
記住我


Post-traumatic stress symptoms (PTSS) are associated with significant child and family psychological distress after injury [1,2,3]. PTSS affects children’s functioning after injury and may include psychological symptoms such as dissociation, avoidance, intrusive thoughts, hyperarousal, and irritability and physical symptoms such as sleep disturbance [4]. Between 25 and 57% of injured children develop significant PTSS [5, 6]. Thus, PTSS following pediatric injury represents a substantial health burden as 3.5 million children sought emergency department care after injury in the USA in 2020 with over 121,994 children under 17 years of age hospitalized for non-fatal injuries [7]. Risk factors for PTSS include pre-injury child adjustment problems such as anxiety, post-injury reactions to the trauma, subjective life threat and fear, low social support and parental PTSS [8,9,10,11,12]. Interestingly, injury severity itself is not associated with development of PTSS symptoms [13]. Because PTSS develops after children are discharged from the hospital, these symptoms are frequently not visible to the trauma system and, thus, may go unrecognized. A study by Newgard and colleagues examining pediatric deaths after admission to the ED for injury showed that self-harm in the year following injury was one of the leading causes of death, underscoring the need for mental health services integrated into the trauma system [14]. Thus, a screening method and a brief, effective treatment that could be delivered through the trauma system has the potential to fill a needed gap in therapy.
Evidence-based therapies for PTSS do exist. Cognitive behavioral therapy (CBT) is an evidence-based treatment that has shown greater improvement than supportive child-centered therapies for childhood anxiety and behavioral problems in general and for children with PTSS in particular [15, 16]. Evidence-based treatments such as CBT [17,18,19,20] typically include education about emotions, identifying and modifying negative thoughts and appraisals, and training in coping skills and relaxation and may include trauma exposure to reduce anxiety and fear (e.g., graded exposure, reducing avoidance) [18, 19]. Trauma-focused CBT was developed to intervene following a range of specific traumas, including interpersonal violence, accidents and injuries, or exposure to/witnessing events occurring to others [17, 21]. Trauma-focused CBT addresses trauma impact using components of CBT and recounting of the trauma narrative to address cognitive distortions and provide exposure to the child’s personal trauma experience. As children retell their experience, they apply the CBT skills that they have learned to restructure and master the response to their memories [18]. The trauma narrative provides children with tools to engage with trauma memory, organize and articulate a positive interpretation of their trauma story, and modify basic core beliefs about the world [21]. Community access to these evidence-based treatments for PTSS is limited in many regions due to families’ lack of health insurance coverage and a paucity of providers especially in more rural areas [22].
eHealth approaches may improve access and reduce barriers to care. eHealth delivers psychological therapy to children and adults with a variety of conditions including PTSD, anxiety, and traumatic brain injury with comparable efficacy to face-to-face approaches [23]. Online alone preventive treatment for PTSS has been successful in a small pilot [10]; however, therapist involvement for treatment may be associated with larger treatment effects [24]. eHealth approaches may also improve access to care especially in rural communities and reduce barriers including the stigma sometimes associated with seeking mental health care [25]. Translating existing PTSS treatments to a therapist-involved eHealth delivery system may substantially improve access to and participation in treatment without reducing efficacy. Many trauma systems, especially those with large rural catchment areas, have active telehealth programs into which an eHealth therapy program could be integrated [26], thereby improving widespread dissemination and implementation [27].
We have developed an online psychoeducational program that includes web-based psychoeducation about PTSS and elements of CBT (e.g., stress management strategies, reframing unhelpful thoughts) with sharing the trauma narrative and graded exposures to the most distressing memories of the experience. The online content is accompanied by weekly meetings with a therapist via videoconference. If successful, these methods could be integrated into trauma systems with existing telehealth programs, providing a systems-level intervention.
