
記住我





Periampullary diverticulum (PAD) is an extraluminal outpouching of duodenal mucosa near the ampulla of Vater.1 It has been reported in 4 to 7 percent of patients, usually incidentally during endoscopic retrograde cholangiopancreatography (ERCP). Although most remain asymptomatic, associated conditions, such as recurrent cholangitis and pancreatitis, have been reported.2 Severe complications, such as perforation, are uncommon and usually reported to occur during ERCPs.3 Treatment options are typically either surgical or conservative, with limited data on endoscopic closure.4 We report a case of a spontaneous perforated PAD within a larger duodenal diverticulum, which was treated endoscopically using a combination of argon plasma coagulation (APC) and an over-the-scope clip (OTSC; Ovesco, Tuebingen, Germany).
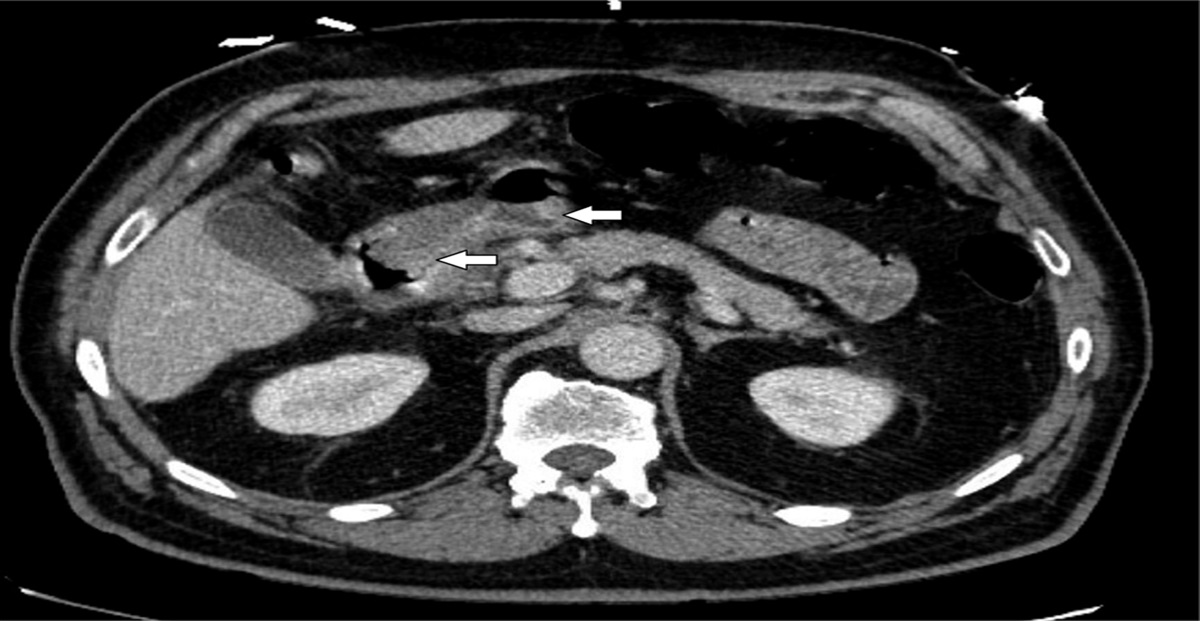
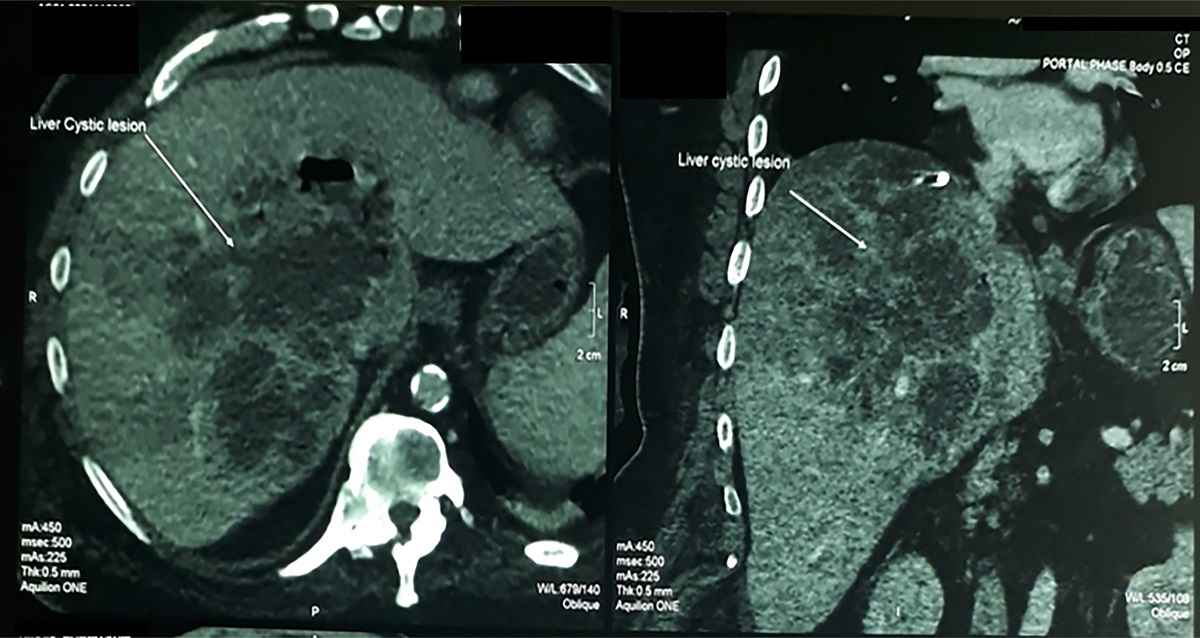
CASE REPORTA 76-year-old woman with a history of kidney donation and gastroesophageal reflux disease initially presented with severe right upper quadrant abdominal pain and vomiting. Physical examination revealed guarding with rebound tenderness. A computed tomography was performed because of suspected luminal organ perforation. This revealed a large periampullary duodenal diverticulum with pneumoperitoneum, concerning for a spontaneous duodenal perforation. The patient was taken emergently for an exploratory laparotomy, and the duodenal perforation was closed with an omental patch. Owing to high suspicion of incomplete closure, despite the patient being asymptomatic, a