
記住我





Despite being the most common acquired idiopathic inflammatory myopathy, inclusion body myositis (IBM) remains a rare disorder affecting only 182 cases per million among adults older than 50 years.1 Symptoms typically present with insidious-onset weakness, which may be incorrectly labeled as age-related changes, leading to missed or delayed diagnosis, and therefore, a high index of suspicion is needed to make the diagnosis.2
Dysphagia, a common symptom of IBM, can be found in up to 33%–50% of patients.3 When compared with other inflammatory myopathies, the presence of dysphagia is associated with an increase in mortality because of respiratory failure or aspiration pneumonia.4 Gastroenterologists should be aware of this entity in the elderly population because early therapies can be offered to manage symptoms and prevent complications.
CASE REPORTA 57-year-old woman with a history significant for breast cancer and IBM presented with progressive dysphagia to solids and liquids localized to her throat with associated globus sensation and regurgitation. Three years earlier, our patient underwent esophagogastroduodenoscopy for evaluation of dysphagia, which was normal without features of eosinophilic esophagitis or stricture, and proton pump inhibitor therapy was initiated without improvement in symptoms. Further evaluation was deferred at that time because of a new diagnosis of breast cancer, but she subsequently returned with worsening dysphagia. During this period, she had notably been hospitalized for 2 episodes of aspiration pneumonia, which occurred