
Remember me







After a patient has been assessed as eligible based on the abovementioned criteria, the GP provides detailed information about the study objectives, procedures, and potential risks and benefits. Participants are also handed a detailed written patient information document and have the opportunity to ask their GP any questions related to the study. Thereafter, the GP obtains written consent and keeps the record safe in accordance with data protection law requirements.
Additional consent provisions for collection and use of participant data and biological specimensIn addition to the general consent to study participation, participants release their GP by written consent from medical confidentiality for the purpose of transferring their data to the study center.
When participants first register on the intervention LMS, they receive detailed information about data privacy according to the General Data Protection Regulation (GDPR). Their consent to data processing in the LMS is obtained digitally during the registration process and stored in the LMS database in accordance with the legal requirements.
InterventionsExplanation for the choice of comparatorsThe control group follows the same overarching study procedures (i.e., informed consent) and has access to the LMS just like the intervention groups. Potential effects of the study procedures or the LMS environment therefore also affect the control group. However, the control group only receives professionally prepared information but no interactive didactic structure nor any interactive/functional elements within the LMS. There is no coaching and no contact person for content-related questions. The LMS content accessible for the control group is similar to an extended fashion of digital information becoming increasingly available from statutory health insurance websites. Laypersons could assemble the information by intensive literature or Internet search. Hence, the control group thus receives a sham intervention with no expected effect beyond what can currently be found by diligent Internet search.
Nevertheless, the control group is provided with sufficient information and video material to ascertain that the minimum processing and material exposure times explained in the patient information and documents consent remain plausible to avoid suspicion of a placebo intervention in the patients. The control group is also subject to the same adherence mechanisms as the intervention groups. At the study termination, we will inquire patients about their best guess whether they were included in the control or intervention group.
Intervention descriptionAll interventions (including control) are applied through the MiLoCoDaS LMS, a digital online learning platform based on TYPO3. After registration, answering a baseline questionnaire, and automated randomization, participants get access to the content of one of the intervention groups or the control group.
High-intensity interventionParticipants are provided a 12-week closed-group online workshop (webinar) combined with a 12-week interactive digital self-study course that delivers similar and complementary content. The webinar consists of 12 sessions, each approximately 45–90 min, once a week on fixed dates, with 15–25 people per group. The groups, webinar coaches, and dates are constant. Static information materials are additionally provided. This static information material is defined as having not been didactically optimized and laypersons could find the information themselves with intensive literature or Internet search.
The webinars and the self-study course are structured into 12 modules, which build upon each other in terms of content and are completed in chronological order. Each module addresses a specific topic based on typical complaints of patients with post-COVID-19 disease. Central topics among others include coping with everyday life, structuring the day, increasing or pacing physical activity and the ability to relax, coping with pain, promoting acceptance and a positive basic attitude, improving cognitive performance, and the ability to regulate emotions.
The webinars are facilitated by psychological coaches. Only one specific module (Module 2), which deals exclusively with medical information and context (such as symptom correlations or pathophysiological explanations), is facilitated by licensed physicians who have been researching Long COVID since the disease emerged. The psychological coaches were selected and trained by the psychological head investigator. Decisive qualifications were previous academic achievements, especially in the field of clinical and health psychology, additional qualifications (e.g., in the form of additional certificates such as “Coaching and Counselling,” “Conversation Management,” etc.), and previous experience in leading therapeutic groups (e.g., through relevant internships). These coaches then received five standardized and interactive training sessions of 2–3 h each in group format from the psychological head investigator. The coaches were introduced to the content, objectives, and didactic concept of the LMS and given precise instructions on how to structure the online sessions and how to deal with potentially difficult discussion situations. Each coach received a detailed course manual with a precise description of the exercises to be performed, their sequence, duration, details of the discussions to be held, reflections, and psychoeducational input. In addition, they received further training and a compendium on the status quo of knowledge about Long COVID. All irregularities in webinars, whether communicative, organizational, professional, emotional, etc., are discussed with the psychological head investigator in regular supervision sessions.
The digital self-study course has been refined by media-didactic experts and uses elements and gamifications such as quizzes, memory trainings, interactive pain maps, graphical visualization, social network maps, responsive self-reflection tools, and others. Furthermore, all figures in illustrations were depicted in a gender-neutral form and with varying ethnic characteristics to avoid bias in the perception of content by association with a social role model or stereotypes. The media-didactic optimization was conducted in order to make the LMS as user-friendly and easy to understand as possible, as well as to make the overall user experience engaging. It was also intended to ensure accessibility. All of these measures are supposed to increase the learning success of the participants and serve to strengthen adherence. Therefore, an experienced professor of applied digital product development, himself a media pedagogue and communication designer, and his team served as media-didactic experts. This provided many years of experience in interaction design, digital product development, and the development and optimization of content management systems, mass customizing platforms, and e-learning systems.
