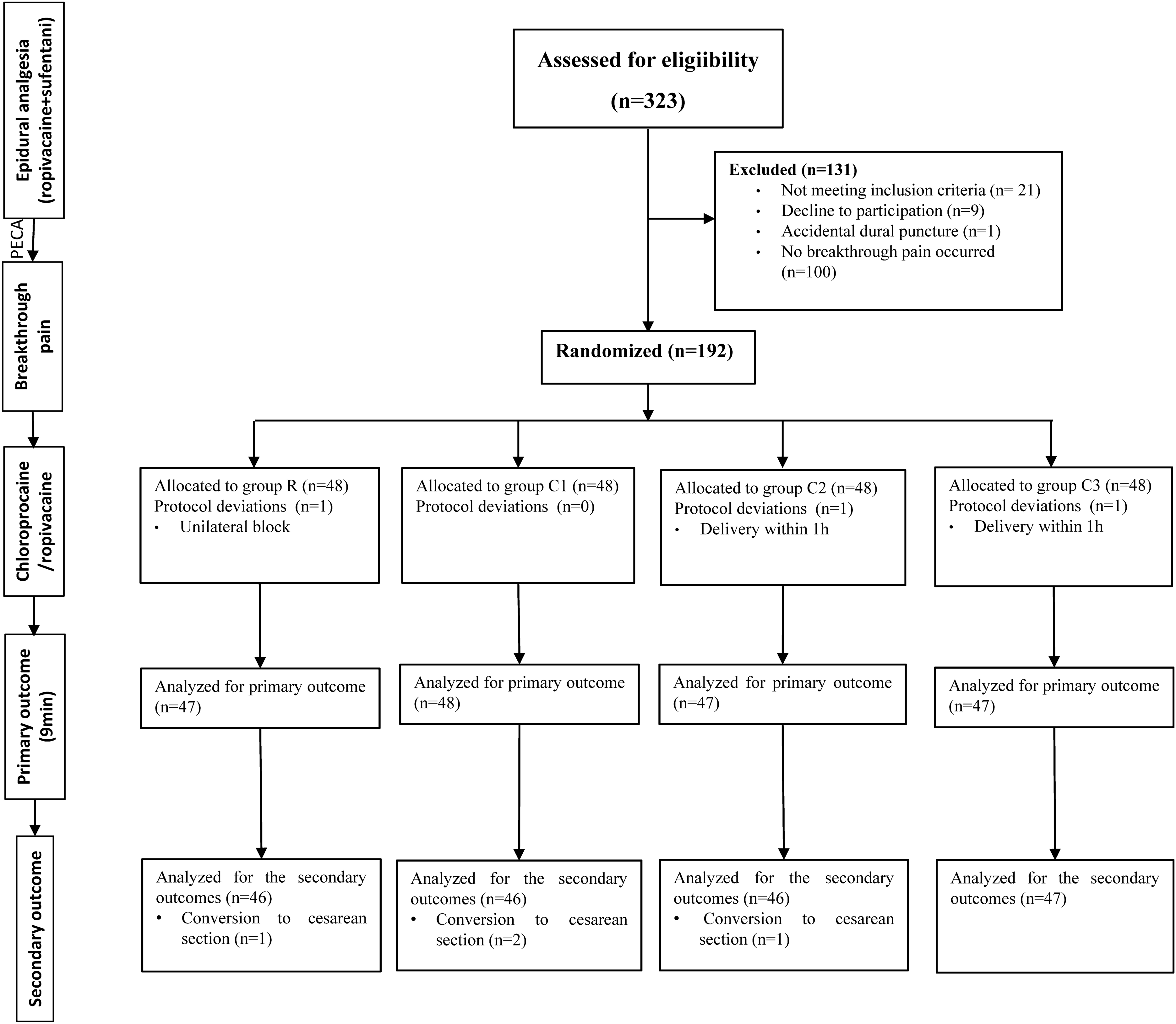
This study evaluated the efficacy and safety of Elosan Cabin C1 whole-body electrostatic therapy in adults with chronic pain over a study period of eight weeks (Fig. 2). The outcomes assessed were pain relief, impact on quality of life and sleep quality in 192 patients. Elosan therapy, in combination with continued conservative treatment, was effective in relieving chronic pain: A total of 61% of the patients experienced an improvement in their pain condition, defined as a reduction of at least 15 points on the VAS pain scale. The overall VAS pain score reduction was 30.9%. Along with pain reduction, there was significant improvement in mobility and physical activity as measured by the SF-12 Physical Component Summary (PCS, + 18%). Regarding sleep quality, 32% of patients reported improvement, with an overall increase of 13% (seven-point Likert scale). These results are in line with the results of the preliminary ELO02 study, where similar improvements in pain, quality of life and sleep quality have been reported [16]. The subgroup analysis showed that patients with long-standing pain conditions and those on prolonged pharmacotherapy also benefited from the treatment. However, female patients were significantly more likely to respond to Elosan treatment if their pain had lasted less than a year. Considering the pathophysiology of pain chronification and the potential development of a chronic pain syndrome over time, this effect is plausible, as the longer the duration of pain, the more challenging the treatment becomes.
