
記住我
This trial-based CUA is reported according to the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) [10]. The CHEERS 2022 checklist is included in the Electronic Supplementary Material (ESM). We used an intention-to-treat approach employing data collected during the IMMENSE study and health register data for the included patients. Previous publications from the IMMENSE study include the study protocol [11], the effectiveness evaluation for the primary and secondary outcomes [9], and an intervention fidelity analysis [12].
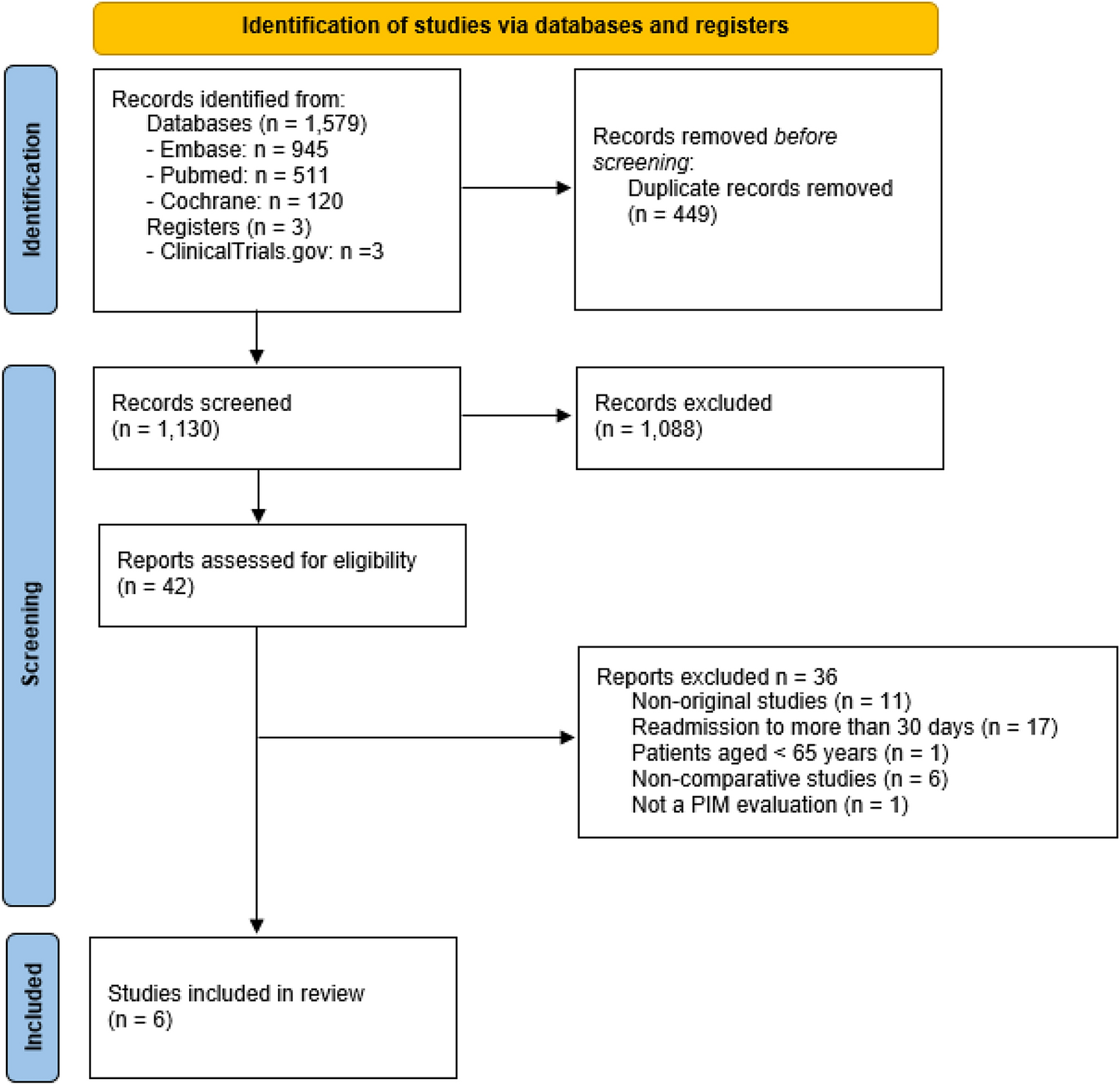
2.1 Study Design and Study PopulationPatients were recruited from September 2016 to December 2019 at two internal medicine wards at the University Hospital of North Norway: one geriatric ward (Ward 1) and one general medicine ward (Ward 2). Patients aged ≥ 70 years acutely admitted to the wards and willing to provide written informed consent (patient or next of kin) were randomized into two groups (1:1). The intervention group received the intervention in addition to standard care, and the control group received standard care only. Follow-up time was 12 months after discharge. According to the study protocol, patients for whom the next of kin provided informed consent were excluded from HRQoL measurements [11]. We have included 285 patients (intervention group, n = 148 and control group, n = 137) of the 480 IMMENSE trial population who were eligible for HRQoL and provided one or more such measurements in the CUA (Fig. 1).