after pill administration. On initial evaluation, her vitals were within normal limits, physical examination revealed moist mucus membranes, clear oropharynx, supple neck without masses, and cardiac auscultation regular without murmurs, and abdomen was soft with positive bowel sounds, nontender to palpation. Laboratory test results including complete blood count, comprehensive metabolic panel, and inflammatory markers were within normal limits.
Videofluoroscopic swallow study and timed barium esophagram were obtained for further evaluation. Barium esophagram (Figure 1) demonstrated rapid emptying of the esophagus; however, the swallow study exhibited a prominent cricopharyngeal (CP) bar, which prevented passage of a 13-mm barium pill and reproduced the patient's symptoms. Findings were consistent with severe CP dysfunction.
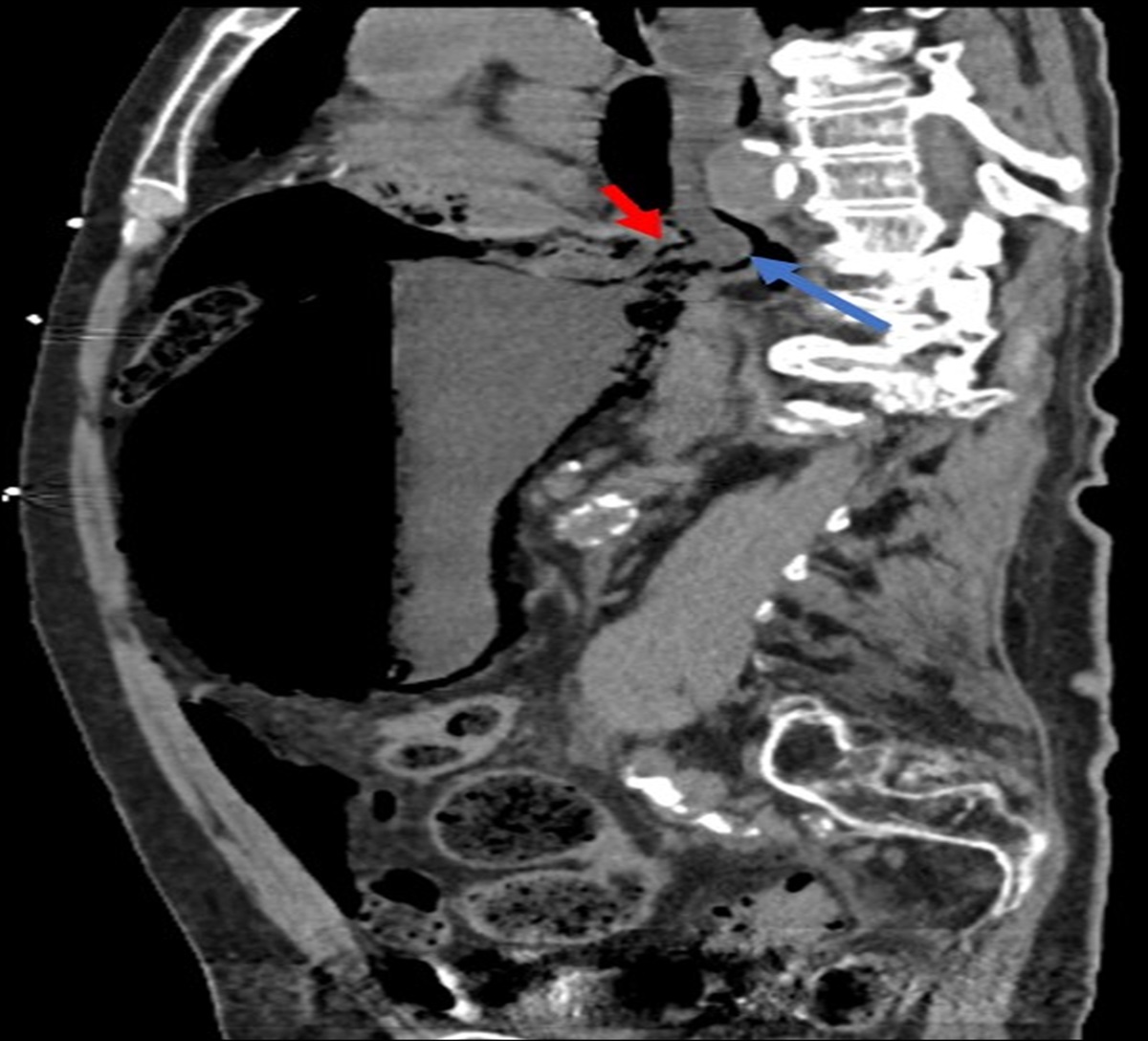
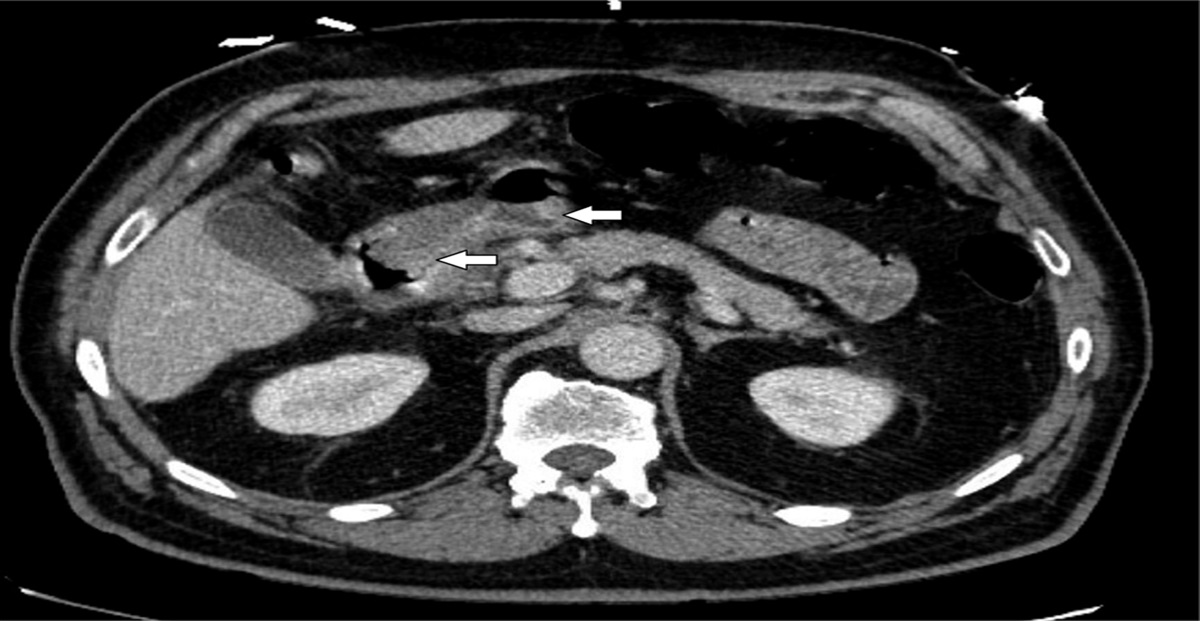
 Figure 1.:
Figure 1.: Barium esophagram swallow study. (A) Prominent cricopharyngeal bar (B) 13-mm barium pill stuck above cricopharyngeal muscle, preventing its passage.
The patient subsequently underwent uncomplicated endoscopic CP myotomy by otolaryngology. Biopsies demonstrated severe myopathy with fibrosis, rimmed vacuoles, and mitochondrial abnormalities consistent with IBM involvement of the cricopharyngeus muscle (Figure 2). Postoperatively, the patient's dysphagia markedly improved with increased ease of taking pills. Two years after endoscopic CP myotomy and speech therapy, our patient's dysphagia has improved with no further episodes of aspiration.