The provision of course exercises is partly adapted according to the answers in the baseline questionnaire. Depending on indications of special disease manifestations (e.g., chronic fatigue syndrome), some exercises are only offered in a limited version or with additional instructions. At the beginning, only the first-course module can be accessed. On the day of the respective webinars, the corresponding modules are unlocked for the participants.
The content of both the webinars and the self-study course is interdisciplinary and provides evidence-based information, recommendations, and exercises from medicine, psychology, physiotherapy, and nutritional sciences. If participants suffer from a particular medical condition that renders specific exercises to be recommended only in a limited or reduced version (i.e., physiotherapeutic exercises), the LMS content automatically adapts according to the given answers in the medical symptom screening. Participants are able to contact their coach via the integrated chat function, if they have any questions or require further advice. In addition, technical support is available by email.
Moderate intensity interventionThe same 12-week interactive self-study course is available as in the high-intensity arm with all features, except for the webinars. Again, only the first module is activated in the self-study course at the beginning. In this arm, however, participants can unlock the following modules independently by completing the previous one. They therefore determine the learning rhythm completely on their own. The participants are advised several times during the course that the modules have been designed in such a way that the optimum processing time for each module is about 1 week. Static information material is equally provided as in the high-intensity arm. Since participants are not assigned to a personal coach without the webinars, they direct their inquiries to a coach-supervisor via the chat function to ask for advice. Requests on psychological topics are answered by the psychological head investigator, while medical questions are answered by a physician of the study team.
The coach-supervisor also leads the quality assurance and supervision sessions in the high-intensity intervention. For specific questions, the coach-supervisor seeks the advice of a qualified specialist from the study team (physician, physiotherapist, etc.).
ControlOnly content that participants could have found without professional guidance should be available here. For ethical reasons, a quality check was carried out to ensure that all information provided is basically correct and does not conflict with the principles of evidence-based treatment. Participants therefore receive 12-week access to a reduced version of the self-study course containing only the static information materials. All interactive, responsive, or didactically optimized content is not offered. At the beginning, again only module 1 is unlocked and the activation of further modules is equivalent to the moderate intensity arm. The chat function, coach support, or other didactic interaction are not available to participants in this arm.
Criteria for discontinuing or modifying allocated interventionsNo changes to the assigned interventions are intended. However, all exercises shown in the program are voluntary and can be done or skipped by the participants individually. Thus, less intervention components deemed by the participant to be less beneficial can be excluded individually.
The attending GP may exclude participants from further participation at any time for medical reasons. The assessment of reasons (e.g., worsening disease) is the exclusive responsibility of the GP.
Participants themselves can terminate their participation at any time by revoking their consent.
Any of the following situations during the study period will also lead to discontinuation:
Strategies to improve adherence to interventionsFor monitoring adherence and participation indices, the LMS provides a dashboard that can only be accessed by the study management team. It allows real-time monitoring of participation numbers and group distributions.
Several measures have been taken to increase adherence.
Starter kitsAll participants receive a starter package as a gift upon joining the study. The package consists of branded carrier bags containing a ball pen, a keychain, and a notebook that participants can use to work on exercises during the program.
Reminder emailsParticipants receive a reminder email at defined events within the patient journey, in case of inactivity or if they miss a checkpoint in the process. Specifically:
In case of an incomplete registration process.
Appointment reminders on webinar days.
In case of inactivity (7 days without interaction in the LMS).
When there is a new system message or chat message in the LMS inbox.
In case of non-response to a mandatory questionnaire.
IncentivesAmong all participants who have completed 80% or more of the evaluation measures, €25 e-gift vouchers will be raffled (about 1 in 3 chances).
Feedback on health determinantsThere are various health trackers within the LMS platform that participants can use to monitor their progress throughout the program. In addition, after each completion of the short weekly symptom questionnaire, participants receive direct feedback as a graphical visualization of their scores on multiple determinants of health in comparison to the previous week. This feature is also available to the control group and exceeds what participants would find on other websites or on the Internet.
Relevant concomitant care permitted or prohibited during the trialAll concomitant treatments or interventions that match the exclusion criteria described in are prohibited during the trial. The same applies to interventions directly caused by any of the exclusion criteria, e.g., psychiatric therapy due to a current psychiatric illness. Other treatments are accordingly allowed.
Provisions for post-trial careFollow-up care after the trial is guaranteed as follows:
By involving the treating GP as the study physician, follow-up treatment is ensured via the usual care with full transparency about the interventions carried out.
A trial participant insurance policy was contracted for all participants.
