
Remember me





Physical fitness is the set of attributes allowing persons to perform daily activities and meet unforeseen emergencies (1). Robust data support physical fitness as an independent predictor of waiting list survival in liver transplant (LT) candidates and, in fact, physical fitness performs as strongly as the model for end-stage liver disease for prognostication (2–5). Despite tremendous progress in understanding the role physical fitness plays in LT, interventional strategies aiming to reverse frailty or improve cardiopulmonary endurance have notably lagged (6). Although emerging evidence supports the value of LT prehabilitation (7), it is still not recognized as a preparatory stage for waitlisted individuals. This relates to exercise clinical trials in cirrhosis being heterogeneous and to limited evidence in advanced chronic liver disease (AdvCLD) (8). Despite some evidence for improved sarcopenia and frailty metrics after an exercise intervention in AdvCLD (7,9–11), there remains contradiction as to whether the Liver Frailty Index (LFI) and 6-minute walk test (6MWT) can meaningfully improve in LT candidates.
We recently developed Exercise and Liver FITness (EL-FIT), a smartphone application that helps prescribe and deliver a standardized exercise intervention for patients with AdvCLD. EL-FIT provides physical literacy and exercise videos, and when linked to a personal activity tracker (PAT), incorporates walking into the training maneuver. As part of its field-testing strategy, we showed that 35% of participants were able to increase their physical activity during a 5-week period (12). Because personalized exercise coaching leads to improved intervention uptake and maintenance (13), we hypothesized that adding coaching to the EL-FIT home-based exercise program would improve fitness and training adherence. As such, the primary aim of the present pilot and feasibility trial was to quantify the improvement in LFI and 6MWT after completion of a home-based prehabilitation program. Secondarily, we wanted to determine the feasibility of and adherence to the prehabilitation program. With the intention of further developing the field of mobile-assisted telehealth regimens to increase exercise (MATRIX), a third aim investigated in-training PAT data and EL-FIT usability to serve as feedback for designing future interventions.
METHODSPatients with cirrhosis and AdvCLD undergoing LT evaluation, ages 40–70 years, with a model for end-stage liver disease–sodium ≥10 and clinical evidence of portal hypertension were invited to participate. After a baseline evaluation and consent, each participant was given a PAT (Fitbit Charge 3; San Francisco, CA) and had both EL-FIT and Fitbit apps downloaded and installed to their smartphone. After a brief educational session on how to use the apps and the PAT by a member of the research team, patients were asked to continuously wear their PAT until the end of study and to explore all features of the EL-FIT app. Refer to the Supplementary Digital Content (see Supplementary Material, https://links.lww.com/CTG/A984) for further details.
Physical fitness evaluationAll patients underwent a comprehensive physical fitness evaluation by the LT physical therapist (LT-PT; P.M.B.), including assessment of LFI, 6MWT, and gait speed test (GST), both at baseline and by the end of study. Using these 3 metrics, patients were considered frail if LFI ≥4.4, 6MWT <250 m, or GST <0.88 m/s (2,4,14). LFI further subclassified nonfrail patients into robust when the score was ≤3.2 or prefrail when the score was 3.21–4.39 (15).
EL-FIT intervention and coaching sessionsAfter a 2-week run-in period, subjects were contacted by a physical activity coach to start the intervention. The EL-FIT home-based prehabilitation program consisted of a 12-week exercise regimen combining aerobic and resistance training of very light to moderate intensity. At baseline and on a weekly basis until completion of study, participants had 15- to 30-minute phone calls with a physical activity coach trained in behavioral counseling and motivational interviewing, a strategy we have found to yield positive results in previous trials (16). Each session finalized with new training goals focusing on exercise video(s) the participants needed to execute successfully (with individualized number of repetitions), along with walking at an increment pace of 500 steps/d in average, weekly to biweekly. Whenever the coaches identified a technology or connectivity issue (e.g., PAT not synchronizing), they would inform the research coordinator to have the issue fixed. Any medical concern (e.g., lower-extremity edema) was informed to the hepatologist (A.D.R.) for proper action (e.g., diuretics adjustment) and discussed at a weekly meeting coordinated by the senior exercise physiologist (J.M.J.), where all safety concerns were reviewed.
