
記住我





Early gastric cancer (EGC) is defined as gastric cancer confined to the mucosa or submucosa, irrespective of lymph node metastasis.1 The prognosis for gastric cancer depends on its stage, so detection in the early stage of disease is important because curative removal is possible.2
Successful curative resection of a superficial lesion can only be achieved by precise characterization of the lesion. Endoscopic submucosal dissection (ESD) is a standard treatment of EGC.3 Postoperative results for EGC are excellent, with a 5-year survival ratio of over 90% in both Japan and Western countries.2 We report a case of EGC in which the absence of a nonextension sign was used, achieving en bloc R0 resection.
CASE REPORTA 64-year-old Costa Rican woman with hypertension, grade 2 obesity, and diabetes underwent screening endoscopy with diagnosis of high-grade dysplasia in random biopsies due to diffuse metaplasia during the endoscopic evaluation. She was referred to evaluate for endoscopic resection. At the time of the evaluation, a 30 mm elevated, Paris 0IIa + IIc lesion was identified at the antrum, with a demarcation line and irregular vascular and surface pattern (Figure 1), endoscopically consistent with malignancy. Owing to size and morphology, depth extension was unclear, for which the absence of the nonextension sign was used to decide for on-site ESD (Figure 1).
 Figure 1.:
Figure 1.: (A) Esophagogastroduodenoscopy shows an elevated (black arrows in A), 30 mm in diameter, Paris 0IIa + IIc lesion at the antrum, with a demarcation line and irregular vascular and surface pattern. (B) Same lesion with bioluminescent imaging shows the absence of a trapezoidal shape and clear flattening of the inspected lesion (black arrows in B) during gastric insufflation compatible with the absence of the nonextension sign.
Subsequently, the patient underwent an ESD, achieving en bloc resection (Figure 2). The biopsy specimen was sent for histopathology, which confirmed gastric adenocarcinoma pT1a with lamina propria and muscular mucosa invasion, but with tumor-free resection margins (Figure 3). During the postprocedural course, after 6 hours, the patient had hematemesis; an endoscopic evaluation identified upper gastric bleeding due to a spurting vessel located at the ulcer center. Endoscopic treatment using Coagrasper was achieved with successful hemostasia. The patient received esomeprazole 80 mg intravenously on the first day with subsequent doses of 40 mg every 12 hours for 5 days and also received sucralfate 1 oz 3 times a day per oral. The next day, a second-look endoscopy was performed and no lesions were observed. The patient was discharged home 5 days after the initial ESD procedure with omeprazole 20 mg every 12 hours per oral.
 Figure 2.:
Figure 2.: Endoscopic assessment after submucosal dissection in the antrum.
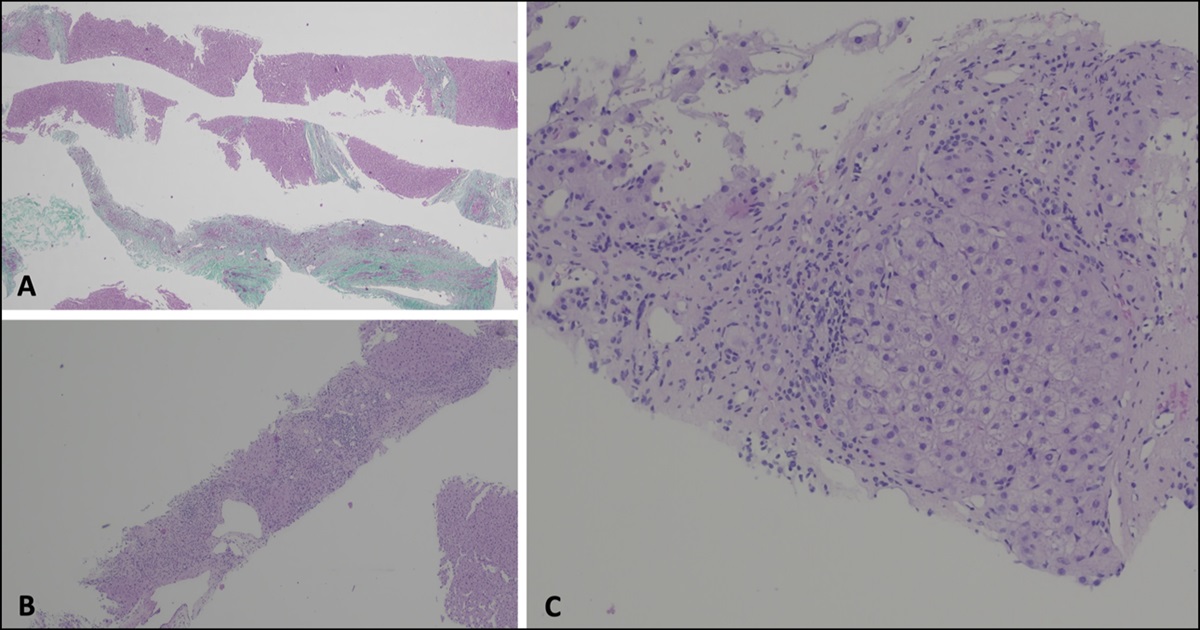
 Figure 3.:
Figure 3.: Histopathological examination (hematoxylin and eosin stain, 40×) reveals cellular atypia and dysplastic changes originating in glandular structures limited to the mucosa, compatible with early gastric adenocarcinoma pT1aNxMx.