Outcomes Primary outcomePrimary outcome is the cumulative sum of sick leave days in patients during the period from enrollment to 6-month follow-up. We compare the high-intensity intervention versus moderate-intensity intervention versus control group. In Germany, every employee requires a medical sick leave certificate. The medical sick leave certificate entitles to 6 weeks of continuous payment of the salary by the employer. Thereafter, for additional 180 days, the statutory health insurance provides 80% of the net salary. Law mandates that employers offer employees with sick leave of longer than 6-week duration the opportunity to participate in a structured employment reintegration program (BEM). In such programs, patients are attempted to be reintegrated into their former jobs in agreement with the occupational health physician, the employer, and the employees’ representative board. The usual process is to gradually increase the weekly job hours and job requirements expressed as a percentage of full employment. Therefore, if a patient takes part in such a program, the sum of days that the participant has spent within an integration percentage stage is used as the primary outcome instead (e.g., 10 working days at 50% equals 5 days on full sick leave). In both cases—sick leave days and reintegration days—the data is reported directly to the study management by treating GPs via their health care networks at once at the end of the trial.
Secondary outcomesSecondary outcomes are change in quality of life, work ability, work productivity, and symptom occurrence and severity. These will be collected via questionnaires using patient-reported outcome measures (PROMs, see below). Participants complete comprehensive surveys at enrolment (T0 questionnaire, approx. 20 minutes completion time, baseline values), after finishing the 12 modules of the intervention period (T2 questionnaire, approx. 10-min completion time, after 3 months) and as mid-term follow-up 6 months after enrolment (T3 questionnaire, approx. 10-min completion time). In addition, a short questionnaire is collected weekly (T1 questionnaire, details see below). T0, T2, and T3 assess the following dimensions of health: health-related quality of life (mental and physical), physical complaints, depression, anxiety, burnout, pain, social support, physical fitness, shortness of breath, sleep quality, and work ability. Current medication, vaccination status, concentration issues, and individual COVID-related medical history as possible influencing parameters are collected at T0. The T0 questionnaire also obtains indicator scores for disease courses or symptoms which require adjusted specific module components. The disease courses or symptoms considered are post-exertional malaise (PEM), myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), and orthostatic intolerance (OI). If required on the basis of the specific score of a participant, the LMS content is automatically adapted for high-intensity or moderate-intensity physical exercises within the intervention.
Once weekly during the intervention period, participants complete a short questionnaire (T1.1–T1.12) of 5-min completion time. This questionnaire offers short questions on current symptoms, well-being, and again work ability. As a direct feedback, participants receive a visualization in the form of a radar chart comparing their current values to the data of the previous week.
Furthermore, participants of the high-intensity and moderate-intensity groups have the possibility to report on how they are feeling in terms of energy level, overall health, pain, mood, number of enjoyable activities, and exercise level in visual analog scales via the LMS as often as they like during the intervention period. This tracker data is presented to the participants as a progress graph line chart.
The high rate of sick leave days in Long COVID patients could be directly related to the variety and severity of symptoms that patients experience [12, 29]. An improved ability to work could therefore be seen as an indicator for an improvement in the activities of daily life and the symptoms.
Further secondary outcomes are participation and dropout rates, including the exact dropout points during the process (directly derived from the user data of the LMS). Finally, we obtain meta-data on the use of resources, particularly the overall usage statistics of the LMS (e.g., which pages and multimedia content were accessed and how often, which bookmarks were set, which exercises were completed repeatedly and how often, how many reminder mails had to be sent and when).
At the end of the trial, all the secondary outcomes data described is exported at once by the provider of the LMS and sent to the study data management after appropriate pseudonymization.
Possible side effects are also recorded as secondary outcomes. These are reported directly and anonymously by the respective treating GP to the study management team. These reports include the methods used for diagnosis of side effects.
Participant timelineThe participant timeline is shown in Fig. 2. An alternative depiction following the SPIRIT schedule recommendation is shown in Fig. 3.