Statistical analysisResults were summarized as proportions for categorical variables, mean ± SD for normally distributed continuous data, or median (25th–75th percentiles) for nonnormally distributed continuous data. Comparisons were performed with χ2, McNemar, Mann-Whitney, or paired t test depending on type and distribution of data. Regarding the analysis of data from PAT, we grouped the output by weeks, averaging the daily step count. Participants were subclassified as being able to accomplish ≥1,200 steps/d or not; patients walking <1,200 steps/d have an increased risk for hospital admission and mortality (17).
The feasibility end point was defined as two-thirds or more participants completing the run-in period and engaging in the intervention phase. Given the dual nature of the intervention, adherence considered video interaction as a minimum of 2 training sessions per week or walking performance as a baseline increase of 500 or more average daily steps over two-thirds of the intervention weeks. The 500 steps/d delta was selected because such a change had been associated with decreased hospital admission and improved survival in AdvCLD per our previous study (17). Participants fulfilling criteria for at least 1 of the 2 training strategies (i.e., video or walking) were considered adherent, and we expected to see over 50% adherence. We followed per-protocol analysis for the primary outcome, a modified intention-to-treat analysis for adherence, where only participants moving into the intervention phase were accounted for, and an intention-to-treat analysis for feasibility. The reason for choosing a per-protocol analysis for the primary aim responded to the pilot nature of study. Statistical analyses were performed using Stata v16 (StataCorp, College Station, TX).
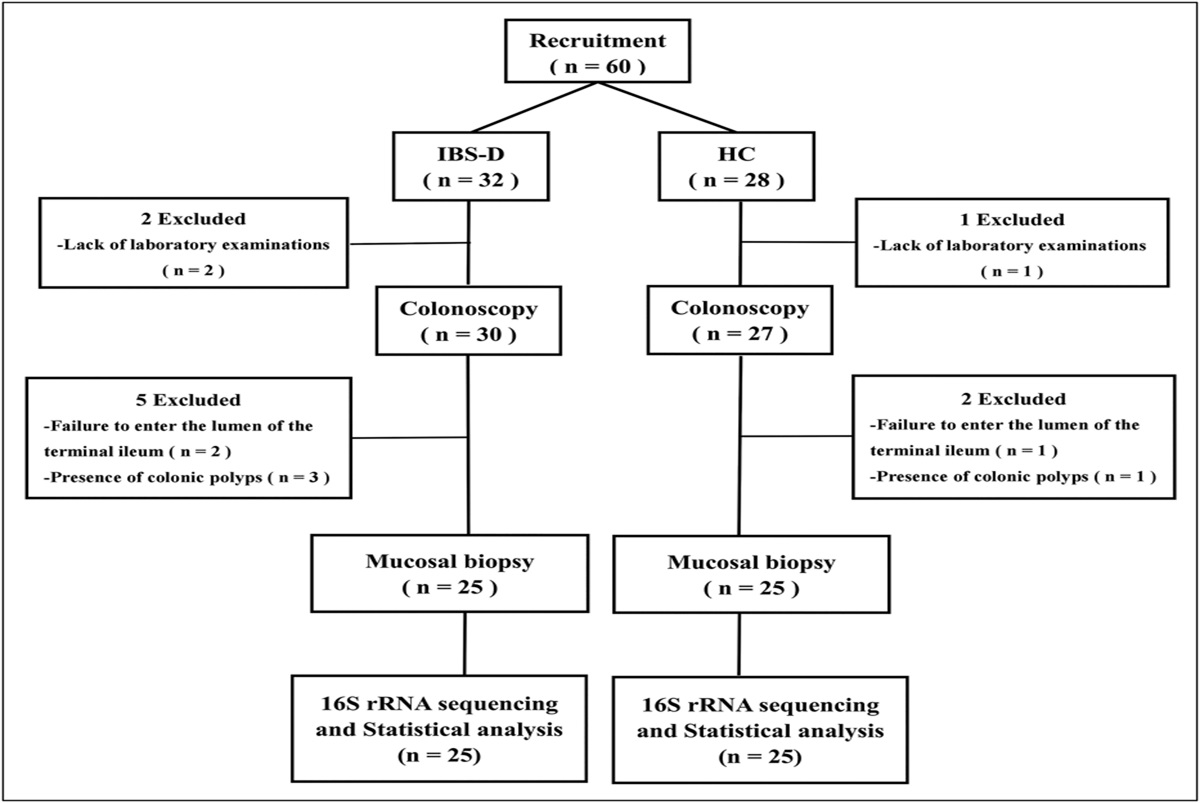
RESULTS Cohort descriptionA total of 31 patients fulfilled inclusion criteria and consented for study. All of them were provided with a PAT and EL-FIT. Ten participants did not complete the run-in phase and thus did not proceed to the intervention phase (Figure 1). Eight participants left the clinic before completing the onboarding process and 3 could never be contacted by the physical activity coaches (Table 1). Regarding the EL-FIT training intensity allocation, we could compare it with our LT-PT prescription in 28 participants, finding agreement in 17 (61%; P = 0.07). Except for 1 case, where EL-FIT assigned moderate-intensity training and LT-PT prescribed the lowest intensity of training, in all other disagreements EL-FIT provided a less intense prescription than LT-PT, thus favoring safety. Refer to the Supplementary Digital Content (see Supplementary Material, https://links.lww.com/CTG/A984) for further details.
