may limit its meaningfulness and responsiveness for defining inactivity. On the other hand, patients may still feel pain after years, even though no lesions are detectable in MRI and no clinical pathologies are found. Pain amplification syndrome has been reported in CNO in this regard [21]. About half of the patients still report pain (NRS ≥ 1) after 1 year and longer at a mean NRS around 2. From the second year on, pain rating was not correlated to further improvement of numbers of lesions, neither clinically defined nor by MRI.
Patients’ overall well-being < 1
Almost comparable to the pain score, during the initial year this criterion covers improvement of disease but fails to describe the patients’ improvement later, especially if the PDGA would be suggested for comparison as the “gold standard of disease activity” estimation. Almost 60% of patients do not reach a patients’ global level below “one” after 4 years, while only 38% of patients had visible bone manifestations in the MRI at that time. Nevertheless, the patients’ view on her/his own disease is of utmost importance.
Physicians’ global disease assessment PGDA < 1
After 4 years, physicians reported “no disease activity” in 75% of patients. A PGDA < 1 may come closest to patient’s or MRI defined absent number of lesions (n = 0) suggesting inactive disease. Of note, certainly the PDGA is influenced by the physician’s knowledge of the MRI results as a potential bias (r = 0.3, Additional file 4). Most improvement of this parameter is seen in the first year of observation, and it continues to decline throughout follow-up.
Inactive disease as defined by absent whole body MRI lesions
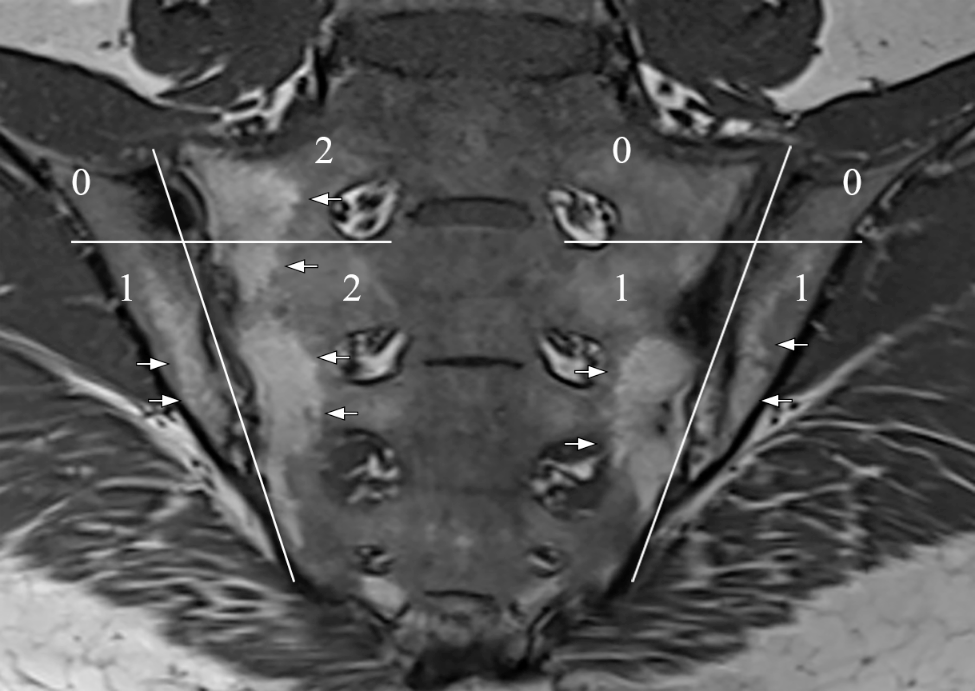
Sixty percent of patients reach this target after 4 years (lesions n = 0). MRI definition of lesions seems more sensitive than the patients’/physicians’ clinical notice of lesions, but it may overstate the clinical relevance of a T2-positive TIRM/STIR-MRI lesion with regard to inflammation. Nevertheless, based on the literature, a T2 active lesion seems to be of relevance for the patients’ disease activity even after years of follow-up [22]. For now, it seems not entirely clear whether the mere detection of a fat saturated T2-TIRM/STIR signal necessarily implements present disease activity especially late in the CNO course [23]. Of note, 40% of the patients still show active inflammation/TIRM positive signals in MRI after 4 years, whereas 33% of patients do notice these lesions as active (Fig. 1). Thus, at least to some extent (up to 7% in the current cohort), MRI may “overstate” the activity of the lesions if the clinical notice of a lesion is prioritized.
Predictors for severe disease courseSpecifics of locations and number of lesions
In general, CNO affects any bone of the body [24, 25] (the neurocranium remains exceptional [26]). Therefore, a detailed analysis of the location of inflammation was performed. During the course of the disease, inflamed lesions were predominately present on the lower extremity and the clavicle. A risk for severe course of disease (defined by PGDA ≥ 4) was identified through statistical correlation when lesions were present in the pelvis and femur at baseline.
Patients with a higher number of lesions exhibited a prolonged and severe course of disease. Each additional affected bone at baseline increased the risk of severe disease course by 19% (OR 1.19, p < 0.001). A multifocal pattern (defined as lesions ≥ 2) at baseline was found to have the highest predictive value for severe disease; it increases the risk of severe disease course by 150% (OR 2.48, p = 0.002).
Laboratory parameters of inflammation
The ESR is one of five parameters in the clinical PedCNO score. Our data now shows that an elevated ESR is associated with a higher disease activity over time. Each mm/h elevation of ESR increases this risk by 3% (OR 1.03%, p = 0.024).