Fig. 2
Patient journey and intervention assessment timeline; LMS, learning management system; GP, general practitioner
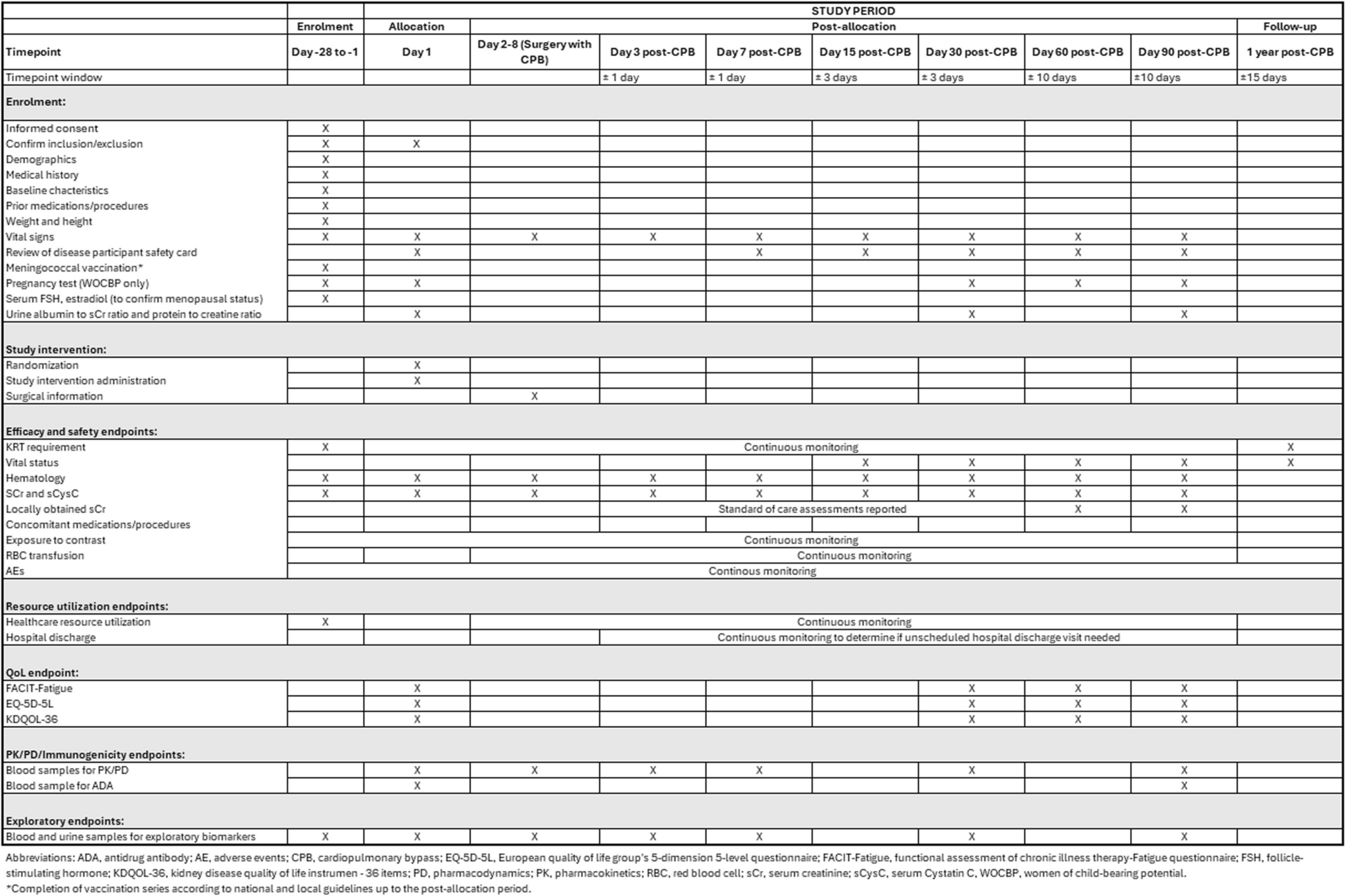
Fig. 3
Schedule of enrolment, interventions, and assessments following the SPIRIT guidelines
Sample sizeThe sample size was calculated for a randomized single-factor ANOVA design with 3 groups without clustering, assuming 30 days of illness (standard deviation of 10 days) during 180 days of follow-up in the control group and a reduction by 4 days for the high-intensity intervention (effect size of Cohen’s d = 0.4) and a reduction by 1 day in the medium intensity group. Such reduction was deemed by occupational health physicians as well as general practitioners as clinically highly relevant. Compared to the control group, a power of 80%, a type 1 error probability of less than 5%, and a dropout rate of 25% result in a required sample size or N = 151 per group. Thus, we aim to include at least N = 453 patients. In order to be able to exclude possible correlations due to socio-demographic variables corresponding to the location of participating practices (in particular rural doctors versus urban infrastructure), the target size is an increased sample size of 600 patients in total (N = 200 patients per study arm).
RecruitmentPatients will be recruited by health care networks and their affiliated general practitioners (GP) through various means, including (1) face-to-face invitations; (2) phone invitations; (3) promotional materials such as posters, leaflets, and brochures; (4) press releases and newspaper articles; (5) promotion through project website; and (6) promotion through social media. In addition, patients can be recruited by occupational physicians of different companies which will allow us to recruit a heterogeneous group covering a broad spectrum of professions.
Assignment of interventions: allocationSequence generationBlocked stratified randomization will be used to assign participants to the randomization groups. Strata have been defined by age, gender, type of employment (brain worker/physical worker), and status of disease (acute or Long COVID). Randomization sequence has been generated by the statistical software package STATA, function STRATA rand (StataCorp. 2019. Stata Statistical Software: Release 16. College Station, TX: StataCorp LLC).