follow-up computed tomography with oral contrast on postoperative day 7 was performed. It demonstrated ongoing perforation with extraluminal fluid and air along the third and fourth portions of the duodenum. After a multidisciplinary discussion between surgery and gastroenterology, the decision was made to proceed with endoscopic evaluation and possible closure of the duodenal perforation. On the initial esophagogastroduodenoscopy, a large 5 cm diverticulum was seen in the proximal second portion of the duodenum. Within this diverticulum, there was a second smaller diverticulum, which had a 1 cm perforation at its 4 o'clock rim. The ampulla of Vater was also located within the smaller diverticulum but along the opposite rim (8 o'clock) (Figure 1). The contrast enterogram confirmed extravasation at the perforation site. Initially, the defect was closed partially with a through-the-scope suturing system (Xtack; Apollo EndoSurgery, Austin, TX), along with a loop snare device (Endoloop Ligature; Ethicon, Raritan, NJ) anchored with 3 endoclips. Intraoperatively, contrast injection showed a persistent, although smaller, extravasation compared with the previous one. A follow-up upper gastrointestinal series was performed on postoperative day 4 to assess healing and possible spontaneous closure; however, it confirmed a persistent leak (Figure 2). After a discussion with the surgery team, the decision was made to reattempt endoscopic closure.
 Figure 1.:
Figure 1.: The periampullary perforation and ampulla of Vater were both located within the smaller diverticulum.