We conclude that patients with certain baseline parameters like lesions at the femur or pelvis, high number of lesions (MRI-defined), or elevated ESR have a particular higher long-term risk for severe disease. Of interest, patients with initially assumed “severe” disease due to vertebral lesions had a favorable outcome and no increased risk for a severe long-term disease. One explanation might be that these patients usually are intensively treated by using bisphosphonates. This finding underlines the importance of defining patients with a putative risk for a severe course. The current analysis suggests considering an intensified treatment for patients with multifocal lesions and femoral or pelvic lesions. Nonetheless, such considerations should be analyzed through controlled prospective trials.
Therapy
While NSAIDs remained an important tool in treatment plans over the years, the use of steroids almost diminished completely over time in our cohort. Most patients have an uncomplicated course of disease and are treated with NSAIDs (86% initially). Generally, escalation of therapy was necessary only in a limited number of patients. These patients are often no longer treated with NSAIDs: So, in the first year, about one third of the patients is treated with DMARDs, raising up to 55% in the 4-year follow-up. In the meanwhile, 40% of patients receive NSAIDs in the fifth year. Prolonged treatment was less based on NSAIDs. However, it is still unknown whether and when stopping of NSAIDs is reasonable. The only existing prospective study by Beck et al. [10] so far pointed out NSAID effectiveness in the first year of disease [10]. Long-term data of this controlled prospective cohort is so far preliminary reported [9]. Bisphosphonate application is rather used during the first years of disease, indicating that bisphosphonates are considered predominantly for an initial “remission induction” therapy but not as a long-term continuous treatment. So, the proportion of patients with bisphosphonate treatment continuously declined, in line with fewer patients affected by lesions of the vertebrae. We consider that patients with vertebral lesions are being treated differently in the beginning compared to those patients affected by peripheral lesions. In general, patients with CNO were in a good clinical condition after 1 year (patient well-being NRS ranged around 2 (of 10) over the years; C-HAQ of zero in 2/3 of the patients after 2 years of treatment). Schnabel et al. [5] highlighted the risk of relapse in the third year of disease. To date, there is no consensus how to design an optimal disease controlling and flare preventing strategy.
When treatment strategies would only be based on patient-reported pain and numbers of clinical lesions, there may be a risk of overtreatment especially for patients affected by pain amplification syndromes or undertreatment of those with persistent bone inflammation without symptoms. On the other hand, if the presence of “active” lesions in MRI might be the only rationale of treatment, the patient may also face the risk of overtreatment in the long run. Risk factors for severe disease course (multifocal disease, inflammation of pelvis/femur at disease start, high ESR at baseline), as defined in the current study, may be considered for treatment decisions: This might lead to the assumption that intensive treatment of femur/pelvis/multifocal disease following a CNO treat-to target (T2T) strategy already in the beginning of disease might lead to a better clinical outcome for these patients, similar to the patients with vertebral lesions in this cohort. Currently, the international CARRA consensus treatment plans do not include such an additional controlled option for particular “risk” lesions, aside from the vertebral lesion [19]. It certainly seems worth defining prospective outcome parameters through larger prospective and controlled studies defining those patients, who may need particular ways of therapeutic strategies including early escalation of therapy. The NPRD cannot follow and evaluate treatment efficacy in such a controlled setting. Nevertheless, the current analysis might give implications for the set-up of treat-to-target protocols or controlled trials in international efforts [19].
Growth development
In the previous first-year analysis of the NPRD cohort, a significant increase of CNO affected children with a growth retardation below the 3rd percentile and weight below the 3rd percentile of the standard cohort was noted, affecting around 8% of patients [2] compared to the national reference cohort [13]. The current analysis of anthropometric data (height, weight, BMI) of the cohort implies that some CNO patients start out small and may stay small and light-weighted over the time. A significant gain of weight/height after instituting effective therapy strategies, as confirmed by several means of disease activity, could not be seen in these patients. On the other hand, low height and weight at inclusion were no predictors for severe disease course. These findings allow several possible interpretations that need further investigations: some CNO patients may be affected by a constitutive energy consuming pathophysiology that is impairing appropriate growth and is still present even after effective therapy. Treatment did not alter this pattern over time. However, a further decline in length and weight was not documented. Inflammation in conjunction with metabolic energy consuming processes might play a role in CNO [27, 28]. Due to the limited number of patients, this finding may not be overinterpreted. So far, only a few patients with a monogenetic disease background mimicking CNO and also affecting growth restrictions have been reported, like hypophosphatasia and Majeed syndrome [28, 29]. In daily pediatric practice, low weight and height should prompt the caring physician to consider further metabolic or genetic diagnostic approaches in CNO. In addition, these findings emphasize the necessity of an early CNO diagnosis and treatment to prevent a possible further decline in growth characteristics.
Limitations of the analysis
In comparison to other cohorts, the patients in the registry do have a slightly lower average MRI lesion number. Possible causes are the delay of inclusion into the registry (5.8 months after first contact to pediatric rheumatologist). There still might be a bias by the shrinking size of patient numbers/lesions over time by losing manifestation locations with lower frequencies. There was a remarkable number of patients who was not followed for the entire 4 years in the registry. We could not find any sociodemographic or clinical parameter that was associated with the likelihood of drop-out. Therefore, the longitudinal data analysis by linear mixed models results in unbiased effect estimates in presence of missing parameters. In addition, we cannot provide data about treatment effectiveness and reasons for discontinuation in this longitudinal data analysis. Measurements of disease activity at treatment start as well as reasons for discontinuation are not collected; only the presentation of patients at the visit is documented in the NPRD.



Comments (0)