Concealment mechanismThe allocation table is stored in the LMS and is queried by an automated script during the registration process. The stratification variables are known, because they are collected via the T0 questionnaire which takes place before the randomization process. In concrete terms, this means that after participants have registered in the LMS with their code, they complete the T0 questionnaire and are then automatically assigned to an intervention group. Thus, additional measures to establish the allocation sequence are not necessary, as no active action is required due to the automatism. Likewise, no measures to conceal the sequence are necessary due to the automation.
ImplementationThe computer-generated allocation sequence was transformed into a randomization reference table for each stratum stored in spreadsheet calculation software. Patients register themselves in the LMS. Patients are then sequentially selected for randomization and classified to strata based on the stratification variables. The allocation number is read sequentially from the reference table for the respective stratum.
Assignment of interventions: blindingWho will be blindedParticipants themselves are blinded. They only receive the information that they have been assigned to an intervention group called “A,” “B,” or “C.” The participants do not know which measures are possible. They also do not know which intervention portfolio is associated with which letter. GPs are blinded in the way that they are not told which group a patient has been allocated to.
The study management and data analysts themselves are generally not blinded. However, they do not have direct access to participant data and participants during the trial period, and the evaluation is done on aggregated data once the study is completed.
Procedure for unblinding if neededA process for unblinding is not envisaged, as no incidental diagnoses or other realistic events requiring immediate action by the participant are conceivable in the given conception. Nor would legal demands be likely to make this necessary.
Data collection and managementPlans for assessment and collection of outcomes Primary outcomeGPs document sick leave days and BEM days in patient records as part of their normal work outside the study. At the end of the trial, the GP totals these days per study participant she enrolled for a period of 6 months counting from the day of registration in the LMS. This registration is defined as the start of the intervention. The GP then writes the accumulated days into a pseudonymized list of her patients and transmits this file to the study center via an end-to-end encrypted virtual data safe access. This simple procedure reduces the workload for GPs and eliminates the need for special instruction.
Secondary outcomesAll questionnaires conducted in the trial are collected via integrated html-based forms within the LMS. All data collected via the LMS is stored in the related sql database.
Various dimensions of health are assessed via the PROM-based T0 to T3 questionnaires:
Health-related quality of life (mental and physical) is measured via short-form 12 (SF-12). The questionnaire consists of 12 items on general health perception (1 item), physical health (2 items), limited physical role function (2 items), physical pain (1 item), vitality (1 item), mental health (2 items), limited emotional role function (2 items), and social functioning (1 item).
The royalty-free version 1 of the questionnaire was used. By weighting and dependent calculation of the individual values, two scores on physical and mental health-related quality of life are generated according to a complex formula. In this trial, the values are not weighted with the orthogonal factor loadings suggested by the test authors, but with oblique factor loadings. It has been shown that this leads to more consistent results, since the calculation includes an interdependence of physical and mental quality of life [30]. Except for these adjustments, the SPSS rule is used for scoring as suggested in the test manual. The SF-12 is part of the T0, T2, and T3 questionnaires.
Screening for depression is carried out by a 9-item PHQ-9 subgroup of the patient health questionnaire family. This subgroup constitutes the depression module and can be used as an independent score to screen for depression. It measures common depression symptoms over a 2-week reference period via 4-point Likert scale with response categories ranging from “Not at all” to “Nearly every day”. Between 0 and 3 points are given for each answer and added up unweighted. The resulting sum score thus ranges from 0 to 27, with higher scores indicating more severe depression symptoms. The PHQ-9 shows good psychometric properties as a screening for depression when using the summed-item method [31, 32]. The PHQ-9 is part of the T0, T2, and T3 questionnaires.
Physical complaints are surveyed via the patient health questionnaire 15 (PHQ-15). The questionnaire consists of 15 items on the severity of the most common somatic symptoms. Each item has the 3 response categories “Not bothered at all” to “Bothered a little” to “Bothered a lot” asking about the symptom burden within the last 4 weeks. One of the mentioned symptoms refers to menstrual problems, so this is automatically not presented to male participants. Non-binary participants are presented with the item. In this trial, the PHQ-15 is not evaluated as a score, but as a distribution of symptom frequencies and symptom severity for each symptom recorded. Two of the items (concerning sleep problems and lack of energy) are also part of the PHQ-9. To calculate its score correctly, these two items are asked for a 2-week reference period like in the PHQ-9 instead of a 4-week reference period. The PHQ-15 is part of the T0, T2, and T3 questionnaires.