Fig. 1
Study flowchart showing the EuroQol 5-dimension 3-level questionnaire (EQ-5D-3L) completed or not completed at discharge, 1 month, 6 months, and 12 months in the study follow-up period. CUA cost-utility analysis
2.2 The InterventionThe intervention in the IMMENSE study comprised five steps: (i) medication reconciliation at admission; (ii) medication review during the hospital stay; (iii) patient counseling about the use of medicines; (iv) comprehensible and patient-friendly dissemination of the medication list with explanations in discharge summary; and (v) post-discharge phone call to the primary care provider (regular general practitioner or nursing home physician/nurse). The first four steps were completed during the index hospital stay. The fifth step was completed shortly after discharge, aiming to improve the communication of recommendations across care levels.
2.3 Health-Related Quality of LifeHealth-related quality of life was measured using the EuroQol 5-Dimension 3-Level Health State Questionnaire (EQ-5D-3L) [13]. The five dimensions of the questionnaire are mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension has three possible response levels, namely no problems, moderate problems, or severe problems. A trained study nurse blinded to the study group allocation collected the EQ-5D-3L data at the time of discharge from the index hospital stay and at 1, 6, and 12 months after discharge. The data collection was performed face-to-face with the participants at discharge in Ward 1, while all remaining collections were completed over the phone. We used the three-level version because of cognitive consideration and practicalities (i.e., time to administer the questionnaire).
As recommended by Norwegian authorities owing to a lack of Norwegian tariffs [14], utility values were derived using the UK time-trade-off societal value set, translating the EQ-5D-3L responses for each collection time to a utility value between one for perfect health, zero for death, or below zero for conditions worse than death [15]. This was completed starting with a utility of 1 and subtracting according to the algorithm for each reported problem in each of the five dimensions [15]. Quality-adjusted life years (QALYs) were calculated for each respondent for the 12-month follow-up as the area under the curve combining the utility value for each collection time, assuming a linear change between each timepoint. Because of the acute care setting, the first measurement was performed at discharge after the intervention had been initiated and we consequently did not have a baseline measurement available. However, assuming a common fixed baseline is considered to ensure a minimal bias to the QALY estimation when the first measurement is taken close to the time of baseline and in a series of measurements over a 12-month follow-up [16]. We therefore assumed a baseline utility score for all patients equal to the mean discharge utility for the control group. Patients who died during the follow-up were assigned a utility value of 0 at the collection times following their death. Missing utility values for any collection times were 9.1% and were assumed to be missing at random.