 Figure 1.:
Figure 1.: Recruitment flowchart.
Table 1. - Degree of engagement among patients not completing the run-in period Participant Completed onboarding LFI|6MWT|GST Steps tracking Average daily step count Total videos watched Educational videos watched Training videos watched Initial session with coach 5 No 3.6|N/A|N/A PAT not linked N/A 0 0 0 N/A 6 No 2.4|366|1.0 PAT not linked N/A 4 4 0 N/A 8 No 5.1|192|0.6 PAT not linked N/A 0 0 0 N/A 9 No 4.4|276|1.0 PAT not linked N/A 23 3 20b N/A 10 No 3.9|252|0.9 PAT not linked N/A 11 10 1c N/A 11 No 3.1|322|1.0 PAT not linked N/A 22 5 17d N/A 12 No 3.5|327|1.0 PAT not linked N/A 44 4 40e N/A 13 Yes 4.1|409|1.3 5 d 1,789 0 0 0 No 16 No N/A|N/A|N/A 1 d 348a 0 0 0 No 20 Yes 2.2|468|1.1 3 d 5,277 12 8 4 No6MWT, 6-minute walk test; GST, gait speed test; LFI, Liver Frailty Index; PAT, personal activity tracker.
aPeriod collected corresponded to <24 hours.
bWatched first 4 strength and mobility videos.
cWatched the first strength and mobility video.
dWatched all strength and mobility videos and low intensity; first 3 moderate intensity and the balance video.
eWatched all 22 exercise available videos.
Baseline characteristics of patients moving on to the intervention phase are shown in Table 2. Importantly, people engaging with the intervention were predominantly women, almost half of them had obesity, had alcohol-related liver disease or nonalcoholic steatohepatitis, and were listed for LT. Regarding their liver disease status, all patients had minimal hepatic encephalopathy (HE) and the presence of decompensation was universal, including a large proportion with esophagogastric varices or overt HE. Approximately, one-third of patients were frail based on any of the 3 metrics assessed; based on LFI, 10 (47%) were prefrail and 5 (24%) robust. When considering frailty by either LFI or 6MWT, 8 subjects performed as frail and in 4, there was agreement between the 2 metrics. There were no differences in baseline characteristics between participants who left the study and those engaged with the intervention.