ObjectivesThe goal of the current randomized controlled trial is to evaluate the Reducing Trauma After Stress (ReSeT) program. ReSeT is a therapist-involved online intervention that incorporates both elements of CBT and graded exposures for children with post-traumatic stress who have been hospitalized following an injury. ReSeT provides online education about post-traumatic stress, identifying and managing feelings, and teaches coping skills which are then used to process the exposure through the trauma narrative. Support is provided by a therapist in weekly online meetings. The goal is to improve children’s psychological outcome after a traumatic injury and give them tools to manage future challenges.
Aims and hypothesesThis study was designed to test the efficacy of ReSeT to reduce PTSS after hospitalization for an injury compared to usual care among children who have elevated symptoms of PTSS at 4 weeks post-injury. Our first aim is to compare the groups on the outcome of PTSS at 10 weeks and 6 months post-randomization as measured by the Child PTSD Scale (CPSS) [28]. Second, we will explore whether child pre-existing psychological health modifies outcomes. Third, we will examine whether there is heterogeneity of treatment effects among subgroups including those with a higher initial symptom burden compared to those with a lower symptom burden, age, and sex.
We hypothesize that children who receive the ReSeT intervention will have a clinically important and statistically significant reduction in symptoms at 10 weeks post-randomization (primary outcome), and this effect will be shown to be durable at 6 months. Finally, we expect that we will find heterogeneity of treatment effect among subgroups of children including those with a higher symptom burden, and those with higher levels of pre-existing psychological problems and with lower functioning families.
Study designThis is a multicentered randomized controlled trial with a 1:1 assignment of the intervention (ReSeT) to control (usual care) that aims to evaluate whether ReSeT is superior to usual care in reducing children’s symptom levels. The intervention lasts 8 weeks. Outcome assessment occurs 1-week post- injury (baseline or pre-injury measure), with assessment for trial entry (elevated stress) at 4 weeks post-injury. The primary study outcome is assessed at the completion of the intervention (10 weeks post-randomization) and durability of effect is assessed at 6 months post-randomization. This study was registered at ClinicalTrials.gov (NCT04838977) 8 April 2021. Study investigators are handling all aspects of trial management including training of research coordinators, monitoring enrollment, and checking data quality. Investigators meet bi-weekly to review subject accrual, monitor processes, and discuss any potential needed protocol modifications. Data are managed by the Utah Data Coordinating Center at the University of Utah who developed and maintain the REDCap database.
SettingChildren are recruited from four level 1 pediatric trauma centers in the USA: Cincinnati Children’s Hospital and Medical Center (Cincinnati, Ohio); Children’s Memorial Hermann Hospital (Houston, Texas); Nationwide Children’s Hospital (Columbus, Ohio); and, Primary Children’s Hospital (Salt Lake City, Utah). Level 1 trauma centers are regional referral hospitals that are capable of providing all aspects of trauma care from prevention through rehabilitation. Children are recruited from the inpatient wards including the pediatric intensive care unit, the surgical unit, and the short stay units (< 23 h hospital admissions).
Participant eligibility, recruitment, enrollment and randomizationEligibilityChildren aged 8 to 17 years hospitalized for trauma are eligible for the study. To be included, children and at least one parent must speak English and have broadband internet availability at their home address. Children with broadband availability but without an internet subscription or computer will be provided with a tablet and internet subscription. Children may not have moderate or severe TBI, as defined by a Glasgow Coma Score of < 13 as these children may find it difficult to participate in therapy. Exclusionary criteria include pre-existing severe psychiatric problems requiring hospitalization; developmental disorders which would preclude participation in therapy; children injured by abuse or through interpersonal violence or a self-inflicted injury; children currently receiving psychotherapy; children hospitalized for over 30 days; and children injured in an event where there was a death of a family member or friend.
Recruitment and enrolmentResearch coordinators screen all hospital trauma admissions daily using the electronic medical record. Families are then approached in person or by telephone to confirm eligibility and request verbal consent to participate in the study. Families who are missed are contacted by postal mail to inform them about the study. Families who agree to participate are sent a link to a REDCap (Research Electronic Data Capture) website 1 week following injury and they are asked to fill in baseline information including demographics and study outcomes to obtain baseline measures. Study measures are shown in Table 1.
