
Remember me





In 1989, Unge et al (1) proposed dual therapy, comprising a proton pump inhibitor (PPI) and amoxicillin, for eradicating Helicobacter pylori infection. PPIs have been an essential component of H. pylori eradication regimens (2). Gastric acid inhibition is crucial for increasing the H. pylori eradication rate by stabilizing acid-labile antibiotics in the stomach and increasing the sensitivity of H. pylori to antibiotics (3). Currently, PPI-based triple therapy, which consists of a PPI, amoxicillin, and clarithromycin, is the most popular eradication regimen worldwide (2,4).
There have been attempts to increase the eradication rate by suppressing gastric acid secretion more effectively using potassium-competitive acid blockers (P-CAB), which exert a faster-onset and longer-lasting acid-inhibitory effect than PPIs (5). In a Japanese randomized controlled trial comparing P-CAB–based triple therapy with PPI-based triple therapy, vonoprazan, a P-CAB, was shown to increase the H. pylori eradication rate by nearly 17% points when compared with a PPI (6). In a meta-analysis on the comparative efficacy of vonoprazan vs PPI, vonoprazan-based triple therapy exhibited a 1.2-times better eradication rate than PPI-based triple therapy (7). The higher eradication rate of vonoprazan-based triple therapy compared with that of PPI-based triple therapy was due to the superior efficacy of vonoprazan-based triple therapy against clarithromycin-resistant strains. Recently, a multicenter trial conducted in the United States and Europe confirmed that vonoprazan-based triple therapy exerted superior efficacy to that of PPI-based triple therapy (8). In South Korea, tegoprazan, a new P-CAB, was approved in 2021 for treating H. pylori infection (9,10).
Regimens comprising therapeutic agents that can facilitate the efficacy of PPI have been explored, including a combination of PPI and antacids. Most PPIs are administered as enteric-coated formulations, which are necessary to protect the acid-labile PPI from acid degradation in the stomach. Accordingly, PPIs are limited because the absorption and onset of their antisecretory effects may be delayed. To overcome these limitations, an immediate-release formulation without an enteric coating containing PPI and sodium bicarbonate was developed (11,12). Sodium bicarbonate protects uncoated PPIs from degradation by gastric acid, enabling its rapid release and absorption and improving its onset of action (11,12). For example, esomeprazole/sodium bicarbonate can rapidly increase the plasma concentration of esomeprazole through sodium bicarbonate–mediated neutralization of gastric acid and stabilization of esomeprazole in the stomach (13). In South Korea, esomeprazole/sodium bicarbonate, which has a faster onset of action than esomeprazole monotherapy, is available for acid-related disorders, such as gastroesophageal reflux disease (14).
Both P-CABs and PPIs/sodium bicarbonate are promising therapeutics for rapid symptom control in patients with gastric acid–related disorders. Tegoprazan and esomeprazole/sodium bicarbonate have been reported to increase the intragastric pH to more than 4 within 1 hour of administration (13,15). In addition, these agents may be effective in H. pylori eradication. However, no previous report has explored the comparative efficacies of P-CABs and PPIs/sodium bicarbonate in H. pylori eradication therapy. In addition, adverse events associated with PPI/sodium bicarbonate–based H. pylori eradication therapy are yet to be established. Therefore, in this study, we aimed to compare the efficacy and adverse events of tegoprazan and esomeprazole/sodium bicarbonate–based triple therapies in real-world settings.
METHODS Study populationAdult patients (aged 19 years or older) with H. pylori infection treated with tegoprazan-based triple therapy or esomeprazole/sodium bicarbonate–based triple therapy between March 2021 and November 2022 at Kangbuk Samsung Hospital were eligible for study inclusion. Patients with a history of H. pylori eradication therapy or subtotal gastrectomy were excluded. We retrospectively reviewed data on patient demographics, symptoms, upper endoscopic findings, comorbidities, medications, adverse events, and results of H. pylori eradication therapy. The institutional review board of the ethics committee approved this study (Kangbuk Samsung Hospital: KBSMC 2022-11-009). Given the retrospective nature of this study, the need for informed consent was waived.