Table 2. - Baseline characteristics of cohort engaged in intervention Variable Descriptor (n = 21) Age (yr) 60 ± 7 Sex (females) 15 (71%) BMI (kg/m2) 31 ± 8 Obesity 9 (43%) Etiology Alcohol 7 (33%) NASH 6 (29%) Cryptogenic 6 (29%) Hepatitis C 1 (5%) Other 1 (5%) Waitlisted for LT 13 (62%) Education (yr) 12 (12–18) Falls (previous 6 mo) 6 (29%) Minimal HE 16 (100%)a Stroop on + off 249 ± 111 Stroop off 109 ± 38 Overt HE 16 (76%) Esophagogastric varices 16 (76%) Previous variceal bleeding 6 (29%) Refractory ascites 14 (67%) Hydrothorax 4 (19%) Hepatopulmonary syndrome 2 (10%) Type 2 diabetes mellitus 2 (10%) Chronic kidney disease 1 (5%) Heart disease 2 (10%) Hemoglobin (g/dL) 10.5 ± 1.9 Total bilirubin (mg/dL) 2.2 ± 1.9 Albumin (mg/dL) 3.2 ± 0.5 INR 1.5 ± 0.3 Creatinine (mg/dL) 1.1 ± 0.6 Sodium (mEq/L) 135 ± 5 Child-Turcotte-Pugh 10 (8–10) Class A|B|D 0|11|10 MELDNa 17 ± 5 LFI 4.1 ± 0.8 Frail by LFI 6 (29%) 6MWT (m) 270 ± 118 Frail by 6MWT 6 (29%) GST (m/s) 0.9 ± 0.4 Frail by GST 8 (38%)BMI, body mass index; GST, gait speed test; HE, hepatic encephalopathy; LFI, Liver Frailty Index; LT, liver transplantation; MELDNa, model for end-stage liver disease–sodium; NASH, nonalcoholic steatohepatitis; PAT, personal activity tracker; 6MWT, 6-minute walk test.
aFour patients could not perform Stroop EncephalApp and data were lost in 1.
Figure 2 shows the changes in our primary outcomes in the 15 participants who completed the study. LFI and 6MWT significantly improved by 0.4 and 41 m, respectively (see Supplementary Figure, https://links.lww.com/CTG/A983 for plotting of individual data). GST did not change from baseline to end-of-study assessment (0.97 ± 0.08 vs 0.99 ± 0.07; P = 0.77). Six participants did not reach the end of study visit due to death (n = 4), need for urgent surgery (n = 1), or being called for LT (n = 1) (Table 3). There was 1 adverse event that was related to the intervention: 1 participant experienced a fall while walking on an uneven surface (body mass index 53 kg/m2). Importantly, 12 participants (57%) were admitted to the hospital during the intervention phase in relation to complications from advanced liver disease and portal hypertension. Frailty by either LFI or 6MWT was reversed in 1 of 3 patients (33%) who were able to complete the study; however, no patient developed progressive frailty.
 Figure 2.:
Figure 2.: Physical fitness metrics before and after the prehabilitation intervention. (a) Improvement in frailty per the Liver Frailty Index. (b) Improvement in cardiopulmonary endurance per the 6-minute walk test.
Table 3. - Physical accomplishments in relation to training Participant's age|MELDNa|LFI Attrition wk Reason for attrition Safety concerns Hospital admissions Baseline step count Max step count (% increment) EOS step count (% increment) % wk at target 70|9|3.74 — — — No 2,257 4,073 (80) 2,317 (3) 75 46|20|3.04 — — Fall (related) Yes 969 1,413 (46) 962 (−1) 0 63|20|5.22 Week 4 Death (unrelated) None Yes 46 938 (1,939) — 20 57|17|2.92 — — — Yes 2,413 4,834 (100) — 46 65|16|5.24 Week 5 Transplanted — Yes 2 605 (30,150) — 20 71|12|4.31 — — — No 723 1,487 (106) 130 (−82) 11 66|12|3.08 — — Fracture (unrelated) Yes 1,185 3,982 (236) — 100 62|26|4.12 — — — Yes 387 10,283 (2,557) 673 (74) 92 53|17|3.95 — — — Yes 995 1,416 (42) 789 (−21) 0 51|15|3.06 — — — No 7,560 11,730 (55) 7,208 (−5) 67 62|12|4.39 — — — Yes 1,338 1,697 (27) 710 (−47) 0 51|16|5.30 Week 5 Death Unknown No 159 —a —a —a 63|17|4.51 — — — Yes 3,055 3,427 (12) 3,230 (6) 0 60|11|3.66 — — Vertigo (unrelated) No 4,717 12,570 (167) 2,853 (−40) 54 65|17|5.03 Week 11 Death (unrelated) None Yes (Hospice) 1,083 2,728 (152) 280 (−74) 70 64|14|5.44 — — — No 379 491 (30) — 0 61|10|2.93 — — — No 3,160 8,365 (165) 6,445 (104) 100 56|24|3.79 Week 1 Urgent surgery None Yes 823 — — — 56|15|4.13 Week 1 Death (unrelated) None Yes 356 — — — 57|27|4.04 — — — No 2,906 3,588 (24) 955 (−67) 11 51|23|3.65 — — — No 3,295 5,168 (57) 4,730 (44) 45EL-FIT, Exercise and Liver FITness; EOS, end-of-study; LFI, Liver Frailty Index; MELDNa, model for end-stage liver disease–sodium; PAT, personal activity tracker.