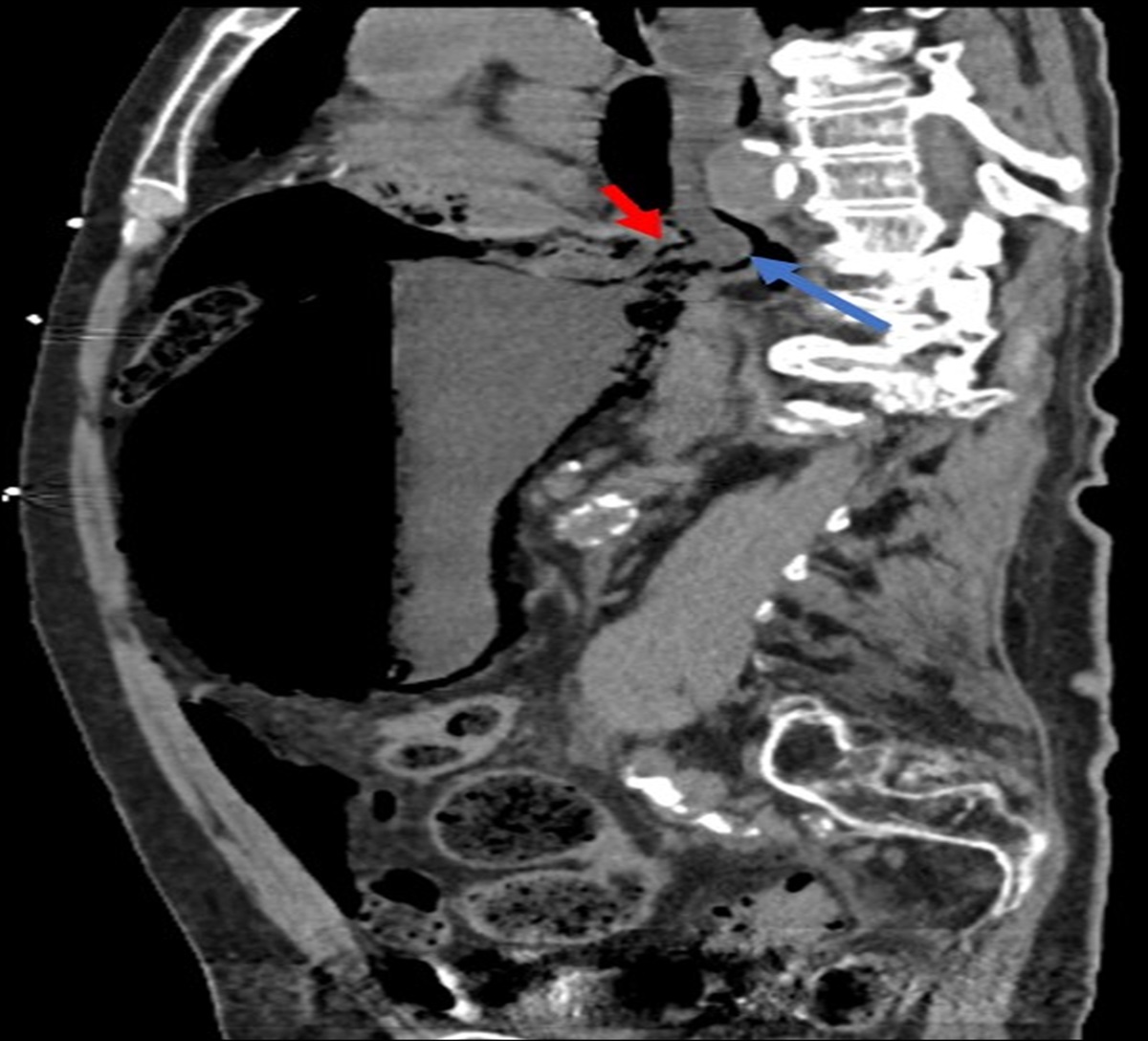
 Figure 2.:
Figure 2.: Upper gastrointestinal series demonstrating contrast extravasation at the perforation site, confirming an ongoing diverticular perforation (red arrow).
On repeat endoscopy, the previously placed endoclips, loop snare device, and suture with tacks were removed with the use of snare, rat-tooth forceps, and endoscopic surgical scissors (Olympus, Center Valley, PA). There was now a persistent 1 cm perforation seen within the small periampullary diverticulum. ERCP was then performed. A cholangiogram was performed, without evidence of biliary leak or filling defect. A plastic straight biliary stent (10 French by 7 cm, Advanix; Boston Scientific, Marlborough, MA) and pancreatic stent (5 French by 5 cm, Geenen; Cook Medical, Bloomington, IN) were placed to mark the biliary and pancreatic orifices and to avoid potential ductal injury during the closure. The site of the perforation within the diverticulum was friable, edematous, and fibrotic; therefore, straight-fire APC was used to treat the margins of the defect (Figures 3 and 4). The gastroscope was then fitted with a 12 mm OTSC. The defect site was suctioned into the cap, and the OTSC was deployed (Figure 5). The contrast was again injected using the sphincterotome and revealed no evidence of further extraluminal contrast extravasation.
 Figure 3.:
Figure 3.: Friable, edematous, and fibrotic margin of the diverticular perforation.
