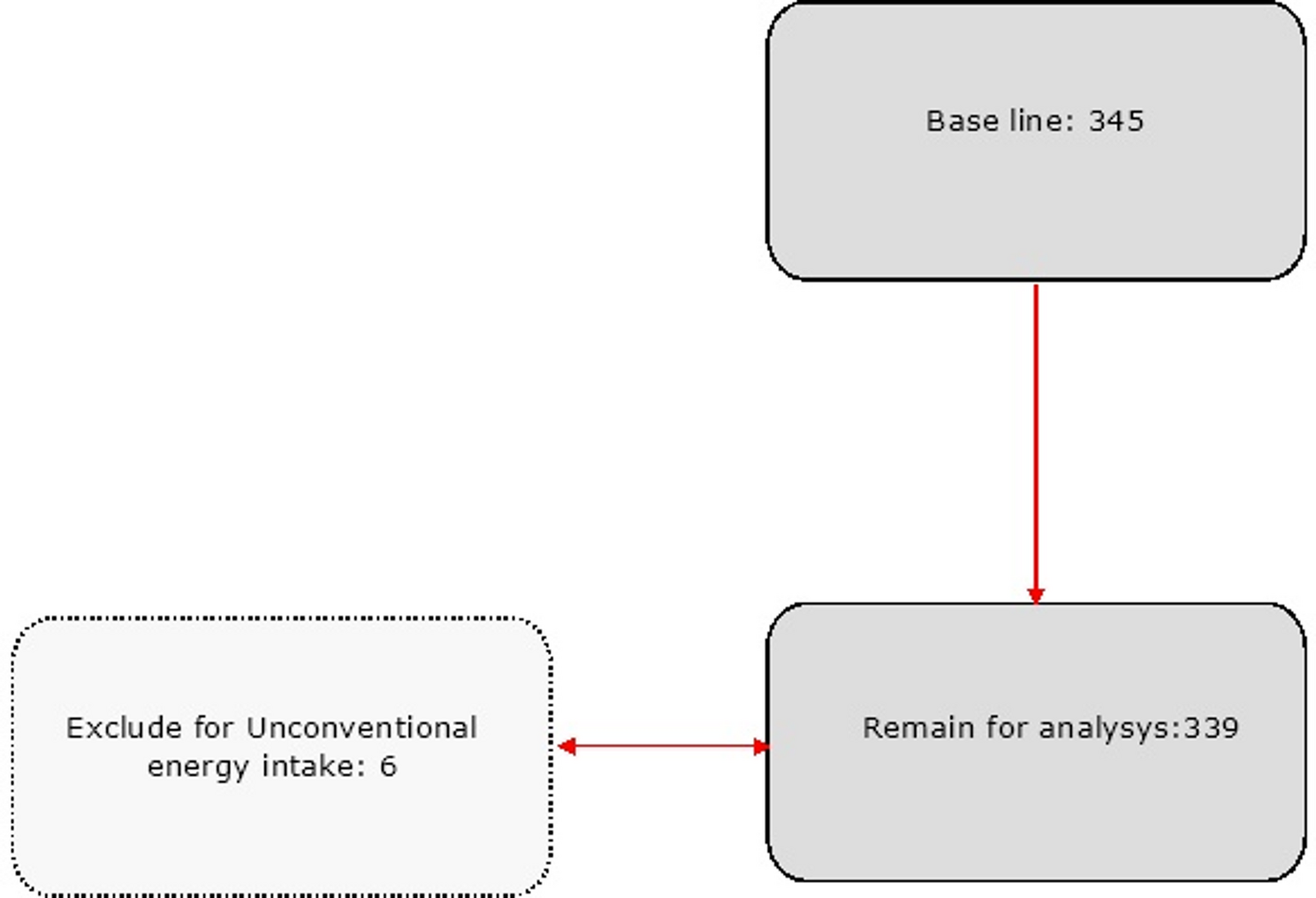
This cross-sectional study was conducted in Kabul, a city with more than 160 health facilities and 22 municipalities [13]. We used a multistage random sampling technique, in each zone of Kabul (North, East, West, and South), we first randomly selected one municipality and from each municipality we randomly selected one health centre. Three comprehensive health centers (CHCs) were selected from the 15th (North), 13th (West), and 9th municipalities (East) [14]. One district hospital was selected from the 16th municipality (south) [14]. From these health centers, we took a convenience sample of 421 reproductive-aged women. Equal samples of women of reproductive age (n = 105) were included from three of the health centres and (n = 106) from one health center according to the following formula [15]:
α = 0.05.