Pain on the one hand and inactivity, psychological distress, and sleep problems on the other have a bidirectional relationship and influence each other [12]. The aim of multimodal pain management must therefore be not only to reduce pain, but also to increase mobility despite pain, restore psychological resilience and improve sleep quality. Physical therapy, using either an exercise or a manipulative approach, attempts to restore flexibility, normal muscle function and muscle strength. Exercise can influence the body's pain modulation system and slightly reverse central sensitization [26]. In the long term, overall pain and functional status can be improved. However, the success of physical therapy is often limited by the underlying pain and the short duration of the treatment sessions in a limited window of time [27]. In addition to exercise, multimodal approaches may also include relaxation techniques such as progressive muscle relaxation and mindfulness meditation. These have been shown to be effective in several types of chronic pain, by reducing central sensitization and pain levels [28]. However, not all patients are open to and suitable for such techniques. The evidence for relaxation techniques is weak [29, 30]. Another possible adjunct in the treatment of chronic pain is the use of massage therapy. There is a large body of literature on different types of massage for different types of pain. Overall, a review of the current literature by Lin et al. found limited positive evidence that massage therapy is effective in pain management, at least in the short term [30]. A complementary method with the largest body of evidence is acupuncture. There is a considerable number of RCTs investigating acupuncture for the treatment of chronic pain and associated comorbidities such as depression and sleep disorders. Most of the reviewed trials show some efficacy in improving pain, reducing opioid use, and improving sleep quality and depression [30,31,32,33]. However, there is a lack of standardization in the way acupuncture is studied. This makes it difficult to compare different studies and the level of evidence varies [33, 34]. As well as the methods mentioned above, there is a wide range of other modalities that can be used to treat chronic pain, such as Yoga, Pilates, Tai Chi, osteopathy, spine manipulation, low level laser, or operant and cognitive behavioral therapies. Overall, complementary methods are in high demand by patients and are recommended in the literature as an adjunct to pharmacological and invasive pain treatments, but lack high quality scientific evidence [12, 29,30,31, 35].
In addition to the conservative methods described, there has been a development of electrical and magnetic therapies for acute and chronic pain: magnetic or electrical transcranial stimulation, transcutaneous electrical nerve stimulation (TENS) and the electrostatic treatment under investigation. Direct electrical or magnetic transcranial stimulation of the brain has been validated as an effective treatment for various types of chronic pain in Grade B trials, but there is still a great deal of heterogeneity in the literature, which makes it difficult to give precise recommendations. The treatment is also not yet widely available to patients [36,37,38,39]. TENS has been shown to be effective for musculoskeletal and neuropathic pain, but the effect is short-lived and has little effect on central pain modulation [40,41,42]. The underlying mechanisms of pain relief by TENS and transcranial stimulation are not fully understood but appear to be different. Whereas TENS is thought to have a peripheral target that may affect central pain processing over time, transcranial stimulation is thought to have a direct effect on the brain's neuroplasticity [36, 37].