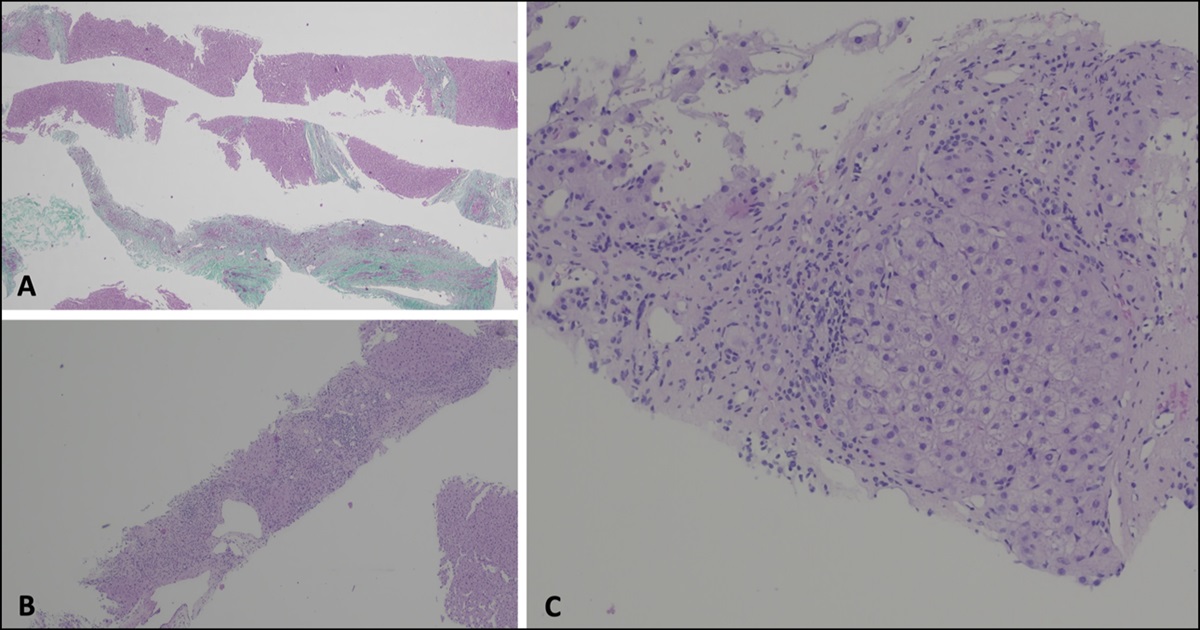
 Figure 2.:
Figure 2.: Biopsy from cricopharyngeal muscle. (A) (H&E stain, 400×) Fibers with vacuoles rimmed by basophilic material and inflammatory changes in endomysium, better appreciated in (B) (trichrome stain, black arrow). There is significant endomysial fibrosis (red arrow), consistent with a chronic, degenerative myopathic process.
DISCUSSIONIBM is described within the group of idiopathic inflammatory myopathies and is characterized by a slowly progressive disease presenting as insidious weakness with a predilection to the finger flexors, knee extensors, and muscles of the oropharynx.5 Muscle histopathology demonstrates inflammatory mononuclear cell infiltration of the endomysium, the presence of rimmed vacuoles within myofibers, and evidence of mitochondrial dysfunction.6 Interestingly, inflammatory myopathies are often associated with neoplasia, although the association between IBM and malignancy is unclear.7 Dysphagia is a common manifestation of IBM, and although most often viewed as a late complication, it may be the presenting symptom of the disease.8 Dysphagia may be underreported by patients, and early identification is important because aspiration pneumonia and respiratory failure are a leading cause of death among patients with IBM.9
Dysphagia in patients with IBM is often multifactorial, but a commonly recognized mechanism is CP dysfunction. Similar to other muscles in the body, the CP muscle undergoes chronic inflammation and subsequent scaring, leading to hypertrophy of the CP muscle and decreased compliance, also known as a cricopharyngeal bar (CPB).10 In fact, the presence of a CPB is a predictor for aspiration pneumonia in patients with IBM .11 Diagnosis of a CPB can be challenging and best identified with a videofluoroscopic swallow study.12
All patients with IBM and swallowing difficulties should be referred to speech pathology for evaluation and treatment. When a CPB is identified, treatment options include botulinum toxin injection, endoscopic dilation, or CP myotomy. Because of the rarity of the disease, treatment outcomes are limited to small case series. Botulinum toxin injection has been shown to improve symptoms and reduce the rates of aspiration; however, its use is limited by duration of action (typically less than 1 year) and need for repeated injections.12,13 Endoscopic dilation is a simple and minimally invasive option; however, less than one-third of patients undergoing dilation have symptomatic improvement.14 CP myotomy seems to be the most effective and durable treatment option to improve dysphagia symptoms. This procedure involves an incision of the CP muscle to permanently reduce resistance to bolus transit and is typically performed by otolaryngologists or gastroenterologists. Approximately 60% of patients respond to surgery.8,15,16 However, not all patients may be suitable candidates including those with significant oropharyngeal dysfunction or those with hiatal hernias.17,18
This case highlights the importance of recognizing cricopharyngeal dysfunction as a common cause of dysphagia in patients with IBM, a disease infrequently seen in gastroenterology clinic. Early identification and intervention can help improve patient symptoms and reduce the risk of aspiration. Cricopharyngeal myotomy seems to be the most established and effective treatment for suitable candidates.
