
記住我





Drug-induced liver injury (DILI) is a common complication of oncologic medication.1,2 Many chemotherapeutic agents, targeted therapies, and, more recently, immunotherapy can contribute to DILI.3 Understanding the implications of hepatotoxicity in the context of potentially life-saving therapy is paramount when managing patients with malignancy.
Trials and case reports suggest that molecular targeted therapy, including tyrosine kinase inhibitor and BRAF kinase inhibitor, can result in DILI.4 Vascular endothelial growth factor (VEGF) inhibitors, known for their hepatotoxicity,5 carry a black box warning.4 However, given the rise of immunotherapy-induced drug injuries, the injury caused by VEGF inhibitors could be masked when coadministered with immunotherapies. The interplay between VEGF inhibitors and immunotherapies could further complicate the detection of DILI.6 Therefore, it is imperative to recognize and address the potential hepatotoxicity. We present axitinib-induced severe acute liver injury of a mixed hepatocellular and cholestatic pattern in a patient on pembrolizumab for metastatic renal cell carcinoma.
CASE REPORTThis is a 61-year-old man with a history of metastatic renal cell carcinoma with bone metastasis being treated with denosumab. The renal cell carcinoma was diagnosed 6 months before presentation, which led to a left nephrectomy.
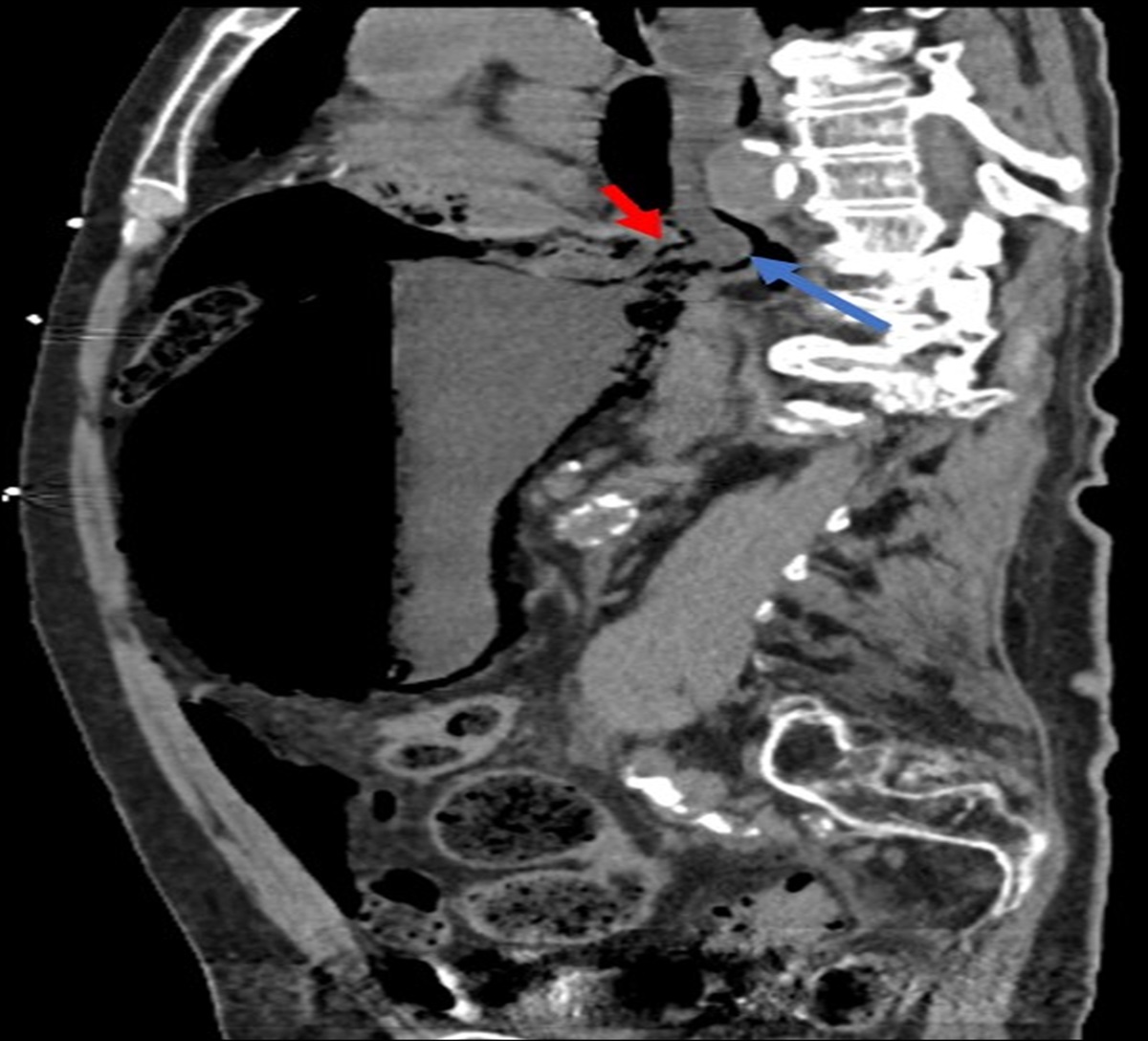
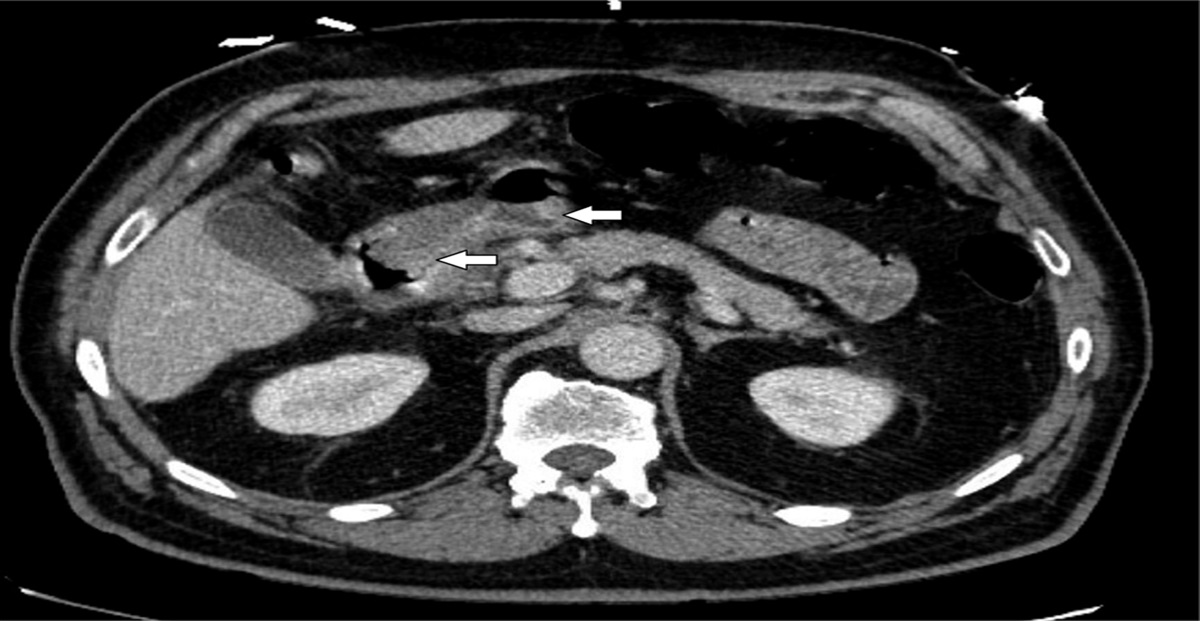
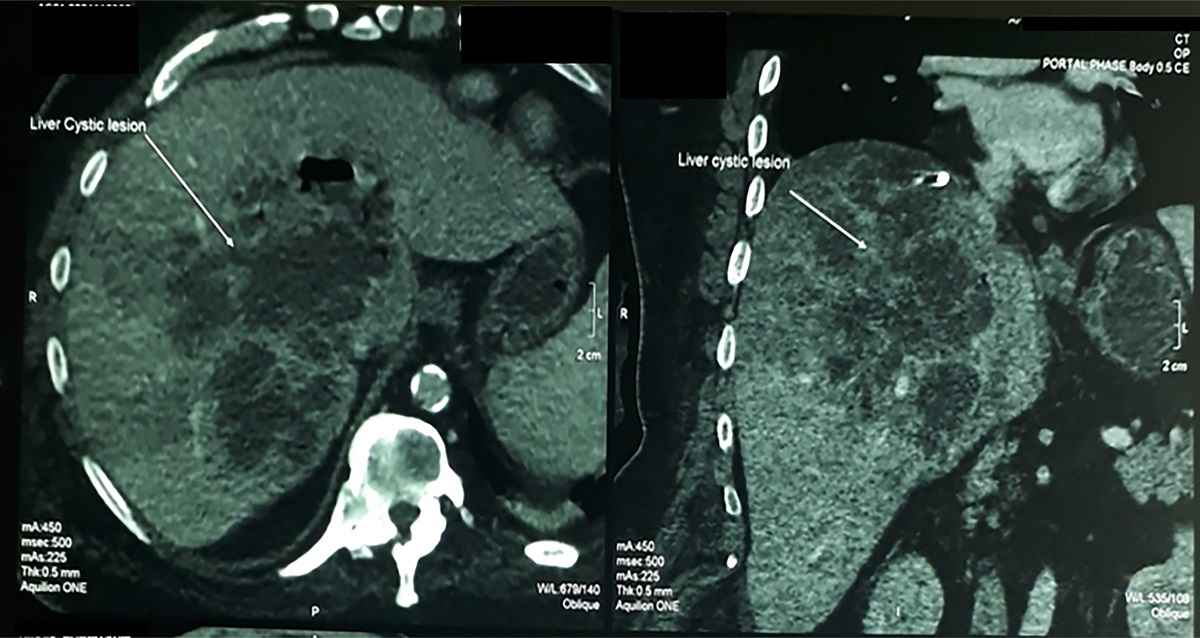
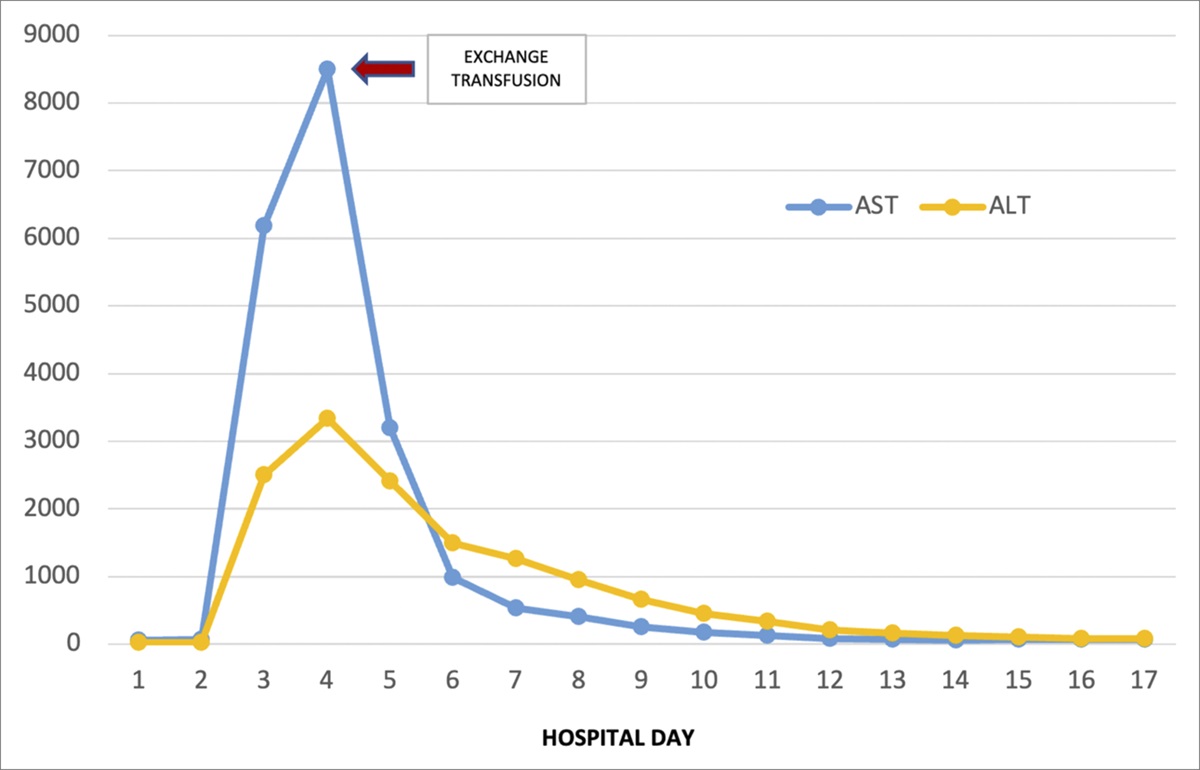
Two months after the nephrectomy, the patient commenced an immunotherapy/targeted therapy regimen of axitinib and pembrolizumab, alongside a course of radiation therapy, which concluded with 10 sessions. However, the patient's fourth cycle of immunotherapy/targeted therapy was interrupted 2 months after the initiation of the therapy because of elevated liver enzymes: alanine transaminase (ALT) 702 U/L, aspartate transaminase (AST) 306 U/L, and alkaline phosphatase (ALP) 308 U/L, all increased from their baseline normal range (Figure 1). The total bilirubin level was normal. The patient was without any discomfort or pain and denied any symptoms. He denied taking any new medications, nutrition supplements, or herbs. The workup for chronic liver disease (viral hepatitis, autoimmune, and hereditary liver diseases) did not reveal other potential etiologies of the elevated liver chemistries. Abdominal and pelvic computed tomography with contrast performed while he was on immunotherapy/targeted therapy showed only mild fatty infiltration in the liver. Owing to concern for possible checkpoint inhibitor hepatitis, pembrolizumab was held while axitinib was continued.