The neurological mechanisms behind the effects of the electrostatic treatment are also still the subject of research. Clinically, our results show a significant improvement of various pain entities and sleep quality with a lasting effect, at least for the period observed. Because of this non-pain specific and sustained effect, we also suggest a central effect on neuroplasticity in the brain. As the electrostatic field has only superficial penetration into the skin [43], this central effect is most likely achieved by influencing afferent pathways via receptors in the skin. The significant improvement in mobility seen in the PCS could be explained by centrally mediated muscle relaxation. In comparison to the above methods of complementary pain treatment, electrostatic therapy is a promising treatment option that has both immediate and long-term effects on chronic pain and quality of life. However, to achieve the best possible effect in pain management, several methods should be combined to address the different comorbidities of chronic pain. Electrostatic treatment with the Elosan Cabin C1 can be a useful adjunct to rapidly reduce pain and increase mobility and resilience to exercise, especially in cases where musculoskeletal and soft tissue pain are dominant. As a result, physiotherapy can be used more effectively as part of the treatment regimen. Better pain control and improvements in sleep and quality of life could then improve psychological resilience and support psychosomatic therapy. Elosan treatment should therefore not be seen as a stand-alone treatment, but as an adjunct to physical therapy, psychosomatic therapy and other complementary treatment options aimed at restoring resilience in the patient's daily life. All these options can work in conjunction with pharmacology but may allow the patient to reduce the use of analgesics and especially opioids.
The Elosan treatment itself takes a minimal amount of time (8 min) and causes no pain. There were no safety events or serious side effects throughout the study. The treatment is always carried out according to the same schedule and does not need to be adapted to the individual patient. Therefore, after an initial consultation with the doctor, the treatment can be administered by the staff of a medical practice. In our study, this was the case in most of the trial sites. Due to the simplicity of the treatment and the possibility to delegate the process, Elosan therapy can be easily implemented in the daily routine of an ambulatory pain clinic.
As with all subjective outcomes, we found a very high variance in the measured outcome parameters. Therefore, our study must be interpreted with caution. A further limitation is the lack of a control group (continuation of the standard therapy without Elosan treatment or a sham treatment). The idea of a randomized control trial has been rejected on the basis of experiences made during the previous Elosan study ELO02 [16]: The nature of electrostatic treatment, with its clear perceptible effect on the patients' skin, precluded sham treatment during the planned study period, and no reliable control group could have been established. In addition, in the outpatient setting, it would not have been feasible to have a control group with standard treatment only. Without a control group, the measured effect of improved pain is based on the combined treatment of Elosan and continued standard therapy. However, the temporal relationship between pain improvement and the start of Elosan therapy strongly suggests efficacy, as most of the patients had a long history of pain and were in a steady state with their conservative pain therapy. Moreover, it was not possible to control for non-specific effects of the treatment under the given circumstances. A certain degree of placebo effect is to be expected with the treatment set-up in the cabin. In this trial, patients were followed for 8 weeks. This is a relatively short time interval compared with the long period of chronic pain before treatment. Long-term pain development and recurrence after treatment were not followed beyond the treatment period. In contrast to the precursory study ELO02 (16), the current study had sufficient power for the outcomes studied, with 143 complete data sets. However, the male subject group was smaller than the expected sample size of 56 (underpowered) and was underrepresented compared to the female subjects (105 women vs. 38 men). This may explain the significantly higher response rate in the female population (67%) compared to the male subjects (45%).
There is still insufficient data on the potential benefits of different configurations of an electrostatic field. Electrostatic exposure of the human body is a natural phenomenon with no evidence of harmful effects (21). To date, the treatment regimen (8 min with a total of six charges of a fixed voltage dose) has been established empirically without scientific analysis of the ideal voltage or duration of the pulses. Further research should investigate the most effective forms of electrostatic field application for the desired indications. The underlying mechanisms and optimal treatment combinations in a multimodal treatment approach should also be further investigated.
The study included only patients with chronic pain. From the experience gained in this study, one mechanism of pain reduction in musculoskeletal pain could be muscle relaxation. Therefore, Elosan treatment could be helpful in the treatment of various acute musculoskeletal conditions, such as low back pain, shoulder pain and acute postoperative pain. Extrapolating from our results, there may also be a positive effect on recovery after intense exercise in athletes. Further research is needed to investigate both the effects on acute pain and musculoskeletal recovery after exercise and surgery.


留言 (0)