
記住我
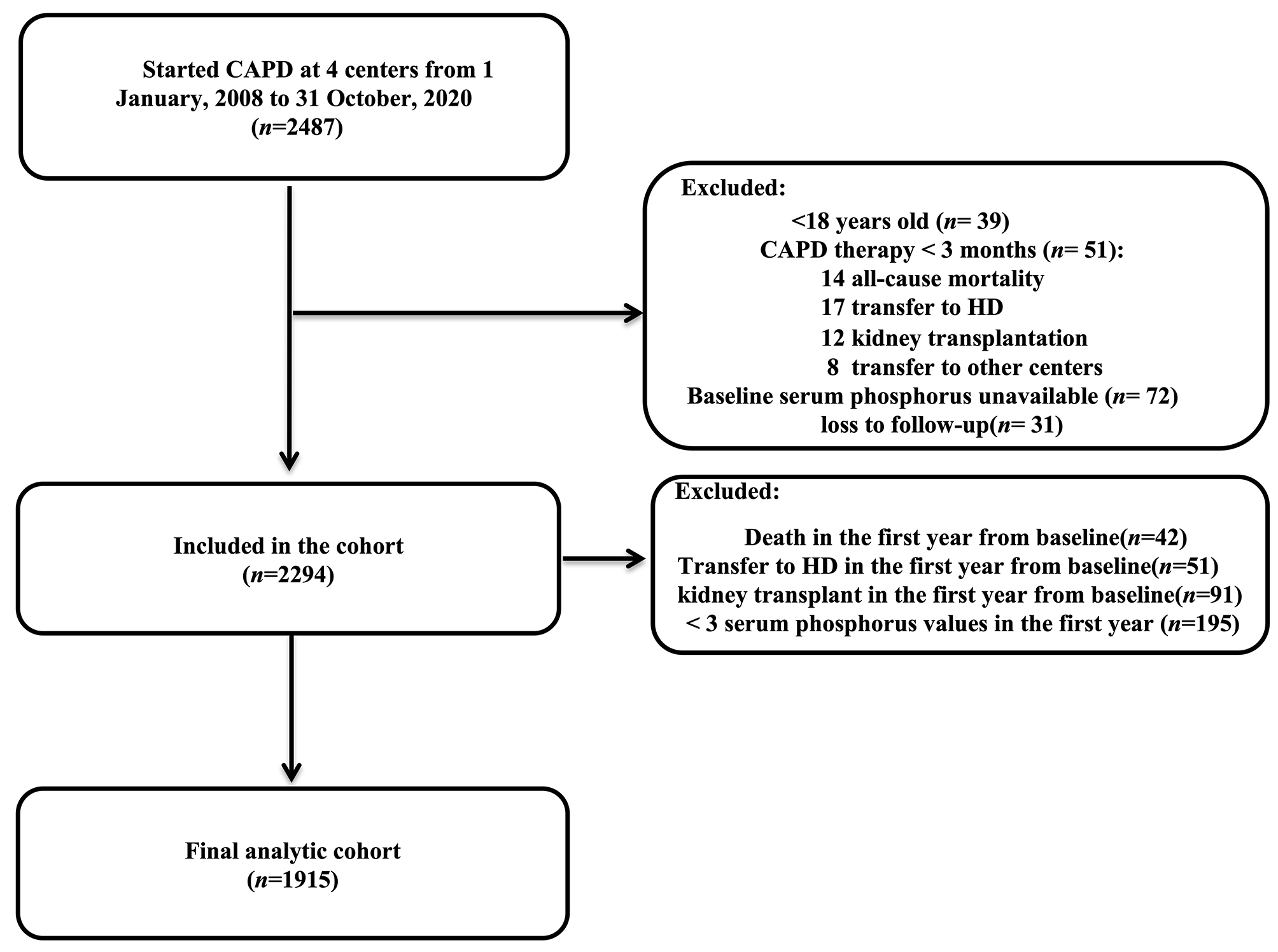





The 2018 PMSI database contains 26,917,832 stays, of which 9,458,453 (35.1%) were admissions for specific procedures and health care (including radiotherapy and chemotherapy sessions, rehabilitation, and dialysis sessions). All of these PMSI stays were included in the main analysis and a code for AKI was present in 415,067 stays (1.54%). An explicit code for sepsis was present in 421,543 (1.6%) stays, a code for CVEC in 40,084 (0.1%) stays, and a code for MOV in 166,831 (0.6%) stays. An AKI code was associated with 83,553 (19.8%), 7,165 (17.9%), and 15,387 (9.2%) of the sepsis, CVEC, and MOV stays respectively. The study population flow-chart is reported in Fig. 1.