 Figure 1.:
Figure 1.: The trend of liver chemistries from before the use through after the discontinuation of axitinib. The pink shaded area denotes the period with pembrolizumab use. The blue shaded area denotes the period with axitinib use. Overlapped area denotes the use of both medications. ALT, alanine transaminase; AST, aspartate transaminase.
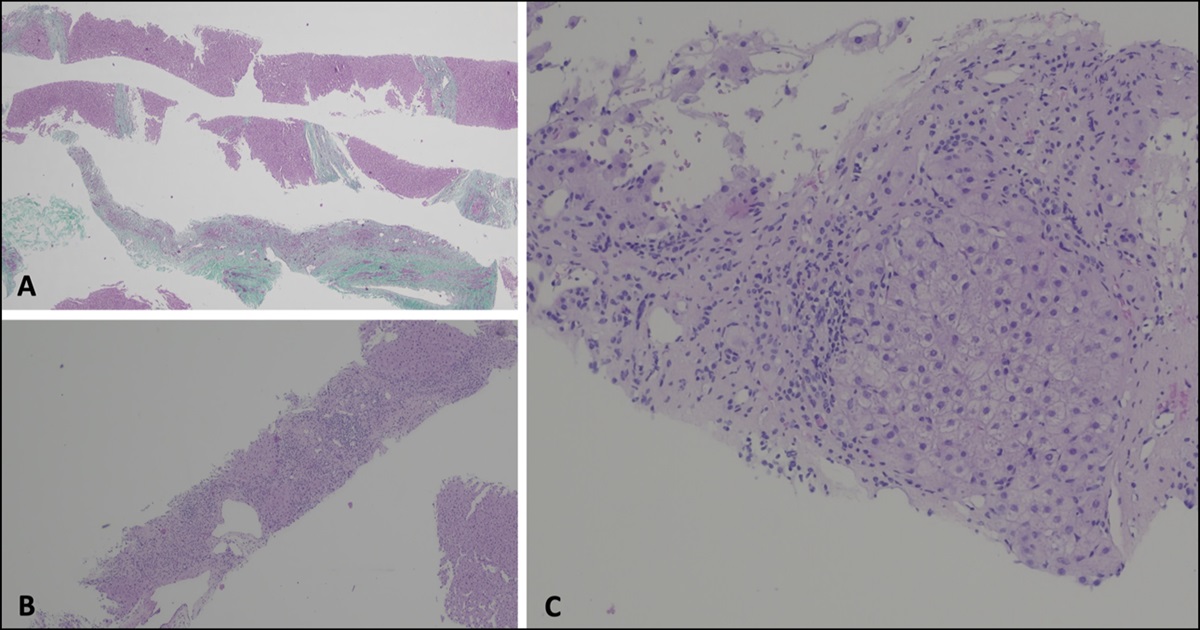
Subsequent laboratory results showed a persistent increase in liver chemistries, with AST, ALT, ALP, and total bilirubin surging to 416 U/L, 1233 U/L, 598 U/L, and 1.5 mg/dL, respectively, despite having stopped pembrolizumab (Figure 1). Axitinib was, therefore, also discontinued, followed by a notable improvement in liver enzymes, with AST, ALT, ALP, and total bilirubin decreasing to 222 U/L, 245 U/L, 64 U/L, and 0.8 mg/dL, respectively. Axitinib was eventually reintroduced while pembrolizumab remained on hold. Unfortunately, his liver enzymes subsequently rose again (AST 1180 U/L, ALT 2003 U/L, ALP 270 U/L, and total bilirubin 2.7 mg/dL). Given the severe liver injury, now with a cholestatic component, axitinib was again discontinued and the liver enzymes again normalized. During this period, there was no change in other medications. Liver biopsy was not performed because his liver chemistries worsened after rechallenging with axitinib and completely normalized after its discontinuation, making our diagnosis of axitinib-induced liver injury certain.