Z = 95% (1.96)
P = 47 (P = 47%, the prevalence of overweight among wealthy reproductive-aged women) [16].
q= (1-0.47) = (0.53)
$$n\, = \,\frac}})}^2}pq}}^2}}}\, = \,\frac^2}\,0.47\,x\,0.53}}^2}}}\, = \,382.7\, \approx \,383$$
For the non-response coverage of the study, we add the 10% to our sample size, which is calculated as 10% of participants= (10*383)/100 = 38 people. We then added 38 to our total sample size, 38 + 383 = 421 participants. An equal number of routine attending women (n = 105) were sampled from each of the four health centres. Women of reproductive age (15–45 years) who agreed to take part in this study and who were clients of selected clinics, as well as women with no dietary restrictions, were included in this study. We excluded women of reproductive age who had previously been diagnosed with a mental disorder by a psychiatrist.
Assessment of dietary intake
All women’s dietary intakes were assessed using a 24-hour recall questionnaire ,which is a reliable and validated method [17, 18]. Dietary intakes were collected on three days of the week, on two weekdays and on one weekend day [19]. To facilitate the data collection, interviewers used a variety of tools to determine serving sizes, including can sizes, a chunk of bread that could fit in the palm of a hand, tablespoons, teaspoons, ladles, plates, bowls, glasses, and photographs of common household meals. Portions sizes were estimated based on household eating/cooking equipment and quantities were reported. Then, the quantities were entered into Nutritionist 4 (NUT4) software for nutrient adequacy analysis and were converted into grams. Total and mean intakes of each food and nutrient consumed were then calculated.
Assessment of anthropometric indices
Anthropometric indices, such as weight, height, waist circumference and body mass index (BMI) were measured and computed for all participants. BMI was calculated by dividing weight (kg) by height2 (m). A calibrated digital scale (SECA 831, Germany) was used for weight measurements. Waist circumference (WC) was measured using an unstretched flexible anthropometric tape at a point midway between the lowest rib and the upper edge of the iliac crest, after normal expiration and without applying pressure to the body surface. We used the World Health Organization (WHO) adult BMI classifications: BMI < 18.5 for low weight, BMI = 18.5 to 24.9 for normal weight, BMI = 25 to 29.9 for overweight, and BMI ≥ 30 for obesity [20].
Assessment of common mental health problems
We used the Depression, Anxiety and Stress Scale − 21 Items (DASS-21), a set of self-report scales to assess symptoms of depression, anxiety and stress. The DASS-21 scale has one section for depression, another for anxiety and a final section for stress (each section contains seven items) [21]. Depressive symptoms were assessed by evaluating dysphoria (a feeling of general dissatisfaction with life), hopelessness, devaluation of one’s life, self-deprecation, lack of interest, anhedonia (inability to experience pleasure), and inertia (a tendency to do nothing). The anxiety component includes autonomic arousal, skeletal muscular responses, and a subjective feelings of anxious affect. The stress component is sensitive to persistent non-specific stimulant levels. The reliability and validity of this instrument have been measured both locally and internationally and is available in 34 languages [22].
The CMHPs have been categorized into three categories: normal, moderate, and severe. The cut-off point for depression is (normal < 13, moderate = 14 to 21, and severe > 22), for anxiety ((normal < 9, moderate = 10 to 14, and severe > 15), and for stress (normal < 18, moderate = 19 to 25, and severe > 26).
Assessment of methyl donor nutrients intake
Dietary intake of methyl donor nutrients (Vitamin B2, B6, folate, B12, methionine, betaine and choline) were calculated using Nutritionist 4 (NUT4) software. The aforementioned nutrients were extracted for each participant and then each of these nutrients were calculated for each individual from the 1st up to the 10th decile. Total scores were derived by summing the scores of each participant (range 7 to 68) and categorized into tertiles. We considered the cut-off points Q1 < 23, 46 < Q2 > 23 and > 46 for Q3. We then considered demographic variables such as women’s age, level of education, monthly household income, marital status, place of residence, history of disease (blood pressure and diabetes) among the tertiles.
Physical activity questionnaire (IPAQ)
The IPAQ is a self-report questionnaire developed in 1998. The reliability and validity of this questionnaire was tested in 12 countries in 2000. The final results suggest that it is an acceptable measure in many countries and in different languages. We used the long form of the IPAQ, which contains four sections (work, cycling/transport, house/garden and leisure) with 27 items [23] and three categories of vigorous, moderate and light physical activity in the last 7 days [24].
Statistical analysis
The quantity of nutrients consumed by each participant was calculated using Nutritionist IV software. The data were analyzed using the Statistical Package for Social Science (SPSS Version 26) software. Regarding individuals’ general characteristics, Chi-square tests and one-way ANOVAs were performed. To assess nutrient intake of methyl donor nutrients and food groups, we used the residual model test while adjusting for energy intake. We fitted logistic regression models to assess the risk of CMHPs based on methyl donor tertiles..




Comments (0)