Four hundred and fifty-nine children were enrolled in the study. They included 276 boys and 183 girls. They had a mean age of 63.94 ± 20.62 days and were followed for a median time of 58 (1–191) months. Table 1 demonstrates the clinical, laboratory, and histologic features of all cases.
Clinically confirmed BA versus non-BA cases
We documented 162 (35.3%) cases of BA out of all 459 enrolled cases (Table 2). It was noted that with increasing patient age, the GGT level increased in the BA group (from 474 to 754 IU/L) compared to the decrease in the non-BA group (from 121 to 67 IU/L).
Table 2 Demographic, clinical, laboratory, and histopathologic features of BA and non-BA groupsAt the histopathologic level, most of the BA cases showed bridging fibrosis (79.1 %) and moderate to marked bile ductular proliferation (68.5%) (P < .001). However, bile ductular proliferation was present to a variable degree in 46.5% of non-BA cases.
One hundred fifty-four cases out of 162 BA cases (95.1%) were clearly suggested on histopathologic examination, while the remaining 8 cases were missed as other diagnoses (7 cases with neonatal hepatitis pattern and one as paucity of intrahepatic bile duct). The mean age of the missing 8 cases was 29.75 (28–32) days. They were all presented with a clay stool with a median GGT level of 443 IU/L (IQR 301.75–643.25). On histopathologic examination, 50% showed mild portal fibrosis and mild diffuse bile ductular proliferation in 5 cases (62.5%). On the other hand, those diagnosed as obstructive cholestasis (179) by histopathologic examination included 154 cases confirmed to be BA, 3 cases of choledochal cyst, 10 cases of PFIC-3, 7 cases as Alagille syndrome (paucity), and 5 metabolic causes including alpha-1 antitrypsin deficiency. The non-BA cases misdiagnosed histologically as obstructive cholestasis did not experience any unnecessary surgical intervention.
Kasai procedure
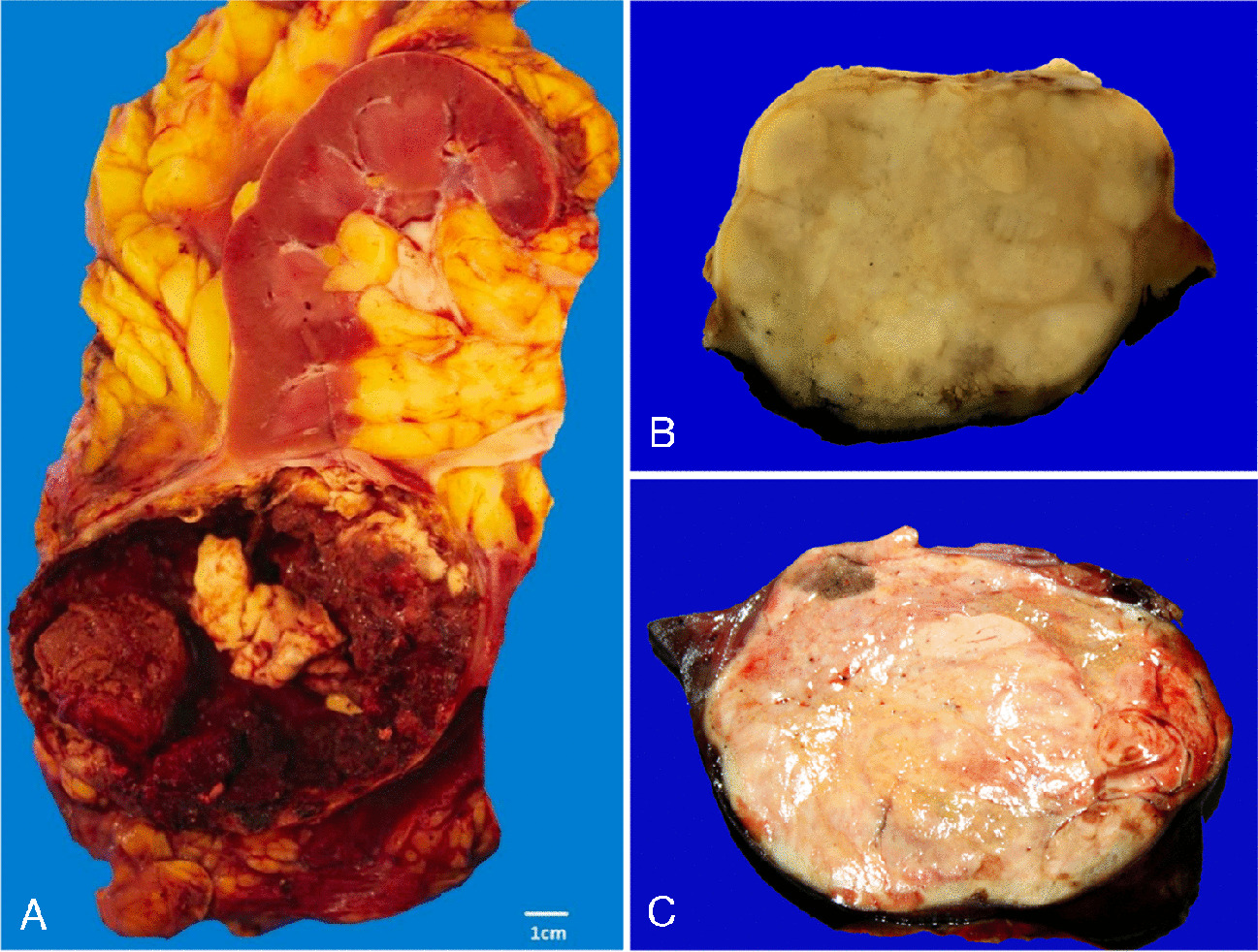
At a mean age of 75.46 months, 142 BA group cases (87.7%) underwent Kasai surgery. An intraoperative cholangiogram was performed for all patients. The excised atretic segment was received and labelled, and the diameter of the bile ductule was measured using a DP50 camera (Olympus, Tokyo, Japan) equipped with an Olympus BX31 microscope. Only 28 operated cases (19.7%) developed hepatic encephalopathy. Those who did not have a Kasai procedure (20 cases) included 11 cases presented late with advanced fibrosis, as well as 9 cases where the parents refused to have surgery due to their belief that natural herbs would solve the problem.