2.4 Healthcare Resource Use and CostsIndividual-level resource use and costs were obtained from administrative registers and linked with other trial data using the unique national identity numbers [17]. Hospital resource-use data (index stay and readmissions, inpatient and outpatient hospital care) were obtained from the hospital’s administrative Cost Per Patient register, an activity-based costing register with patient-level costs per episode. Primary care resource-use data (general practitioner, specialist physician, and emergency room visits) were obtained from the Norwegian Control and Payment of Health Reimbursements Database (KUHR), a national administrative database with patient-level costs per episode for all primary healthcare, including patient contributions and healthcare provider reimbursements from the state for treatment and material costs. All costs covered the time horizon from 12 months before inclusion in the study until 12 months after discharge from the index hospitalization. A health provider perspective was taken, including costs of health service use during the trial period. Costs were transformed to 2021 values using the Norwegian inflation index for health [18] and translated to Euros (€) using the 2021 exchange rate (€1 = NOK 10.16) [19].
The intervention cost was estimated based on mean pharmacist salary costs from Statistics Norway [20] adjusted to 2021 values using the Norwegian inflation index for healthcare [18] and social costs (factor 1.4). This produced a cost per hour of €69. We assumed that one clinical pharmacist could deliver the intervention for an average of 30 patients per working week (1.33 hours per patient), based on experience with performing the associated steps in clinical practice. This resulted in an intervention cost of (€ 69*1.33) €92 per patient. For the cost-effectiveness analysis, we assumed that the tasks performed by the study pharmacists were not conducted in standard care and could be performed without additional time spent by the ward staff.
2.5 Statistical AnalysisWe estimated incremental QALYs (∆QALY) as the mean difference in QALYs per patient between the groups, based on mean utility at each observation point and an area-under-the-curve approach. Mixed-model regression was used to model the multi-level structure of the data in terms of repeated measures on an individual level, as well as missing timepoints [21,22,23,24]. The model was fitted with a clustering on the patient level. Clustering on the ward level did not contribute to the model, indicating that the variation between wards was not significant between the study wards and was not included. The model included an interaction term between treatment and time and an unstructured covariance matrix was applied [22]. We adjusted the model for the assumed fixed baseline utility [16, 22, 25]. All other baseline characteristics in Table 1 were tested as covariates, and the following covariates significantly contributed to the model: the total number of medications (continuous), receiving multi-dose dispensed medication (yes/no), home dwelling (yes/no), and receiving home care services (yes/no).
Table 1 Characteristics of the total population (N = 285), non-long stayers (n = 222), and long stayers (n = 63)Incremental costs (∆C) were reported as the difference in mean total per patient costs between the groups. Cost differences were adjusted for costs in the year before the index hospital stay using linear regression. All costs were described with bias corrected 95% confidence intervals (CIs) calculated by bootstrap, to account for skewed cost data [26].
The incremental cost-effectiveness ratio (ICER) was calculated as the ratio between the incremental cost and incremental QALYs comparing the intervention and control groups, using the following equation: ICER = ∆C/∆QALY. The uncertainty of the ICER was assessed by pairwise bootstrapping of 1000 ICERs plotted in a cost-effectiveness plane. A cost-effectiveness acceptability curve was generated from the 1000 bootstrapped ICERs for several willingness-to-pay (WTP) thresholds, to assess the likelihood that the intervention is cost effective compared to standard care. As the Norwegian societal WTP threshold for gaining 1 year in full health depends on the severity of the condition calculated from absolute shortfall, we report a range of €27,067–81,201 (NOK 275,000–825,000) as recommended by Norwegian authorities [14, 27].
Because of a capacity problem in primary healthcare during the IMMENSE study conduct, hospital stays were extended beyond the patients’ need for hospitalization for some participants; however, the available data do not distinguish between patients who needed extended hospital care and those affected by the capacity problem. Before unblinding the group allocation, we inspected the distribution of extended stays between the study groups. We applied a cut-off for hospitalizations of ≥ 14 days, as this was twice the length of a mean hospital stay in the data material. A post-hoc subgroup analysis was undertaken for patients with at least one hospitalization (index or readmission) of ≥ 14 days, hereafter called long stayers, and those with no such extended hospitalizations, hereafter called non-long stayers.
All statistical analyses were carried out using Stata 17. The analyses were conducted with a 12-month time horizon from discharge, and thus QALYs and costs were not discounted.
留言 (0)