Table 1 Schedule of enrolment, interventions and assessmentsParents and children are asked to complete a measure of child PTSS, the Child PTSD Scale (CPSS), at 1 week and 4 weeks post-injury [28]. The CPSS was selected as it is a well-established open source questionnaire with favorable sensitivity and specific for identifying PTSS and predicting children’s response to treatment that has been used previously in similar populations [10, 29]. To assess the child’s stress symptoms, the highest value of the parent or child’s response to each item on the CPSS are summed. If the sum is greater or equal to 11 at 4 weeks post-injury, the child is eligible for randomization. The summed value is used as parents may be unaware of children’s internalizing symptoms and children may self-report low values on some items due to avoidance as suggested by Mai and Scheeringa [30]. Families whose child has a CPSS ≥ 11 meet with the research coordinator for their site via videoconference to recheck eligibility requirements and to review the full trial information. After time to ask any remaining questions or consult with other family members, parents are asked to complete informed consent via a REDCap module and children are asked for assent. After informed consent and assent, the family is enrolled in the trial and proceeds to randomization. There are no additional consent provisions. Figure 1 shows the consort diagram from recruitment through follow-up.
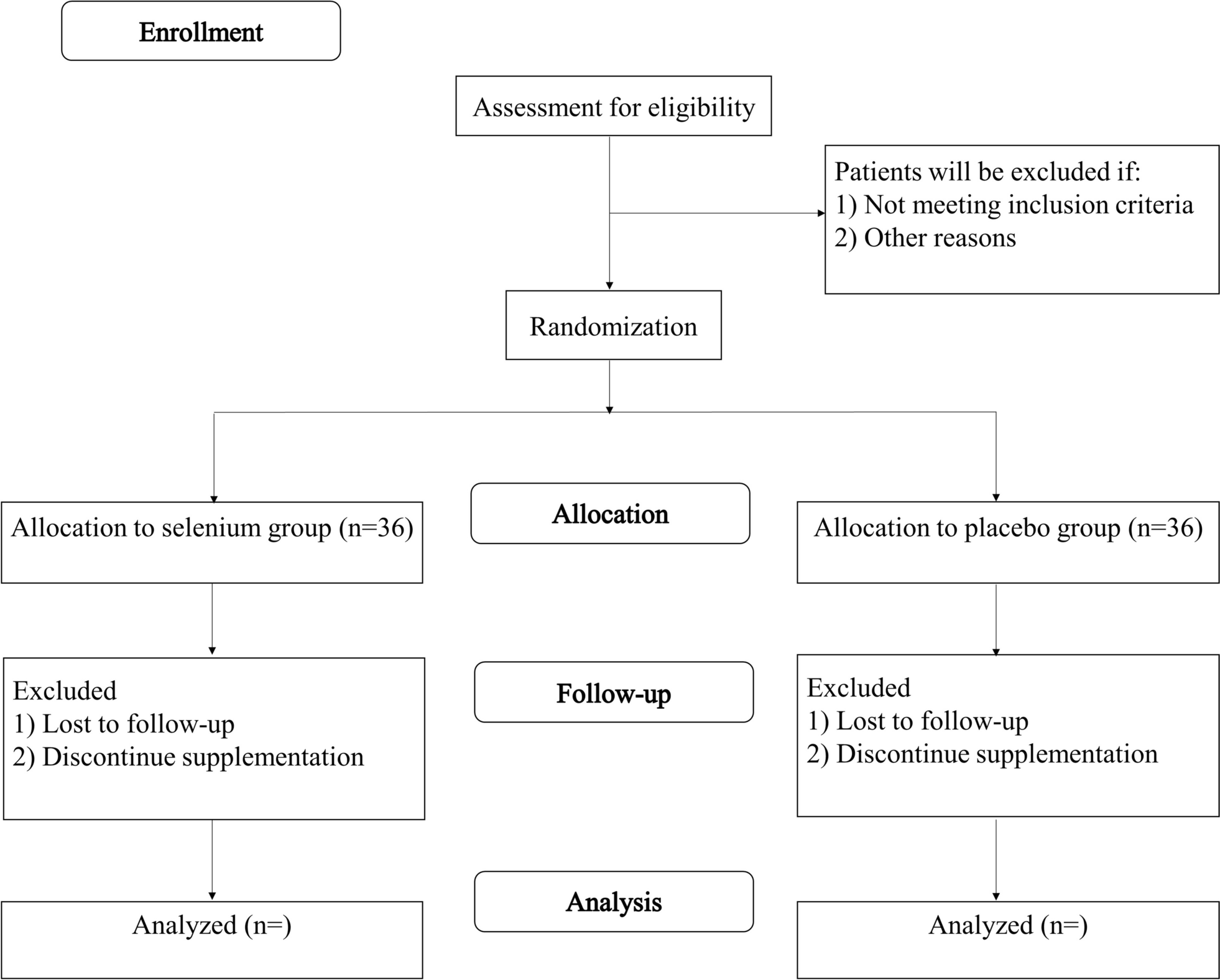
Fig. 1
ReSeT flow chart from recruitment through completion
RandomizationRandomization occurs at the time of the 4-week CPSS. One hundred and six children will be randomized from the participating centers using a computer-generated random assignment sequence prepared by the study statistician and uploaded into the REDCap randomization module. Stratification will occur by site and by age group (8–11 years, 12–17 years). Randomization is conducted while the coordinator is speaking with the family via videoconference in order to enable a “warm handoff” to the therapist for families randomized to the treatment group. The randomization sequence is not visible to the research coordinators.
InterventionThe ReSeT intervention includes 8 online psychoeducational sessions with each session followed by a meeting with a post-doctoral psychology fellow or a doctorate level psychology student supervised by a psychologist with expertise in trauma intervention. The psychoeducational content is delivered online from a dedicated website that has a logon for each individual. Each of the 8 sessions has 3–4 short interactive videos to help children learn the concepts being taught. Concepts are reinforced with brief homework assignments. The therapist meetings are conducted via HIPAA compliant video conferencing. Parents are asked to attend therapy sessions with children younger than age 11 years and may meet the therapist before and after the session for older children as outcomes have been shown to improve with parent involvement [31].