Anxiety is measured via the generalized anxiety disorder questionnaire (GAD-7). The questionnaire consists of 7 items on anxiety symptoms over a 2-week reference period via 4-point Likert scale with response categories ranging from “Not at all” to “Nearly every day”. Between 0 and 3 points are given for each answer and added up unweighted. The resulting sum score thus ranges from 0 to 21, with higher scores indicating higher anxiety. The GAD-7 as a self-report instrument for generalized anxiety disorder has good reliability and construct validity with an optimized sensitivity of 89% and specificity of 82% [33]. There is a high correlation between severity in the GAD-7 and disability scores [34]. The GAD-7 is part of the T0, T2, and T3 questionnaires.
Burnout (personal, work-related) is measured via Copenhagen Burnout Inventory (CBI). It divides the symptomatology into personal, work-related, and client-related burnout. Each scale can be calculated independently. All 3 scales show good reliability levels [35]. The questionnaire is administered to check the successful differential diagnosis between burnout and Long COVID. In addition, a possible deviating effect of the MiLoCoDaS intervention plan on varying burnout scores might be discovered. Since the client-related burnout does not essentially affect the research question, this subscale was not included in the survey for reasons of test economy. The chosen subscales consist of 13 items on burnout symptoms using 5-point Likert scales with response categories ranging from “Never / very rarely” to “Always” or from “To a very low degree” to “To a very high degree” respectively. Between 0 and 4 points are given for each answer and added up unweighted. In the resulting sum score, higher values are indicating higher burnout probability. The CBI is part of the T0, T2, and T3 questionnaires.
Pain is measured via an adaptation of the Cornell Musculoskeletal Discomfort Questionnaire (CMDQ). In this trial, the CMDQ is not evaluated as a score, but as a distribution of pain locations, frequency, and severity among Long COVID patients. In the first step, the particular pain localization is asked using a suggestion list. Then, the participants rate the pain intensity per previously named region on a numerical analog scale of 1–10, with higher values representing more pain. At last, participants rate the impairment of their usual activities by the reported pain. The German version of the CMDQ shows good psychometric properties [36]. The CMDQ is part of the T0, T2, and T3 questionnaires.
Social support is measured via the ENRICHD-Social-Support-Instrument (ESSI), the social support subscale from the Enhancing Recovery in Coronary Heart Disease study (ENRICHD) questionnaire. The questionnaire consists of 5 items on individual availability of social support using a 5-point Likert scale with response categories ranging from “None of the time” to “All of the time”. Between 1 and 5 points are given for each answer. Items are then added up for an unweighted sum score, with higher values indicating greater social support. The ESSI shows good psychometric properties including the German adaptation [37, 38]. The ESSI is part of the T0, T2, and T3 questionnaires.
Physical fitness is measured via the 12-item short form of the questionnaire for the assessment of physical function status (FFB-MOT). The questionnaire consists of 12 items on physical activities related to everyday life using a 5-point Likert scale with response categories ranging from “I cannot do this activity” to “I do not have any problems.” Between 1 and 5 points are given for each answer. Items are then added up for an unweighted sum score, with higher values indicating better physical fitness. The FFB-MOT shows good psychometric properties for general populations [39]. The FFB-MOT is part of the T0, T2, and T3 questionnaires.
Sleep quality is measured via 5 mixed items on overall assessment of sleep quality, daytime sleepiness, problems falling asleep and staying asleep, and restfulness of sleep. Response categories use 5-point and 6-point Likert scales on quality (overall assessment) and frequency (other terms). Items on sleep problems and restfulness are inverted, so that higher values indicate better sleep. Afterwards, the items’ values are harmonized to a range of 0–100 to equalize the different response scales. Then, an unweighted mean is calculated. A root-based transformation is performed to compensate for ceiling effects and finally standardized to a mean of 66 and standard deviation (SD) of 15. Questions on sleep quality are part of the T0, T2, and T3 questionnaires.
Work ability is measured by an abbreviated assessment based on the Work Ability Index (WAI). The original version consists of 7 indicators on (WAI 1) Current work ability compared with the lifetime best, (WAI 2) Work ability in relation to the demands of the job, (WAI 3) Number of current diseases diagnosed by a physician, (WAI 4) Estimated work impairment due to diseases, (WAI 5) Sick leave during the past year (12 months), (WAI 6) Own prognosis of work ability 2 years from now, and (WAI 7) Mental resource [40, 41]. The trial-adapted version consists of 5 items relating to WAI 1, 2, and 4. WAI 4 topic was split into two items that record productivity losses and work quality separately. Items referring to WAI 1 and 4 use a numerical analog scale from 1 to 10; items related to WAI 2 use a 5-point Likert scale with response categories ranging from “poor” to “excellent”. In this trial, the adapted WAI indicators are not evaluated as a score, but as single-item distributions. The described questions on work ability are part of all questionnaires T0 to T3 administered throughout the trial.