H. pylori eradication therapyThe tegoprazan-based and esomeprazole/sodium bicarbonate–based eradication regimens were selected according to the clinician's preference in a real-world setting. The patients were classified into 2 groups according to the H. pylori eradication regimen as follows: (i) tegoprazan-based triple therapy group, twice daily doses of 50 mg of tegoprazan + 1,000 mg of amoxicillin + 500 mg of clarithromycin for 14 days; and (ii) esomeprazole/sodium bicarbonate–based triple therapy group, twice daily doses of 40/800 mg of esomeprazole/sodium bicarbonate + 1,000 mg of amoxicillin + 500 mg of clarithromycin for 14 days. Confirmation tests for successful eradication were performed at least 4 weeks after treatment. If first-line H. pylori eradication therapy failed, second-line eradication therapy was performed with bismuth-containing quadruple therapy as follows: (i) acid suppressant (either 50 mg of tegoprazan or 20 mg of rabeprazole) twice daily in combination with 120 mg of bismuth 4 times a day, 500 mg of metronidazole 3 times a day, and 500 mg of tetracycline 4 times a day for 14 days. The success of second-line eradication therapy was evaluated after ≥4 weeks of treatment.
Study end point and measurementsThe primary study end point was the H. pylori eradication rate with first-line treatment in an intention-to-treat (ITT) analysis. The secondary study end points were as follows: H. pylori eradication rate with first-line therapy in the per-protocol (PP) analysis, eradication rate with second-line treatment in the ITT and PP analyses, and adverse events associated with H. pylori eradication therapy.
One or more of the following tests were used to confirm the successful eradication of H. pylori infection: the 13C-urea breath test (Korea Otsuka Pharmaceutical Co., Ltd, Seoul, Korea) and histological evaluation with modified Giemsa staining. If any of the 2 tests were positive, H. pylori eradication was considered to have failed.
We visually assessed the severity of atrophic gastritis based on the Kimura-Takemoto classification as follows (16): mild (C-1 and C-2), moderate (C-3 and O-1), and severe (O-2 and O-3). Drug adherence was defined as the administration of ≥80% of prescribed medications. The severity of adverse events was assessed as mild (transient symptoms that improved spontaneously), moderate (symptoms that required management), or severe (symptoms that led to emergency visits) (17).
Statistical analysisContinuous variables, presented as mean ± SD, were compared using the Student t test. Categorical variables, presented as numbers with proportions, were compared using the Fisher exact test. Patients who did not receive sufficient medication (<80% of the prescribed medications) or were lost to follow-up were considered to have failed to achieve a cure in the ITT analysis. For PP analysis, patients with insufficient medications and those lost to follow-up were excluded. Logistic regression analysis was performed to identify factors associated with the failure of first-line H. pylori eradication therapy. Variables with P values <0.1 in the univariable logistic regression model were included as covariates in the multivariable analysis. P < 0.05 was deemed statistically significant. Data analyses were conducted using the R statistical software (version 4.2.2; R Foundation for Statistical Computing, Vienna, Austria).