aPatient stopped synchronizing PAT to EL-FIT after week 1.
For feasibility, our study met its end point by showing that 21 (68%) of consented patients engaged in the prehabilitation program for a median duration of 11 (7–12) weeks. Furthermore, of the 21 subjects who continued to the intervention phase, 18 (86%) watched the literacy videos and 16 (76%) interacted with the exercise videos afterward. Of the 5 participants who did not use the EL-FIT training videos, 3 chose walking as their only form of training and showed engagement with such activity (see below). Regarding the interaction with EL-FIT exercise training videos, participants watched a median of 22 (7–43) videos (includes repeat videos), 8 (4–12) educational videos, and 18 (1–34) exercise training videos. The average interaction of training videos per week was 2 (0–4), and 11 of 21 participants (52%) showed adherence with the video exercising program by interacting with at least 2 videos per week, meeting the a priori definition. The reported emoji-based rate of perceived exertion after completion of each training video is shown in Table 4 for all participants. As shown, more than half of the video-training interactions were below the targeted training intensity (i.e., at least moderate). Participants showing video adherence reported their rate of perceived exertion more frequently (22 [13–26] vs 1 [0–10]; P < 0.001), although their perceived exertion was not more intense (2 [1–3] vs 0 [2–3]; P = 0.63).
Table 4. - Emoji-based Borg 15-point rating of perceived exertion scale after exercising with a video Score Meaning Frequency (%) 0 No answer provided 28a 1 Very light (6–10) 41 (17%) 2 Light (11–12) 100 (43%) 3 Somewhat hard (13–14) 73 (31%) 4 Hard or heavy (15–16) 12 (5%) 5 Extremely hard (17–20) 10 (4%)aOf 264 video interactions (11% with no response).
Table 3 also shows PAT training end points for all participants engaging with the program. The baseline daily step count (first week, run-in) was 1,083 (383–2,981) and 12 participants (57%) averaged <1,200 steps/d. During the best performance week past the run-in period, which corresponded to the 5th [4th–7th] week, participants were able to accomplish 3,508 (1,415–5,967) steps/d (vs 1,260 [639–3,081] at baseline; P < 0.001) and only 4 (22% vs 50% at baseline; P = 0.08) remained at the <1,200 steps/d category. Such improvement, however, was not maintained and the daily step count decreased to 958 (656–4,169) steps/day (vs 1,260 [639–3,081] at baseline; P = 0.55), with 10 participants below the 1,200 threshold (45% vs 50% at baseline; P = 0.5). Regardless, 7 participants (33%) were able to remain adherent with the walking program throughout the 12-week intervention by keeping more than two-thirds of their training weeks with increases of ≥500 steps/day above their baseline. When overall adherence to the training program was considered (i.e., video exercising or walking), we found that 57% (12/21) of patients extending past the run-in were adherent. Interestingly, 2 patients were so severely debilitated that their shuffle walk would not be recognized by the PAT. In both cases, as shown in Table 3, they were able to improve their stride and have their steps accounted for by the PAT while eliminating the need for any walking assistive device.