DISCUSSIONWe present a case with severe axitinib-related liver injury characterized by marked elevations of hepatocellular and cholestatic liver enzymes during initial treatment and rechallenge of axitinib with subsequent normalization of liver chemistries after the discontinuation of the medication. To our knowledge, this is the first case report of severe acute liver injury from axitinib with cholestatic hepatitis. Understanding its risk profile, particularly while taking concurrent immunotherapy, is paramount in the overall management of those with malignancy. In our case, discontinuing the immunotherapy, pembrolizumab did not affect the level of his liver chemistries, pointing toward axitinib as the primary causative agent. This case underscores the complexities of managing oncological therapy-related liver injuries, highlighting the need for meticulous monitoring and proactive management to achieve early recognition, prevent irreversible hepatic damage, and optimize patient outcomes.
Axitinib, a selective inhibitor of the VEGFR,7 showed in a phase III trial the most common grade ≥3 adverse events were hypertension, diarrhea, and fatigue; 32% had elevated thyroid-stimulating hormone, necessitating thyroid hormone management.8 A phase 1b trial with axitinib and pembrolizumab reported relatively mild elevations in liver enzymes (AST and ALT)9 while the proportion of grade 3 or 4 liver enzyme elevation was higher in the KEYNOTE-426 trials, which used pembrolizumab and axitinib as the first-line treatment in patients with advanced renal cell carcinoma.10 Currently, axitinib is categorized as a suspected, but unproven, hepatotoxic agent according to the LiverTox website.11 This is the first case report that showed a grade 4 liver enzyme elevation (AST and ALT >10.0 times upper limit of normal [ULN]) after axitinib administration. In addition, the liver injury after the rechallenge of axitinib, in this case, has met the Hy law criterion, which is defined as concurrent elevations of ALT (>3× ULN) and total bilirubin (>2× ULN) without initial evidence of cholestasis. The Hy law is a sensitive and specific predictor for a medication to trigger severe hepatotoxicity12 and potentially indicates a need for liver transplantation in 10% of such cases.13 Notably, according to the previous consensus, both pembrolizumab and axitinib should be discontinued permanently when a grade 4 hepatotoxicity is found.14
VEGF is involved in numerous physiological processes, including endothelial cell growth and migration.15,16 Hepatotoxicity triggered by VEGF inhibitors is suspected to result from direct and/or indirect hepatotoxicity.17 Direct hepatotoxicity might arise from either the formation of a reactive metabolite or unintended multikinase inhibition, which could perturb various hepatocellular processes and lead to cell death.18 Indirect hepatotoxicity could ensue from the disruption of sinusoidal blood vessels' structure and function. A previous study reported hepatotoxicity secondary to the use of pazopanib in patients with renal cell carcinoma.19 A meta-analysis of genome-wide association studies suggested an increased risk of liver enzyme elevations in pazopanib-treated patients carrying the HLA-B*57:01 allele.20
In conclusion, we demonstrate a case with severe mixed hepatocellular and cholestatic DILI conforming to the Hy law, as evidenced by clinical improvement after axitinib discontinuation and exacerbated liver injury upon readministration. Physicians using axitinib should be aware of its potential for severe hepatotoxicity and remain cautious when using it combined with immunotherapy. Further studies are warranted to elucidate optimal management strategies and preventive measures.