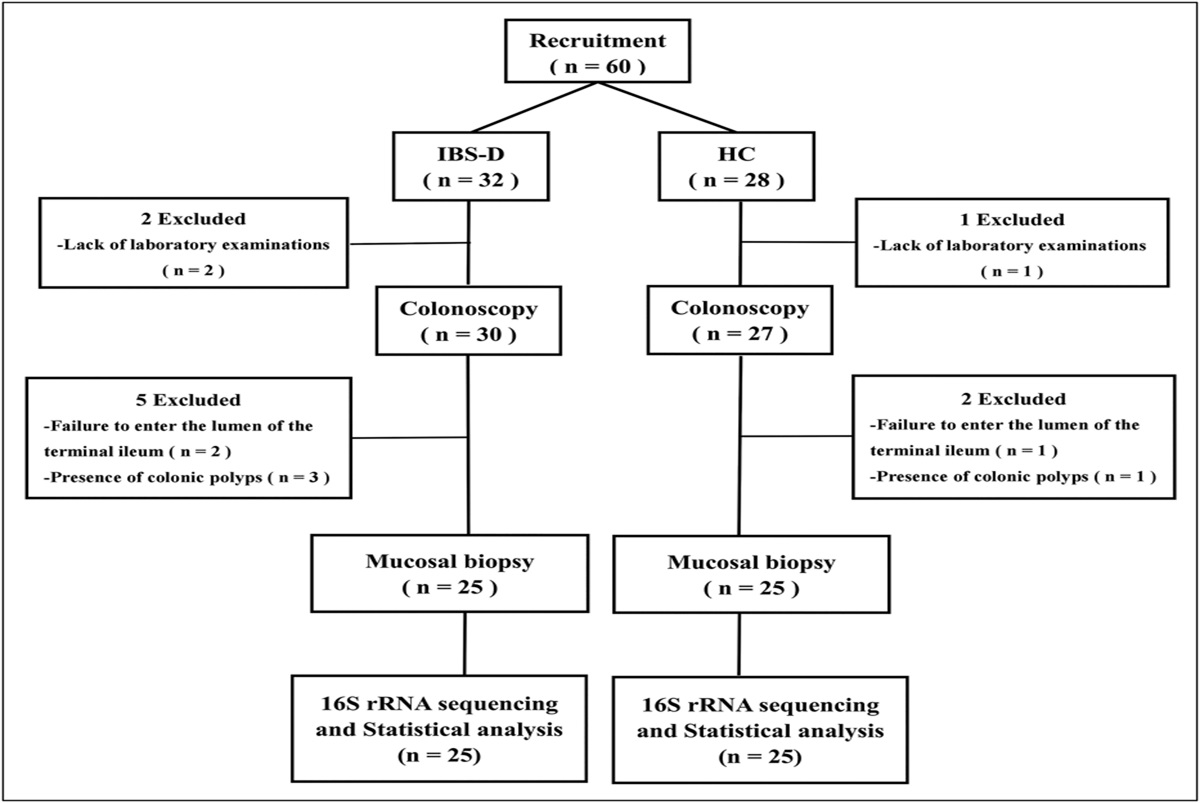
RESULTS Study population and baseline characteristicsIn total, 883 patients who received tegoprazan-based or esomeprazole/sodium bicarbonate–based triple therapy for H. pylori infection were included in this study (Figure 1). After excluding 29 patients with a history of H. pylori eradication therapy or subtotal gastrectomy, 854 patients were included in the ITT analysis. Of them, 435 patients had undergone 14-day tegoprazan-based triple therapy, while 419 patients had received a 14-day esomeprazole/sodium bicarbonate–based triple therapy. After excluding 6 patients with insufficient medication and 64 who were lost to follow-up, 399 and 385 patients in the tegoprazan-treated and esomeprazole/sodium bicarbonate–treated groups, respectively, remained in the PP population. Second-line H. pylori eradication therapy was administered to 107 patients in whom first-line eradication therapy failed to treat the H. pylori infection.
 Figure 1.:
Figure 1.: Study flow diagram. aInsufficient medication is determined as administration of <80% of prescribed medications. PBMT indicates bismuth-containing quadruple therapy comprising PPI (or P-CAB), bismuth, metronidazole, and tetracycline. ITT, intention-to-treat; P-CAB, potassium-competitive acid blocker; PP, per-protocol; PPI, proton pump inhibitor.
Table 1 summarizes the baseline characteristics of included patients. The mean age was 56.0 ± 11.6 years in the tegoprazan group and 57.1 ± 10.9 years in the esomeprazole/sodium bicarbonate group (P = 0.155). The proportion of males was 55.6% and 50.1% in the tegoprazan and esomeprazole/sodium bicarbonate groups, respectively (P = 0.107). Hypertension was more common in the esomeprazole/sodium bicarbonate group than in the tegoprazan group (28.6% vs 21.6%, P = 0.018). Antithrombotic agents, particularly aspirin, were more commonly taken by patients in the esomeprazole/sodium bicarbonate group than those in the tegoprazan group (any antithrombotic agent: 12.6% vs 7.1%, P = 0.007; aspirin: 7.9% vs 3.4%, P = 0.005).