DISCUSSIONResearchers in the field of hepatology have expanded the physical fitness toolbox to include frailty (18,19), cardiopulmonary endurance (20,21), and sarcopenia (22,23) metrics. It is now clear that investigating an LT candidate's physiologic reserve through any of these metrics yields pivotal prognostic information (6,24). Furthermore, the effect is carried over to the post-LT period where physical fitness affects not only survivorship but also recovery and health-related quality of life, each of which leads to significant health care utilization and cost (14,25,26). In this pilot and feasibility study, we were able to demonstrate clinically meaningful changes to both LFI and 6MWT fitness metrics after a 12-week home-based exercise regimen, despite our population being composed of difficult-to-train participants (decompensation/HE features and highly prevalent obesity and frailty). A longitudinal observational study had previously shown that patients with an improved LFI (0.07 [0.03–0.17]) gained survival advantage against those with stable or worsening LFI (27). Furthermore, LFI improvements between 0.2 and 0.4 were associated with better survival in our cohort study of LT candidates (7). Although less data exist for 6MWT changes in LT candidates, we know from rehabilitation in other specialties that an increase in the order of 20–50 m constitute a meaningful change (7,28). As such, the improvement of 0.4 in LFI and 41 m in 6MWT achieved by participants in the current study are clinically meaningful. When considering frailty as a category, although only 1 of 3 participants who completed the study lost their frailty status, the other 2 improved their LFI and 6MWT by 0.47 and 96 m, and 1.05 and 14 m, respectively. No participant progressed into frailty by either LFI or 6MWT.
Our exercise intervention, which is scalable and generalizable, consisted of monitored EL-FIT exercise videos and walking, along with remote coaching by an exercise specialist. Exercise prescription was provided through the EL-FIT allocation algorithm using baseline clinical characteristics (12). The algorithm assigns patients to 1 of 3 categories: strength and mobility (lowest intensity), low-intensity, or moderate-intensity training. The prescription was easy to understand and could be followed, whether partially or in full adherence, by all participants. Lack of expertise to provide an exercise prescription at most transplant centers is one of the main limiting factors in making prehabilitation widely available, a hurdle the MATRIX initiative is aiming to solve. Thus, we tested whether EL-FIT provided an exercise prescription with proper training intensity. Importantly, the disagreement between our LT-PT and EL-FIT was not statistically significant, and in the 39% with discordant results, EL-FIT almost universally downplayed intensity and allocated 1 stage below the 1 deemed appropriate by our LT-PT. This is a safety feature of EL-FIT's stratification algorithm which can be easily corrected remotely using the EL-FIT trainer dashboard. These results provide further proof of concept that EL-FIT can be used by LT centers to prescribe exercise to candidates with AdvCLD.
Our home-based exercise program reached its feasibility goal by showing that more than two-thirds of participants engaged in study. We selected this threshold based on previous experience (attrition ≤36%) (8) and with the understanding that this novel intervention carried some technological challenges, which in turn could affect initial uptake. In fact, the main reasons for attrition were the time needed to complete the assessment/troubleshoot technology issues. This carries important feasibility information on making MATRIX accessible and user friendly to patients and providers, although the study allowed researchers to overcome a learning curve on smartphone apps and PAT. Regarding adherence to the program, we conformed to a dichotomous definition at the 50% threshold instead of definitions considering 2 levels of adherence (i.e., partial: 20–79% and full: ≥ 80%) to facilitate analysis and given the lack of precedent with telemonitored adherence. Our adherence figure at 57% represents both a gain from our previous studies (7,12) and is acceptable for a 12-week exercise trial in a difficult-to-train population while being in agreement with published literature (range: 14%–100% in cirrhosis) (8). In the end, both feasibility and adherence were affected by AdvCLD complicated course and high mortality (4/21), need for surgery (2/21), or hospitalizations (>50%). A multicenter study is needed to further refine our findings and the impact of exercise-driven LFI/6MWT changes on survival.