DISCUSSIONEndoscopic diagnosis of EGC using conventional endoscopy is challenging because it often shows only subtle changes on endoscopic examination.4 To aid in the detection of suspicious EGC, 2 endoscopic criteria are a well-demarcated border and irregularity in color/surface pattern.4 The next step after diagnosis of EGC is determining the depth of invasion, which is important when considering therapeutic strategies.5
Some indicators that are considered useful in suggesting submucosal deep cancer include surface irregularities seen on gross examination of the tumor, depth of depressions, and tension.6
The nonextension sign requires adequate gastric distension and consists of a protrusion of the surrounding mucosa into the lumen, creating a trapezoidal shape in the gastric wall (Figure 4).7 This phenomenon occurs when massive submucosal invasion by a cancer increases the thickness and rigidity of the gastric wall and may be useful to differentiate between mucosal or microinvasive submucosal (SM1) and invasive submucosal (SM2) cancers.7
 Figure 4.: Type 0 – IIa + IIc lesion, 10 mm in diameter. (A) Visible trapezoid elevation. The tumor and normal mucosa around the tumor show trapezoid elevation (arrowheads). (B) Histological findings were well to moderately differentiated adenocarcinoma, pT1 (2,600 μm). Adapted from Hisabe et al.6 © 2018. This work is licensed under a CC-NC-ND License.
Figure 4.: Type 0 – IIa + IIc lesion, 10 mm in diameter. (A) Visible trapezoid elevation. The tumor and normal mucosa around the tumor show trapezoid elevation (arrowheads). (B) Histological findings were well to moderately differentiated adenocarcinoma, pT1 (2,600 μm). Adapted from Hisabe et al.6 © 2018. This work is licensed under a CC-NC-ND License.ESD was developed to make accurate en bloc resection possible.2 When submucosal invasion is superficial (<500 μm from the muscularis mucosae; T1b1), ESD is considered curative, whereas surgery is indicated for lesions with deep invasion of the submucosa (≥500 μm from the muscularis mucosae; T1b2).8
The absence of the nonextension sign has traditionally served as a valuable diagnostic tool in Eastern countries; however, its use in Western countries is not widespread, and its application in this population has been reported to be difficult to determine.8
In this case report, we demonstrate the usefulness of the absence of the conventional endoscopic nonextension sign as a marker to decide the adequate approach for mucosal lesions applied in Western population. As shown in Figure 1, the absence of a trapezoidal shape during gastric insufflation was useful to decide in favor of endoscopic submucosal resection, achieving en bloc resection (Figures 2 and 5), and was confirmed by histologic examination (Figure 3). Validation of the nonextension sign is necessary through prospective studies; however, we present a successful application in on-site decision making with a successful result.
 Figure 5.:
Figure 5.: Resected specimen stretched for histologic evaluation where a central irregular vascular and glandular pattern is clearly identified (white arrows), with flattening of the lesion on the examination pad.
DISCLOSURESAuthor contributions: JS Montero: conceptualization, investigation, supervision, writing—original draft and writing—review and editing. AC González: investigation, writing-original draft and writing—review and editing, and is the article guarantor. MA Salazar: supervision, writing—review, and editing. IC Soto: supervision, writing—review, and editing. AC Picado: supervision, writing—review, and editing.
Financial disclosure: None to report.
Informed patient consent was obtained for this case report.
REFERENCES 1. Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2021 (ver. 6). Gastric Cancer. 2023;26:1–25. 2. Yada T, Yokoi C, Uemura N. The current state of diagnosis and treatment for early gastric cancer. Diagn Ther Endosc. 2013;2013:241320. 3. Pimentel-Nunes P, Libânio D, Bastiaansen B, et al. Endoscopic submucosal dissection for superficial gastrointestinal lesions: European Society of Gastrointestinal Endoscopy (ESGE) guideline: Update 2022. Endoscopy. 2022;54(6):591–622. 4. Yao K. The endoscopic diagnosis of early gastric cancer. Ann Gastroenterol. 2013;26:11–22. 5. Takeda T, So S, Sakurai T, et al. Learning effect of diagnosing depth of invasion using non-extension sign in early gastric cancer. Digestion. 2020;101:191–7. 6. Hisabe T, Tsuda S, Hoaschi T, et al. Validity of conventional endoscopy using “non-extension sign” for optical diagnosis of colorectal deep submucosal invasive cancer. Endosc Int Open. 2018;6:E156–64. 7. Nagahama T, Yao K, Imamura K, et al. Diagnostic performance of conventional endoscopy in the identification of submucosal invasion by early gastric cancer: The ‘‘non-extension sign’’ as a simple diagnostic marker. Gastric Cancer. 2017;20:304–13. 8. Esposito G, Pimentel-Nunes P. Should we recommend use of non-extension sign in Europe? Endosc Int Open. 2019;7:E883–E884.
留言 (0)