In the first session, the therapist goes through the online video content with the child and parent to teach them about the program and trouble shoot problems that families may have with the technology. After this initial visit, the next three sessions focus on aspects of cognitive behavioral therapy including understanding feelings, identifying helpful and unhelpful thoughts, understanding that thoughts can change outcomes, and cognitive reframing. Videos for each session engage children in learning the concepts and learning skills that they are then able to practice with the therapist and at home including belly breathing, positive imagery, cognitive reframing, and using feelings thermometers to rate the intensity of feelings and the effectiveness of stress management therapies. Videos include interactive content to engage children. Children may go to the ReSeT website to practice skills using the videos as often as they wish and are asked to rate their feelings with the feeling thermometer on the website. Sessions 5 to 7 involve telling the most stressful or scary aspects of the trauma narrative while practicing stress management techniques to allow desensitization to the trauma. The video content shows a child who was injured sharing her trauma narrative with the therapist. The videos show the child creating a hierarchy of least scary to most scary events after injury, and working through the hierarchy with therapist by using the skills that were taught in the prior sessions if she becomes stressed. In the session with the therapist, children build their own trauma narrative hierarchy by identifying and ranking the least to most scary aspects of the trauma and practicing their skills while they talk about what happened. The final session involves a wrap up and resilience plan in which children learn that stress may return and make a plan to manage it. If the parent requests or the therapist feels that the child needs ongoing care after the intervention is completed, appropriate referrals are made by the PI at each site.
Psychoeducational resources for parents are available on the website and include education about self-care for the parent, managing their own stress symptoms, positive parenting and managing child behavior, and managing sleep problems for children. Parents view these resources independently and their completion is not required.
Control subjects will receive usual care. All aspects of care are permitted during the trial, including psychological support. Families are asked whether psychological support was received outside of the ReSeT program at the 10-week and 6-month outcome assessments. Usual care was selected as the comparator as it reflects what children currently receive in the trauma system. Families who request a referral for psychological resources either during or after the completion of the study are given a referral by the site investigator.