Table 1. - Baseline characteristics of included patients Variable 14-d tegoprazan-based triple therapy (N = 435) 14-d esomeprazole/sodium bicarbonate–based triple therapy (N = 419) P value Age, y, mean ± SD 56.0 ± 11.6 57.1 ± 10.9 0.155 Male, n (%) 242 (55.6) 210 (50.1) 0.107 BMI,a kg/m2, mean ± SD 24.3 ± 3.3 24.2 ± 3.4 0.827 Smoking habit 0.415 Never smoker 247 (56.8) 253 (60.4) Former smoker 117 (26.9) 110 (26.3) Current smoker 71 (16.3) 56 (13.4) Alcohol use 0.238 Absent 235 (54.0) 218 (52.0) Present <2/wk 128 (29.4) 113 (27.0) ≥2/wk 72 (16.6) 88 (21.0) Comorbidity Hypertension 94 (21.6) 120 (28.6) 0.018 Cardiovascular disease 17 (3.9) 22 (5.3) 0.347 Diabetes 44 (10.1) 57 (13.6) 0.114 Cerebrovascular accident 12 (2.8) 8 (1.9) 0.412 Antithrombotic agent Any antithrombotic agent 31 (7.1) 53 (12.6) 0.007 Aspirin 15 (3.4) 33 (7.9) 0.005 Clopidogrel 12 (2.8) 18 (4.3) 0.223 Other antiplatelet agent 4 (0.9) 4 (1.0) > 0.999 Warfarin 0 (0.0) 1 (0.2) 0.491 NOAC 2 (0.5) 2 (0.5) > 0.999 Others (types unknown) 2 (0.5) 1 (0.2) > 0.999BMI, body mass index; NOAC, nonvitamin K–dependent oral anticoagulant; N/A, not applicable.
aBMI is missing in 1 patient in the triple therapy group.
Table 2 summarizes baseline patient symptoms and endoscopic findings. The most common indication for H. pylori eradication was H. pylori-associated gastritis in both groups (tegoprazan vs esomeprazole/sodium bicarbonate: 83.4% vs 89.5%). Atrophic gastritis was more common in the esomeprazole/sodium bicarbonate group than in the tegoprazan group (96.4% vs 79.3%, P < 0.001).
Table 2. - Baseline symptoms and endoscopic findings Variable 14-d tegoprazan-based triple therapy (N = 435) 14-d esomeprazole/sodium bicarbonate–based triple therapy (N = 419) P value Symptom Reflux symptoma 10 (2.3) 13 (3.1) 0.468 Nausea or vomiting 7 (1.6) 8 (1.9) 0.739 Abdominal discomfort 93 (21.4) 89 (21.2) 0.961 Abdominal pain 12 (2.8) 9 (2.1) 0.565 Othersb 12 (2.8) 22 (5.3) 0.063 Indication for H. pylori eradication 0.033 Gastric and duodenal ulcers 2 (0.5) 1 (0.2) Gastric ulcer 26 (6.0) 16 (3.8) Duodenal ulcer 30 (6.9) 24 (5.7) MALT lymphoma 1 (0.2) 0 (0.0) EGC treated with ESD 10 (2.3) 1 (0.2) Gastric adenoma treated with ESD 3 (0.7) 2 (0.5) H. pylori–associated gastritis 363 (83.4) 375 (89.5) Nodular gastritisc 23 (5.3) 27 (6.4) 0.472 Atrophic gastritisc,d <0.001 Absent (C-0) 90 (20.7) 15 (3.6) Present C-1 112 (25.8) 81 (19.3) C-2 53 (12.2) 63 (15.0) C-3 71 (16.4) 88 (21.0) O-1 47 (10.8) 99 (23.6) O-2 43 (9.9) 58 (13.8) O-3 18 (4.1) 15 (3.6)EGC, early gastric cancer; ESD, endoscopic submucosal dissection; MALT, mucosa-associated lymphoid tissue.