Well-being is measured via the World Health Organization’s 5-item questionnaire on well-being (WHO-5). The concept of the WHO-5 is based on the Major Depression Inventory, which maps the WHO/ICD-10 criteria for depression. The questionnaire consists of 5 items on general psychological well-being aspects over a 2-week reference period via 6-point Likert scale with response categories ranging from “At no time” to “All of the time”. Between 0 and 5 points are given for each answer. The individual values are added up and multiplied by 4, resulting in a score range of 0–100. Higher values indicate higher well-being. The WHO-5 shows good psychometric properties [42,43,44]. The WHO-5 also showed a strong negative association with depression symptoms, especially in the range of mild to moderate symptom severity, and is therefore suitable for screening [45]. The WHO-5 is only used in T1 questionnaire.
Shortness of breath is measured via 3 specific items using a numerical analog scale from 1 to 10 with pre-COVID-19 and post-COVID-19 values resulting in a total of 6 values. They assess shortness of breath at rest, during light physical activity, and during heavy physical activity. Scores will not be calculated from this. Questions on the shortness of breath are part of the T0, T2, and T3 questionnaires.
Medication, vaccination status, concentration issues, and COVID-related medical history are surveyed as single items in order to enable fine-grained subgroup analyses and adjustment for influencing variables. Items on medical history use a numerical analog scale from 1 to 10 with pre-COVID-19 and post-COVID-19 values, if specific symptoms are asked. Scores will not be calculated from this. They are only asked in the T0 baseline questionnaire.
Health trackersParticipants from the high-intensity intervention and moderate-intensity intervention groups have health trackers in the form of sliders as a visual analog scale on their overview pages in the LMS. These are labeled as “energy level,” “overall health,” “pain,” “mood,” “amount of enjoyable activities,” and “exercise level” and can be set and saved as often as desired. This offers the possibility of chronological documentation, which allows conclusions to be drawn about the variance of the values referring to the mentioned domains in relation to the individual progress within the therapy program.
User statisticsBy registering on the LMS, participants agree to their user activity being recorded. The corresponding data is also stored in the participant’s respective data record.
Generating data setsAt the end of the trial, all raw values regarding the abovementioned secondary outcome data acquired via the LMS are exported by the platform provider as a data set in .json format (JavaScript Object Notation) and sent to the study management team for evaluation using the end-to-end encrypted virtual data safe. These data sets are pseudonymized without exception. They do not contain any unencrypted personal data.
Plans to promote participant retention and complete follow-upParticipant retention plans are consistent with the strategies to improve adherence to interventions described in . Full follow-up is usually ensured by adherence to the GP, unless patients generally change their GP. As many of the planned outcomes as possible are collected for all participants, including those who drop out.
Data managementThe MiLoCoDaS study has a comprehensive data protection conception, including a data protection impact assessment, technical and organizational measures, records of processing activities, and data processing agreements with involved service providers. Data quality assurance has been sufficiently implemented as a requirement of the data protection laws by numerous measures that can be found in the respective documents.
Confidentiality General data protection regulationsThroughout the entire project, the data protection regulations according to the GDPR are strictly adhered to and controlled. An accompanying assessment by the responsible department for data protection has been carried out for all relevant aspects. For concrete details on individual measures, please refer to the comprehensive respective documents.
Nevertheless, special reference is made to the constant pseudonymization of patient data at all trial steps.
Enrolment and accompanying careAll measures carried out by the GP are subject to medical confidentiality and the data protection standards according to which medical practices are obliged to work. GP keep the pseudonymization key in the patient record, as they are the only party usually holding unencrypted patient data.
LMSIdentifying data and health data are stored in different data sets in the LMS database. All health data is stored in pseudonymized form only. Only top-level system administrators of the LMS service provider have direct access to the database. No one else has direct access during or after the study period. However, direct database access during the project period is usually not required. Data exports for analysis exclusively occur in pseudonymized form. The data will be completely anonymized as soon as the purpose and progress of the research permits.
Data transferAny data transfer between stakeholders that includes the health data of participants will only be conducted in pseudonymized form. When data sets or outcome information is sent, this is done exclusively via end-to-end encrypted password-protected virtual data safe access.
Plans for collection, laboratory evaluation, and storage of biological specimens for genetic or molecular analysis in this trial/future useNot applicable, as no biological samples are collected in the MiLoCoDaS study.
Statistical methodsStatistical methods for primary and secondary outcomesGeneralized linear models will be used to compare the distribution of primary outcomes (sick leave days) in the randomization groups. Link function will be determined based on the observed sample distribution (we expect Poisson or Negative Binomial distribution). Secondary outcomes will be analyzed by Repeated Measurements Analysis of Variance and Mixed Models for Change analysis. Longitudinal response curves will be visualized by graphs showing the marginal estimates in the randomization groups. All statistical analysis will be conducted using the software package STATA (StataCorp. 2019. Stata Statistical Software: Release 16. College Station, TX: StataCorp LLC).