 Figure 4.:
Figure 4.: Coagulating the diverticular perforation margins with straight fire argon plasma coagulation in preparation for clip closure deployment.
 Figure 5.:
Figure 5.: An over-the-scope clip was placed for perforation closure (red arrow); pancreatic and biliary ductal stents were placed to protect ductal patency before clip deployment.
The patient recovered well with no postprocedural adverse events. At 1-week post-endoscopic closure, an upper gastrointestinal series showed the resolution of the leak. At 6 weeks, a follow-up endoscopy and ERCP were performed, which confirmed a complete closure of the prior defect. The plastic biliary and pancreatic stents were also removed at that time.
DISCUSSIONPAD is defined as an outpouching of the duodenal wall within 3 centimeters of the major papilla. Some PAD contains the major papilla inside, and these are called intradiverticular papilla (IDP). A meta-analysis has shown PAD with IDP to associate with significantly higher risks of complications, such as pancreatitis, bleeding, and perforation.5 The mortality rate with PAD perforation is extremely high, reported at 18% after surgical management and 24.3% for nonoperative therapy. Recently, endoscopic closures have begun to emerge as an alternative management option for duodenal diverticula perforation. Techniques described include endoscopic nasobiliary drainage and endoscopic retrograde biliary drainage. There has been very limited literature on PAD perforation, especially in those with a concurrent IDP.
To the best of our knowledge, this is the first report of endoscopic closure for a spontaneous perforation of a PAD with IDP within a larger duodenal diverticulum. We performed an endoscopic procedure using APC to treat the friable margins and defect closure with an OTSC. To protect the papilla during endoscopic closure, we also placed plastic biliary and pancreatic stents to mark and retain the openings of the ductal orifices. This technique seems to be a promising salvage treatment of PAD perforation.
Although most PAD perforations are reported to occur during an endoscopic procedure, such as ERCP, spontaneous perforation can occur. Available treatment options previously described include surgical and conservative management for this potentially life-threatening complication. Within this case, we demonstrated the feasibility and efficacy of endoscopic closure of a spontaneous perforated PAD with IDP, which was concealed within a larger diverticulum. As such, endoscopic closure may be considered as a rescue treatment of PAD perforation.
DISCLOSURESAuthor contributions: S. Arayakarnkul made substantial contributions to the design and draft of the work, had final approval of the version to be published, and agreed to be accountable for all aspects of the work. E. Inal made substantial contributions to the draft of the work, had final approval of the version to be published, and agreed to be accountable for all aspects of the work. A. Mehta made substantial contributions to the acquisition of data for the work, reviewed the work critically for important intellectual content, had final approval of the version to be published, and agreed to be accountable for all aspects of the work. S. Ngamruengphong is the article guarantor and corresponding author, made substantial contribution to the conception and acquisition of data for the work, reviewed the work critically for important intellectual content, had final approval of the version to be published, and agreed to be accountable for all aspects of the work.
Financial disclosure: None to report. S. Ngamruengphong is a consultant for Boston Scientific Corporation, Olympus Medical Systems Corporation, Neptune Medical.
Informed consent was obtained for this case report.
REFERENCES 1. Wijarnpreecha K, Panjawatanan P, Manatsathit W, et al. Association between juxtapapillary duodenal diverticula and risk of choledocholithiasis: A systematic review and meta-analysis. J Gastrointest Surg. 2018;22(12):2167–76. 2. Teven CM, Grossman E, Roggin KK, Matthews JB. Surgical management of pancreaticobiliary disease associated with juxtapapillary duodenal diverticula: Case series and review of the literature. J Gastrointest Surg. 2012;16(7):1436–41. 3. Lin LW, Wu CC, Chong LW, Lin AC. Periampullary diverticulum perforation following endoscopic retrograde cholangiopancreatography (ERCP); a case report. Emerg (Tehran). 2015;3(2):78–80. 4. Miao YS, Li YY, Cheng BW, et al. Clinical analysis of 45 cases of perforation were identified during endoscopic retrograde cholangiopancreatography procedure. Front Med (Lausanne). 2022;9:1039954. 5. Mu P, Yue P, Li F, et al. Does periampullary diverticulum affect ERCP cannulation and post-procedure complications? An up-to-date meta-analysis. Turk J Gastroenterol. 2020;31(3):193–204.
留言 (0)