aReflux symptoms include heartburn and acid regurgitation.
bOther symptoms include globus sensation, anorexia, and belching.
cThere are 2 missing values for nodular gastritis and atrophic gastritis in the triple therapy group.
dSeverity of atrophic gastritis is determined by the Kimura-Takemoto classification (15).Figure 2 shows the success rate of first-line H. pylori eradication therapy. In the ITT population, there was no significant difference in eradication rates between the tegoprazan and esomeprazole/sodium bicarbonate groups (78.6% [95% confidence interval (CI), 74.6–82.3%] vs 81.4% [95% CI, 77.4–84.9%], P = 0.313). The PP analysis also revealed a similar eradication rate between the 2 groups (tegoprazan vs esomeprazole/sodium bicarbonate: 85.5% [95% CI, 81.8–87.5%] vs 87.8% [95% CI, 84.1–90.7%], P = 0.339).
 Figure 2.:
Figure 2.: Success rate of first-line H. pylori eradication therapy. ITT, intention-to-treat; PP, per-protocol.
Considering the 107 patients who received second-line therapy, 83 received 14-day tegoprazan-based bismuth-containing quadruple therapy, while 24 received 14-day rabeprazole-based bismuth-containing quadruple therapy (Figure 2). There were no significant differences between the groups in either ITT or PP analysis (tegoprazan-based quadruple vs rabeprazole-based quadruple: ITT, 84.3% [95% CI, 75.4–90.9%] vs 87.5% [95% CI, 70.3–96.4%], P = 0.703; PP, 95.8% [95% CI, 89.3–98.8%] vs 95.2% [95% CI, 79.8–99.5%], P = 0.906) (See Supplementary Figure S1, Supplementary Digital Content, https://links.lww.com/CTG/A990). We further analyzed previous eradication regimens in patients who received second-line therapy. Of the 83 patients who received tegoprazan-based quadruple therapy as second-line treatment, 52 (62.7%) received tegoprazan-based triple therapy and 31 (37.3%) received esomeprazole/sodium bicarbonate-based triple therapy as first-line treatment. Conversely, of the 24 patients who received rabeprazole-based quadruple therapy, 15 (62.5%) received esomeprazole/sodium bicarbonate-based triple therapy, while 9 (37.5%) received tegoprazan-based triple therapy.
Treatment adherence and adverse eventsTable 3 summarizes the adherence and adverse events associated with the first-line H. pylori eradication therapy. Adherence was >90% in both groups (tegoprazan vs esomeprazole/sodium bicarbonate: 91.7% vs 91.9%, P = 0.932). However, the overall adverse event rate was higher in the esomeprazole/sodium bicarbonate group than that in the tegoprazan group (39.4% vs 28.0%, P < 0.001). Both groups experienced mild or moderate adverse events. Specifically, abdominal discomfort and diarrhea were more common in the esomeprazole/sodium bicarbonate group than in the tegoprazan group (abdominal discomfort: 1.1% vs 3.8%, P = 0.012; diarrhea: 9.9% vs 21.2%, P < 0.001).
Table 3. - Adherence and adverse events of first-line H. pylori eradication therapy Variable 14-d tegoprazan-based triple therapy (N = 435) 14-d esomeprazole/sodium bicarbonate–based triple therapy (N = 419) P value Adherence,a n (%) 399 (91.7) 385 (91.9) 0.932 Loss of follow-up 33 (7.6) 31 (7.4) 0.917 Insufficient medication 3 (0.7) 3 (0.7) > 0.999 Adverse event,b n (%) Any adverse event 122 (28.0) 165 (39.4) < 0.001 Mild 119 (27.4) 162 (38.7) Moderate 3 (0.7) 3 (0.7) Severe 0 (0.0) 0 (0.0) General weakness 1 (0.2) 1 (0.2) > 0.999 Dizziness 1 (0.2) 0 (0.0) > 0.999 Headache 2 (0.5) 3 (0.7) 0.681 Myalgia 0 (0.0) 0 (0.0) N/A Acid regurgitation 1 (0.2) 2 (0.5) 0.618 Nausea or vomiting 14 (3.2) 16 (3.8) 0.634 Dysgeusia 53 (12.2) 62 (14.8) 0.263 Abdominal discomfort 5 (1.1) 16 (3.8) 0.012 Abdominal pain 2 (0.5) 8 (1.9) 0.060 Diarrhea 43 (9.9) 89 (21.2) < 0.001 Constipation 3 (0.7) 2 (0.5) > 0.999 Skin rash 8 (1.8) 2 (0.5) 0.108 Othersc 2 (0.5) 5 (1.2) 0.279aAdherence is determined as administration of ≥80% of prescribed medications.