DISCLOSURESAuthor contributions: OA Ramirez Ramirez was primarily responsible for case report design, data collection, and manuscript drafting and is the article guarantor. L. Hillman was responsible for study design/concept and manuscript revision.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
REFERENCES 1. Shelly S, Mielke MM, Mandrekar J, et al. Epidemiology and natural history of inclusion body myositis: A 40-year population-based study. Neurology 2021;96(21):e2653–61. 2. Goyal NA. Inclusion Body Myositis, 2022. 3. Wintzen AR, Bots GT, de Bakker HM, Hulshof JH, Padberg GW. Dysphagia in inclusion body myositis. J Neurol Neurosurg Psychiatry 1988;51(12):1542–5. 4. Naddaf E, Shelly S, Mandrekar J, et al. Survival and associated comorbidities in inclusion body myositis. Rheumatology (Oxford) 2022;61(5):2016–24. 5. Houser SM, Calabrese LH, Strome M. Dysphagia in patients with inclusion body myositis. Laryngoscope 1998;108(7):1001–5. 6. Dimachkie MM, Barohn RJ. Inclusion body myositis. Neurol Clin 2014;32(3):629–46, vii. 7. Damian L, Login CC, Solomon C, et al. Inclusion body myositis and neoplasia: A narrative review. Int J Mol Sci 2022;23(13):7358. 8. Oh TH, Brumfield KA, Hoskin TL, Kasperbauer JL, Basford JR. Dysphagia in inclusion body myositis: Clinical features, management, and clinical outcome. Am J Phys Med Rehabil 2008;87(11):883–9. 9. Price MA, Barghout V, Benveniste O, et al. Mortality and causes of death in patients with sporadic inclusion body myositis: Survey study based on the clinical experience of specialists in Australia, Europe and the USA. J Neuromuscul Dis 2016;3(1):67–75. 10. Naddaf E. Inclusion body myositis: Update on the diagnostic and therapeutic landscape. Front Neurol 2022;13:1020113. 11. Taira K, Yamamoto T, Mori-Yoshimura M, et al. Obstruction-related dysphagia in inclusion body myositis: Cricopharyngeal bar on videofluoroscopy indicates risk of aspiration. J Neurol Sci 2020;413:116764. 12. Schrey A, Airas L, Jokela M, Pulkkinen J. Botulinum toxin alleviates dysphagia of patients with inclusion body myositis. J Neurol Sci 2017;380:142–7. 13. Liu LW, Tarnopolsky M, Armstrong D. Injection of botulinum toxin A to the upper esophageal sphincter for oropharyngeal dysphagia in two patients with inclusion body myositis. Can J Gastroenterol 2004;18(6):397–9. 14. Shrivastava M, Harris C, Holmes S, Brady S, Winter S. Inclusion body myositis and dysphagia. Presentation, intervention and outcome at a swallowing clinic. J Laryngol Otol 2023;137(2):213–8. 15. McMillan RA, Bowen AJ, Bayan SL, Kasperbauer JL, Ekbom DC. Cricopharyngeal myotomy in inclusion body myositis: Comparison of endoscopic and Transcervical approaches. Laryngoscope 2021;131(8):131. 16. Poirier NC, Bonavina L, Taillefer R, Nosadini A, Peracchia A, Duranceau A. Cricopharyngeal myotomy for neurogenic oropharyngeal dysphagia. J Thorac Cardiovasc Surg 1997;113(2):233–40; discussion 240-1. 17. Langdon PC, Mulcahy K, Shepherd KL, Low VH, Mastaglia FL. Pharyngeal dysphagia in inflammatory muscle diseases resulting from impaired suprahyoid musculature. Dysphagia 2012;27(3):408–17. 18. Sanei-Moghaddam A, Kumar S, Jani P, Brierley C. Cricopharyngeal myotomy for cricopharyngeus stricture in an inclusion body myositis patient with hiatus hernia: A learning experience. Case Rep. 2013;2013:bcr2012008058.
留言 (0)