DISCLOSURESAuthor contributions: YH Yeo wrote the manuscript. W. Ayoub, JD Yang, and A. Kuo revised the manuscript. HD Trivedi revised the manuscript and is the article guarantor.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
REFERENCES 1. Low EXS, Zheng Q, Chan E, Lim SG. Drug induced liver injury: East versus West: A systematic review and meta-analysis. Clin Mol Hepatol. 2020;26(2):142–54. 2. Mondaca SP, Liu D, Flynn JR, et al. Clinical implications of drug-induced liver injury in early-phase oncology clinical trials. Cancer. 2020;126(22):4967–74. 3. Remash D, Prince DS, McKenzie C, Strasser SI, Kao S, Liu K. Immune checkpoint inhibitor-related hepatotoxicity: A review. World J Gastroenterol. 2021;27(32):5376–91. 4. Shah RR, Morganroth J, Shah DR. Hepatotoxicity of tyrosine kinase inhibitors: Clinical and regulatory perspectives. Drug Saf. 2013;36(7):491–503. 5. Powles T, Bracarda S, Chen M, et al. Characterisation of liver chemistry abnormalities associated with pazopanib monotherapy: A systematic review and meta-analysis of clinical trials in advanced cancer patients. Eur J Cancer. 2015;51(10):1293–302. 6. Donahower B, McCullough SS, Kurten R, et al. Vascular endothelial growth factor and hepatocyte regeneration in acetaminophen toxicity. Am J Physiol Gastrointest Liver Physiol. 2006;291(1):G102–9. 7. Kelly RJ, Rixe O. Axitinib: A selective inhibitor of the vascular endothelial growth factor (VEGF) receptor. Target Oncol. 2009;4(4):297–305. 8. Rini BI, Escudier B, Tomczak P, et al. Comparative effectiveness of axitinib versus sorafenib in advanced renal cell carcinoma (AXIS): A randomised phase 3 trial. Lancet. 2011;378(9807):1931–9. 9. Atkins MB, Plimack ER, Puzanov I, et al. Axitinib in combination with pembrolizumab in patients with advanced renal cell cancer: A non-randomised, open-label, dose-finding, and dose-expansion phase 1b trial. Lancet Oncol. 2018;19(3):405–15. 10. Rini BI, Atkins MB, Plimack ER, et al. Characterization and management of treatment-emergent hepatic toxicity in patients with advanced renal cell carcinoma receiving first-line pembrolizumab plus axitinib. Results from the KEYNOTE-426 trial. Eur Urol Oncol. 2022;5(2):225–34. 11. LiverTox: Clinical and Research Information on Drug-Induced Liver Injury. National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, 2012. 12. Temple R. Hy's law: Predicting serious hepatotoxicity. Pharmacoepidemiol Drug Saf. 2006;15(4):241–3. 13. Andrade RJ, Lucena MI, Fernández MC, et al. Drug-induced liver injury: An analysis of 461 incidences submitted to the Spanish registry over a 10-year period. Gastroenterology. 2005;129(2):512–21. 14. Grunwald V, Voss MH, Rini BI, et al. Axitinib plus immune checkpoint inhibitor: Evidence- and expert-based consensus recommendation for treatment optimisation and management of related adverse events. Br J Cancer. 2020;123(6):898–904. 15. Taniguchi E, Sakisaka S, Matsuo K, Tanikawa K, Sata M. Expression and role of vascular endothelial growth factor in liver regeneration after partial hepatectomy in rats. J Histochem Cytochem. 2001;49(1):121–30. 16. Walter TJ, Cast AE, Huppert KA, Huppert SS. Epithelial VEGF signaling is required in the mouse liver for proper sinusoid endothelial cell identity and hepatocyte zonation in vivo. Am J Physiol Gastrointest Liver Physiol. 2014;306(10):G849–62. 17. Schmidinger M. Understanding and managing toxicities of vascular endothelial growth factor (VEGF) inhibitors. EJC Suppl. 2013;11(2):172–91. 18. Teo YL, Ho HK, Chan A. Formation of reactive metabolites and management of tyrosine kinase inhibitor-induced hepatotoxicity: A literature review. Expert Opin Drug Metab Toxicol. 2015;11(2):231–42. 19. Shantakumar S, Nordstrom BL, Djousse L, et al. Occurrence of hepatotoxicity with pazopanib and other anti-VEGF treatments for renal cell carcinoma: An observational study utilizing a distributed database network. Cancer Chemother Pharmacol. 2016;78(3):559–66. 20. Xu CF, Johnson T, Wang X, et al. HLA-B*57:01 confers susceptibility to pazopanib-associated liver injury in patients with cancer. Clin Cancer Res. 2016;22(6):1371–7.
留言 (0)