bPercentage is calculated based on the ITT population.
cOther adverse events include insomnia, dry mouth, and sores on the tongue.
Adherence and adverse events associated with second-line therapy are listed in Supplementary Table S1 (see Supplementary Digital Content, https://links.lww.com/CTG/A991). Although the incidence of most adverse events did not differ between the rabeprazole-based and tegoprazan-based quadruple therapies, the tegoprazan-based quadruple therapy group exhibited a higher incidence of diarrhea than the rabeprazole-based quadruple therapy group (22.8% vs 4.2%, P = 0.040).
Factors associated with failure of H. pylori eradicationTable 4 summarizes the logistic regression model for the failure of first-line H. pylori eradication therapy. Although univariable analysis revealed that sex, smoking habits, and alcohol use were associated with eradication failure, no significant associations were identified after adjusting for confounding variables. In addition, the eradication regimen (tegoprazan-based vs esomeprazole/sodium bicarbonate-based triple therapy) was not independently associated with failure of first-line H. pylori eradication.
Table 4. - Factors associated with failure of first-line H. pylori eradicationa Variable N Failure n (%) Univariable analysis Multivariable analysis OR (95% CI) P-value OR (95% CI) P-value Treatment duration 14-day tegoprazan-based triple therapy 399 58 (14.5) 1 1 14-day esomeprazole/sodium bicarbonate–based triple therapy 388 47 (12.1) 0.81 (0.54–1.23) 0.318 0.81 (0.53–1.25) 0.344 Adherence Adherent 783 105 (13.4) 1 Nonadherent 4 0 (0.0) N/A 0.999 Age, yr <60 452 54 (11.9) 1 ≥60 335 51 (15.2) 1.32 (0.88–2.00) 0.182 Sex Male 416 38 (9.1) 1 1 Female 371 67 (18.1) 2.19 (1.43–3.36) <0.001 1.62 (0.90–2.92) 0.110 BMI, kg/m2 <25 474 66 (13.9) 1 ≥25 313 39 (12.5) 0.88 (0.58–1.35) 0.555 Smoking habit Never smoker 463 76 (16.4) 1 1 Former smoker 210 19 (9.0) 0.51 (0.30–0.86) 0.012 0.82 (0.42–1.61) 0.566 Current smoker 114 10 (8.8) 0.49 (0.25–0.98) 0.044 0.79 (0.34–1.82) 0.575 Alcohol use Absent 422 68 (16.1) 1 1 <2/wk 222 28 (12.6) 0.75 (0.47–1.21) 0.779 0.95 (0.57–1.59) 0.854 ≥2/wk 143 9 (6.3) 0.35 (0.17–0.72) 0.004 0.55 (0.25–1.20) 0.135 Comorbidity Hypertension 198 27 (13.6) 1.03 (0.65–1.66) 0.888 Cardiovascular disease 38 4 (10.5) 0.76 (0.26–2.17) 0.602 Diabetes 92 16 (17.4) 1.43 (0.80–2.57) 0.226 Cerebrovascular accident 19 2 (10.5) 0.76 (0.17–3.34) 0.716 Antithrombotic agent 77 9 (11.7) 0.85 (0.41–1.75) 0.654 Symptom Reflux symptomb 19 2 (10.5) 0.76 (0.17–3.34) 0.716 Nausea or vomiting 13 2 (15.4) 1.18 (0.26–5.42) 0.827 Abdominal discomfort 168 30 (17.9) 1.58 (0.99–2.51)
Comments (0)