Criteria for discontinuing the interventionParticipants are free to discontinue the intervention at any time; however, modification will not be made to the intervention.
Strategies to improve adherenceParticipants are reminded to complete measures using automated REDCap reminders and text messages from the research coordinators. Participants receive a small monetary incentive for completion of trial activities.
Relevant concomitant careWhile we exclude children from the trial if they are currently receiving therapy so as not to interfere with their ongoing care, all types of concomitant care are allowed during the trial including seeking therapy outside of the trial.
Data management and securityWe use REDCap to support this study. REDCap is a secure, web-based, data capture tool, hosted at the University of Utah, which allows participant outcomes to be directly entered by participants. Participants and their parents enter all baseline information including private identifiers and subsequent assessments into REDCap. Study personnel enter medical information from the patients’ charts into the REDCap database. Study personnel may only view participants from their own site. REDCap is programmed with plausible ranges for entered values. The ReSeT website, where participants view the videos, is encrypted and password protected. Each family is given a unique logon and create a password. Each participant is assigned a study ID that is linked to the REDCap database and the ReSeT website. At the time of analysis, an analysis file will be created that merges de-identified information from the ReSeT website and REDCap database by study ID. Data checks are run prior to each DSMB meeting and site research coordinators are asked to source verify any missing variables; however, participants may skip questions in the assessments if they do not wish to respond. The REDCap instance is HIPAA compliant and is housed at the University of Utah’s secure, Federal Information Security Management Act compliant, Data Coordinating Center behind University firewalls.
Quality control measuresTraining research assistantsResearch assistants are trained on the study protocol. Training includes (1) review of the ReSeT manual; (2) use of the REDCap; (3) best practices for communications with families including how to approach families in person, by phone or by text; (4) consent procedures including practice of providing informed consent and using the REDCap consent module. Training materials are kept with updated versions stored in a Box folder accessible to all sites.
Supervision of therapistsTherapists are trained in the use of the website and delivery of therapy. They are trained through reading and discussion of the training manual, viewing video trainings, and discussions with a licensed clinical psychologist. All cases are supervised weekly by two experienced clinical psychologists who helped to develop the intervention. During supervision meetings, each aspect of the completed sessions is discussed and future sessions are planned to ensure fidelity to the manual.
MaskingThis is an unblinded study as it is not feasible to blind the research coordinators, the therapists, or the participants. Participants in the treatment and control groups complete outcome measures by directly entering responses into REDCap and the analysis file is de-identified which reduces the risk of bias from unblinded study personnel. Because this study is not blinded, there are no procedures for unblinding.
Fidelity to treatmentTherapists complete a detailed fidelity checklist after each session to document that each element in the treatment manual for that session is completed. Additional documentation includes the total duration of the session, who attended, and time spent with the participant and the participant’s parent. The therapist also rates the participant’s engagement in the session using a Likert scale.
Baseline measuresParents will be asked to complete family demographic measures including family composition, self-identified race and ethnicity, health insurance status, and income. Parents will be asked to complete measures of family functioning and parental psychological health as these may directly impact children’s recovery [32, 33]. Children complete baseline mental health questionnaires. Both children and parents separately complete a measure of post-traumatic stress reflecting the 1-week post-injury timepoint. Research coordinators will abstract injury information from the chart to include injury mechanism, injury severity score, admission unit and whether there was an operative intervention, and length of stay using a structured format. Abbreviated injury scores will be provided by each hospital’s trauma registrar [34].
Outcome evaluationAll child participants and parents will be asked to complete outcome evaluations through REDCap at 10 weeks and 6 months post-randomization. Participants randomized to the intervention will be asked to complete outcome evaluations regardless of whether they completed all 8 sessions. Table 1 displays schedule of enrolment, interventions and assessments with their timing for participants and their parents. Measures include child physical and psychological health as well as brief measures of family function and parent psychological health as these may affect either children’s likelihood of having PTSS or their response to treatment.
留言 (0)