Interestingly, approximately half of the patients walked <1,200 steps/d, an inactivity level we previously showed to be a risk factor for hospital admission/mortality in AdvCLD (17). Although at the peak of their training subjects increased daily steps by ∼2,500 and almost 80% were able to walk ≥1,200 steps/d, walking reverted to baseline by the end of study. As disappointing this finding might be, it attests for physical self-efficacy (i.e., they had the physiological reserve to become fitter) and for the temporary nature of change in lifestyle modification. Alternatively, it is possible participants switched from walking to other types of exercise as an explanation for the drop in daily steps, something we identified during coaching sessions in few participants. Regardless, there is a need to complement the intervention with motivating strategies to maintain physical training for longer periods, particularly for patients without a living donor who need to maintain their improved fitness for months and until an organ becomes available. We had previously shown that the addition of EL-FIT to PAT improves monitoring maintenance, and a new version of the EL-FIT app clearing bugs affecting its gamification/notifications performance was relaunched after completion of this study. We are now looking into the development of novel and more efficient wearables able to document a wide range of training efforts, particularly when mobility is gravely affected as in shuffle walk or the use of an assistive device. We hope these strategies will help with uptake and maintenance of prehabilitation in LT.
Regarding usability, we were able to confirm that 76% of patients exercised with an EL-FIT video and rated their exertion. Participants' understanding of the need for exercising and the risks of poor physical fitness was verified during coaching sessions and served as added proof of app utilization. The gamification and social features of EL-FIT, such as leaderboard competition, earning of badges, ability to send emojis to other participants and push notifications, were appreciated by some participants and helped them remain focused on their training, as reported to their coaches. However, as learned from the only subject with an intervention-related adverse event (i.e., a mechanical fall), gamification features could have a downside because they might inappropriately push patients beyond their physiologic limits to gain their peer's recognition. In this regard, the corollary start low and go slow is of the utmost importance to prevent training-associated injuries which in turn disincentivize patients and bring exercise to a halt. These EL-FIT usability learning points will be considered during the development of future MATRIX studies.
Our study has some limitations. Most importantly, 10 participants (32%) did not engage in the intervention. However, no differences in basic clinical characteristics between those who engaged or not were noted, which suggests there is a need to better characterize exercise readiness before starting home-based exercise. Of note, 7 patients were recruited during the beginning of the COVID-19 pandemic, a time with limited access to subjects and caregivers. The emoji-based rate of perceived exertion showed that most participants exercising with EL-FIT videos did not train at moderate intensity. This was a surprising finding given that participants expressing insufficient exertion during their coaching session were moved up in intensity as needed. In fact, this was not an unresolved or recurrent concern during our multidisciplinary intervention fidelity monitoring meetings. Although improved physical fitness might be related to participant's familiarization with LFI and 6MWT, we believe this to be unlikely given that 6MWT and LFI (particularly balance component) rely on complex muscle utilization and cardiopulmonary endurance. Finally, the EL-FIT intervention depends on sufficient technology literacy from participants. We partially overcame this by considering patients whose caregiver was knowledgeable and committed to facilitate the intervention through their personal smartphone.
In conclusion, our EL-FIT tele-prehabilitation intervention was not only feasible, acceptable, and safe but also highly efficacious in that it meaningfully improved physical fitness in patients with AdvCLD. Although resolution of few technological challenges remains, our results, including an analysis of participant's interaction with the smartphone app data, speak of EL-FIT's potential as a virtual prehabilitation platform in LT and we look to a future multicenter confirmatory study.
CONFLICTS OF INTERESTGuarantor of the Article: Andres Duarte-Rojo, MD, MS, PhD.
Specific author contributions: All: study concept and design. A.D.R., P.M.R., R.K.G., C.B.H.: recruitment and data acquisition. A.D.R., J.M.J.: monitoring of intervention fidelity. A.D.R.: analysis and interpretation of data/drafting of manuscript. All: critical revision of manuscript and important intellectual content. A.D.R., J.M.J.: study supervision. All: final approval of the version to be published.
Financial support: Study was funded by the Pittsburgh Liver Research Center (PLRC; NIH-NIDDK P30DK120531) Pilot and Feasibility Program, Cycle 2019 (https://livercenter.pitt.edu/pilot-and-feasibility-grant-awardees-2019/). EL-FIT was developed with funds from the American Association for the Study of Liver Diseases (AASLD) Foundation, PLRC Pilot & Feasibility Funds, and an Innovation Grant (University of Pittsburgh Innovation Institute).
Potential competing interests: None to report.
Study Highlights
Comments (0)