Because the patient’s age is critical for the Kasai procedure [10], we divided all 162 clinically proven BA cases into two groups according to age (≤ 6 weeks and > 6 weeks, Supp Table 5). Histopathologic features of obstruction such as portal edema, advanced portal fibrosis, and bile ductular proliferation were more common in infants > 6 weeks of age (P < .001).
Concordance of liver biopsy with final diagnosis
When studying the histopathologic concordance with the clinical diagnosis of BA, a liver biopsy assessed using the strict histopathologic criteria (Table 1) did perform well, with a sensitivity of 95.1%, specificity of 91.6%, PPV of 86%, and NPV of 97.1%. Concordance between the histopathologic and the clinical diagnosis of BA was 0.846 (perfect agreement).
Univariate and multivariate analysis of features associated with BA
The histopathologic predictors of BA identified by univariate analysis (Table 3) included portal edema, moderate and advanced portal fibrosis, ductular proliferation (mild diffuse or moderate/marked), bile duct/ductular plugs, DPM-like pattern, and cholangiolitis in addition to the absence of EMH or giant cell transformation of hepatocytes. Only portal edema, ductular proliferation (mild diffuse or moderate/marked), bile duct/ductular plugs, and cholangiolitis are the histopathologic predictors of BA according to multivariate analysis (Table 3).
Table 3 Univariate and multivariate analysis of histopathologic features associated with biliary atresiaDesign of the diagnostic score for BA
There is no single diagnostic procedure that appears to be clearly superior for diagnosis of BA, rather a few diagnostic tools are used collectively to reach an early and accurate diagnosis. BA can only be correctly diagnosed by correlating the clinico-radiological features with histological findings [13]. In this study, all patients underwent an abdominal ultrasound, which gave a detailed report about the gall bladder length, contractility, triangular cord sign, and extra and intrahepatic biliary radicles with a clear comment on any abnormality as if the gallbladder (non-contractile or rudimentary or non-visualized). When radiology was non-conclusive or negative and the liver biopsy showed a picture of obstructive cholestasis, hepatobiliary scans (HIDA showing no excretion of radiotracer) and intraoperative cholangiogram were done to reach a definite diagnosis.
Serum levels of GGT are not required, but their high elevation (10 times normal) supports the diagnosis. Patient age was taken into consideration when assessing both the liver biopsy pathologically and the level of GGT. The AUC of serum GGT levels in relation to age group was 0.812 in neonate ≤ 60 days, 0.868 in infants aged 61–90 days, and 0.940 in those aged 91–120 days (Supp Figure 2). The cutoff of GGT in patients with BA ≤ 60 days was 309.5 IU/L with 82.4% sensitivity and 72.7% specificity. The cutoff increased to 347.5 IU/L with increasing age (61–90 days) with 88.6% sensitivity and 80.6% specificity. Despite that the cutoff value of GGT decreased to 295 IU/L at age (91–120 days), its sensitivity and specificity increased to 93.3% and 83.9%, respectively.
When all histopathologic features of obstruction are diffusely present (> 50% of portal tracts), a total score of 2 is given regardless of patient age. When some of these features are present or when all features are detected focally (< 50% of portal tracts), then referral to patient age is essential for scoring (Table 4).
Table 4 The diagnostic scoring system for biliary atresiaWe assigned points to each of the 4 aforementioned parameters (Table 4). This score was then validated across all cases in the study (BA and non-BA cases). We found a sensitivity of 100% and a specificity of 93.3% at a cutoff of 3, 100% sensitivity and 100% specificity at a cutoff of 4, 95.1% sensitivity and 100% specificity at a cutoff of 5, and 78.4% sensitivity and 100% specificity at a cutoff of 6 points.
Since patient’s age can affect the histopathologic features of BA, we investigated all the study cases aged less than 6 weeks to evaluate how the diagnostic score will perform. Only 3 cases out of 19 cases of Paucity/Allagille and 2 cases of PFIC-3 got a score of 3, while 8 (30.8%) out of 26 cases of BA got a score of 4. When the total score is equivocal for BA, proceeding with an intraoperative cholangiogram may be the most effective and quick strategy to avoid the drawbacks of a delayed BA diagnosis, such as a delayed Kasai surgery and the higher possibility of a liver transplant.


留言 (0)