Fig. 1
Study flow chart: In the matched populations, cases (AKI stays) and controls (no-AKI stays) were paired based on age class, sex, area of residence, hospital type (public/private), presence of a sepsis (in the surgical subgroups), presence of a surgery (in the sepsis subgroup). AKI Acute kidney injury, CVEC Cardiovascular surgery with extracorporeal circulation, MOV Major open visceral surgery, PMSI Programme de Médicalisation des Supports d’Information
Characteristics of AKI and no-AKI staysPublic hospitals accounted for 67.7% of the total stays in 2018 (n = 18,212,482), and 87.7% of the AKI stays (n = 363,988). When compared to no-AKI stays, AKI stays concerned more often male patients (n = 235,554, 56.8% vs. n = 12,657,336, 47.8%) and older patients (mean [SD] age 74.2[16.4] vs. 55.8[23.9]). AKI stays were mainly admitted from the ER (n = 227,377, 54.8%), whereas no-AKI stays were mainly admitted from home (n = 21,580,666, 81.4%). Discharge was more frequent to home for no-AKI stays (n = 24,726,121, 93.3%) than for AKI stays (n = 238,392, 57.4%). Death occurred in 59,338 patients with AKI during their hospital stay (14.3%) and in 237,673 patients without AKI (0.9%; Table 1). The most common DRG in AKI stays were “heart and heart valves diseases, with complications” (n = 31,389, 7.6%), “respiratory tract infections, with complications” (n = 27,994, 6.7%) and “other kidney and urinary tract diseases, with complications” (n = 24,653, 5.9%).
Table 1 Characteristics of the populationSurgical stays (CVEC and MOV) with AKI required more often RRT than stays with sepsis and AKI (CVEC: n = 2,121, 29.6%; MOV: n = 4,013, 26.1%; sepsis: n = 14.522, 17.4%). However, death occurred more frequently in the sepsis and AKI stays than in the surgery and AKI stays (sepsis: n = 24,672, 29.5%; MOV: n = 3,870, 25.2%; CVEC: n = 1,196, 16.7%). The characteristics for each subgroup of stays are presented in the Supplementary Table 2.
Costs and lengths of stay in the whole populationThe total cost of stay and its main components are shown in Table 2 for the whole PMSI population and subpopulations. AKI stays were associated with higher costs than no-AKI stays (median [IQR] €4,719.9 [2,963.6–7781.8] vs €735.5 [382.8–1805.4]). Patients with AKI required more medical procedures (such as mechanical ventilation, vasopressor infusion and oxygen delivery) than those without AKI (Table 1). Among stays with AKI, 9.7% (n = 40,436) required RRT during their stay and 17.2% (n = 71,277) had at least one admission to the ICU whereas only 0.8% (n = 208,265) of those without AKI were admitted to the ICU. The additional cost of an ICU stay was higher for AKI-stays compare to no-AKI stays (median [IQR] €4,024 [€1,608—€8,844] vs. €1,608 [€0- €4,824]).
Table 2 Cost of stay (in euros) in different populationsStays with AKI were longer (median [IQR] 9 [4-16] days vs. 0 [0–2] days); 56% (n = 232,368) of the AKI stays lasted > 8 days whereas 75.7% (n = 20,065,935) of the no-AKI stays lasted < 2 days and 8.2% (n = 2,161,042) lasted > 8 days.
Increase in costs and LOS associated with AKI in the matched subgroupsThe case–control study included 82,312 AKI stays with sepsis, 6,659 AKI stays with CVEC, and 15,239 AKI stays with MOV. The pairing ratio was 1:2 in the sepsis group and 1:1 in the surgical groups. As decided a priori, analyses were adjusted based on the presence of chronic kidney disease, diabetes, and cardiac failure.
In the sepsis group, compared to the matched no-AKI stays, the presence of AKI increased the hospital cost by 1.70 times (95%CI [1.69; 1.72]; crude median cost of stay [IQR] €8.274,0 [4.769,0–17.076,4] for stays with AKI vs. €5.988,5 [3.522,3–9.688,7] for matched stays with no AKI, p < 0.0001) and the LOS by 1.33 times (95%CI [1.32; 1.34]; crude median LOS [IQR] 13 [7-25] days for stays with AKI vs. 10 [5-18] days for matched stays with no AKI, p < 0.0001). In the CVEC group, the presence of AKI increased the hospital cost by 1.48 times (95%CI [1.45; 1.50]; crude median cost of stay [IQR] €25,024 [18,898.2 – 35,476.9] for stays with AKI vs. €18,034.6 [14,500.5 -23,033.2] for matched stays with no AKI, p < 0.0001) and the LOS by 1.47 times (95%CI [1.44; 1.51]; crude median LOS [IQR] 16 [11 – 29] days for stays with AKI vs. 11 [9-17] days for matched stays with no AKI, p < 0.0001). In the MOV group, the presence of AKI increased the hospital cost by 1.68 times (95%CI [1.65; 1.70]; crude median cost of stay [IQR] €18,587.8 [11,411.9 – 29,546.4] for stays with AKI vs. €11,292.6 [7.534,7 -17.661,2] for matched stays with no AKI, p < 0.0001) and the LOS by 1.41 times (95%CI [1.38; 1.44]; crude median LOS [IQR] 19 [11 – 36] days for stays with AKI vs. 13 [6-23] days for matched stays with no AKI, p < 0.0001; Fig. 2).
Fig. 2
Median length of stays and costs with interquartile range in the whole PMSI population and the matched populations for each subgroup. A length of stay in days, median with interquartile range. B total hospital cost of stay in euros, median with interquartile range. p < 0.0001 for all comparisons between AKI and no-AKI stays in the matched populations, Wilcoxon tests CVEC Cardiovascular surgery with extracorporeal circulation, MOV Major open visceral surgery
留言 (0)