Interim analysesInterim analyses will only take place in the form of the regular monitoring of participation numbers by the study management team and will not constitute a study termination.
The only defined criterion for study termination is data protection incidents (especially if there is a risk of recurrence or expansion). The final decision on study termination is then made by the primary sponsor.
Methods for additional analyses (e.g., subgroup analyses)Subgroup analyses will be conducted repeating the efficacy analyses in subgroups of the study population defined by patient-specific variables. Subgroup analyses focus on elucidating observed heterogeneity of effect sizes rather than testing for statistical significance, as the sample size of the study has been defined to achieve sufficient power for the main analysis. Subgroup analyses have only exploratory objectives and nature; therefore, we refrain from adjustment for multiple comparisons. Rather than reporting statistical inference test results, we will report observed effect sizes and related confidence intervals without adjustment for multiple testing.
Methods in analysis to handle protocol non-adherence and any statistical methods to handle missing dataStatistical analysis will be conducted using complete case analysis and as a sensitivity analysis using imputed data based on a multiple imputation algorithm. If the distribution of the observed missing pattern is at random, the core model will be based on the imputed data.
Plans to give access to the full protocol, participant-level data, and statistical codeUnlimited public access is not planned. Following the guidelines of the administering study register, there exists an IPD (Individual Participant Data) Sharing plan for the exchange of participant data. According to its provisions, only aggregated, anonymized data and aggregated questionnaire scale values will be shared. Eligible recipients are researchers who submit a methodologically sound proposal. This applies equally to the dissemination of complete protocols or statistical code. Requests should be directed to the principal investigator via email.
Oversight and monitoringComposition of the coordinating center and trial steering committeeThe study center is responsible for study coordination. It works closely with the project partners. The responsibilities are distributed as follows:
Primary Sponsor (Joachim Fischer)The Primary Sponsor (PS) is responsible for the coordination and supervision of the team. He also has the final decision on content and conceptual matters.
Principal Investigator (Adrian Krotz)The Principal Investigator (PI) provides oversight for all aspects of the study and the implementation of the intervention.
Scrum Master (Stephanie Bechtel)A Scrum Master is established and responsible for project management. She supports the team to achieve the project’s goals by following the Scrum framework.
Conception team (Nadia Sosnowsky-Waschek / Joachim Fischer and coworkers)Together with the project partners from psychology and physiotherapy, the Primary Sponsor forms the conception team, which is largely responsible for the development of the interventions' content. This team is supported by a group of at least 10 students from these disciplines.
Study management teamPrincipal Investigator, Scrum Master, and other intermittently involved scientific staff form the study management team. The study management team contributes to the development of content in interventions as well as the design and technical implementation of the LMS. It is responsible for the collaboration with healthcare networks and provides ongoing support. In cooperation with the study statistician, it is also responsible for data analysis. The study management team meets on a weekly basis to oversee the study progress and to ensure the integrity of the protocol and conduct of the study.
Composition of the data monitoring committee, its role, and reporting structureThe implementation of a data monitoring committee is not planned for this study. Because of data aggregation, all data will only be obtained in summary form at the end of the study. Only the monitoring of patient allocations is carried out on a regular basis via the LMS study management dashboard.
Adverse event reporting and harmsAll participants are instructed to report adverse events and harms or side effects at any time to their GP as the first instance. Such events can in addition be reported directly to all other stakeholders in the project. The reporting chain and the cooperation in such cases are defined in the respective contracts.
Frequency and plans for auditing trial conductThere is no audit plan for this study. In particular, since a data analysis only takes place at the end and no adjustments are planned in the meantime, an interim audit is not necessary.
Plans for communicating important protocol amendments to relevant parties (e.g., trial participants, ethical committees)If significant changes to the protocol occur, relevant parties are informed as follows:
Participants: Participants receive a system message providing all necessary information via the integrated message function of the LMS. In addition, an email notification is sent about the receipt of the system message.
Project stakeholders: If they are affected by the changes, LMS service providers and healthcare networks are notified directly by the study management team via email or phone. GPs receive the information through their affiliated networks.
Registries, journals, and other external recipients: The study management team determines the necessary scope of change information at its weekly meeting and initiates appropriate notification.
Dissemination plansIt is planned to publish all trial results as journal articles. Results are additionally to be summarized in brief form on the study center’s website. All participating GPs and healthcare networks will be sent references to results as soon as they are published. For the information of participants, a highly abbreviated layperson’s summary of the results will also be issued to the GPs. Participants can ask their GP about the status of the results at any time.
Comments (0)