
Remember me








General practice or primary care is a vital component of contemporary medicine worldwide and the largest specialty of most healthcare systems.1 Primary care is central to patient healthcare. Furthermore, maintaining an efficient and accessible general practice is essential to how patients perceive this care.2,3
In many countries, general practitioners (GPs) are the foundation for meeting the growing demand for healthcare caused by increases in the older population, progressively complex patient needs, and expanding treatment possibilities.1 As the World Health Organization acknowledges, primary care is essential to address patient needs.4
In the Netherlands, every resident is encouraged to register as a patient in a general practice.5 For all noncritical health problems, patients consult their GP first. The GP oversees various conditions, from common ailments to chronic diseases, and manages patients longitudinally. When more complex problems arise, the GP serves as a gatekeeper and refers patients to an appropriate medical specialist in a hospital or ambulatory care setting.1
About 13,000 GPs are clinically active across about 5,000 general practices in the Netherlands.5 A typical patient visits the GP office 4.3 times per year.6 Most (92%) new health problems present in primary care.7 In the aggregate, the healthcare provided by GPs contributes to efficient and low-cost services with a high patient satisfaction rate.8 The biggest challenges to general practice care in the Netherlands are the high workloads and long hours.6,9
General practices in the Netherlands are organized under two structures: a GP physician as the practice owner (self-employed) or an association consisting of several GPs as salaried employees.10 In the first case, the GP is directly responsible for the business results as an entrepreneur, and the GP's income is derived from the practice results. In the larger organizational model, GPs are contracted employees. Although there is a trend toward more group practice arrangements, most Dutch GPs work in small practices of three or fewer GPs.11 Evening and weekend services are separately organized and not included in this study.12,13
Since the start of the new century, PAs and NPs have been included as medical care providers in Dutch general practices.14 The central drivers for this change are universal: the increased demand for healthcare due to an increase in the older population and the shifting of less-complex, specialized medical care from hospitals to general practices.15 The introduction of PAs and NPs in 2001 was a national strategy to reduce the workload of GPs and other specialties and to provide more cost-effective care.2,13,16
Worldwide, evidence has been accumulating about the usefulness of PAs and NPs and their quality of care.17,18 However, the financial and organizational benefits of employing PAs and NPs in general practices have yet to be thoroughly investigated.13 We set out to examine whether the employment of a PA or NP can benefit GPs' workload, both quantitatively and qualitatively. The research questions were:
What are the financial aspects of PA or NP employment in a GP practice? Does the employment of a PA or NP in a GP practice have benefits beyond financial ones? METHODSThe Radboud University Medical Center's research ethics committee approved the research protocol. Informed consent was obtained from all subjects.
A descriptive study and a mixed-methods approach were selected to explore PA and NP employment in representative general practice arrangements. The intent was to identify the contribution that the PA or NP provided to the GP's workload. A second focus was on the employment costs of an NP or a PA and their financial benefit as employees in terms of return on investment (ROI).
Study sampleFour representative types of practices were selected based on input from an advisory group.
Self-employed GPs with a direct personal financial interest in an NP. Self-employed GPs with a direct personal financial interest in a PA. A group GP practice in which the GPs are contracted, and which employed an NP. A group GP practice in which the GPs are contracted, and which employed a PA.The selection of practices that met the inclusion criteria was a purposeful sample drawn from a list of Dutch practices employing at least one PA or NP.19 Criteria were the employment of an NP or PA for the past 2 years, the staff agreeing to interviews, GPs willing to provide financial and organizational practice data, and the practice willing to make available patient care data. The selection was completed when four candidate practices were willing to participate and met the inclusion criteria. Because of the sensitivity of the data requested, the funds available, and the amount of work to collect and analyze the data, the project was limited to four practices that could represent the range of interest.
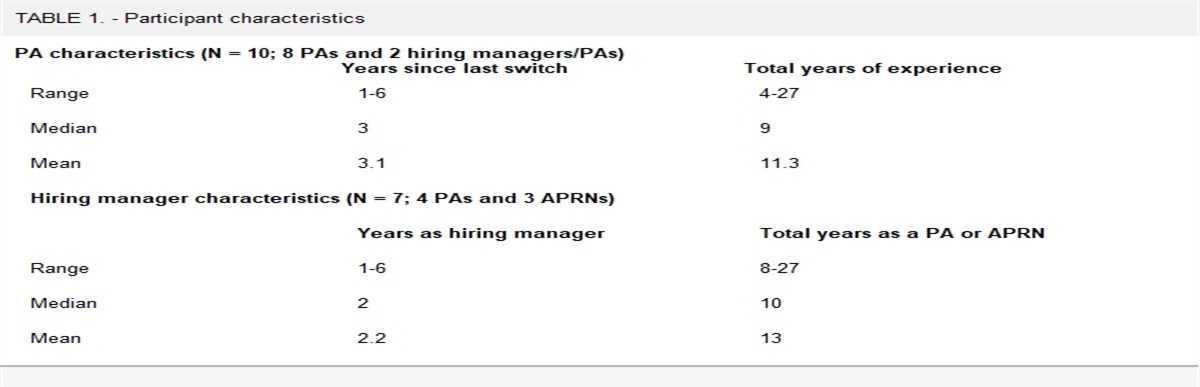
We invited family physicians to form a reference group to maintain a grounding in our work. All were recruited from the medical school's GP training program. In total, 13 GPs agreed to be a part of the reference group; seven solo practices (employing three PAs and four NPs) and six associated or group practices (four employed a PA and two employed an NP). The medical school-associated GPs served as a content validation measure to determine whether the results from the four practices were generalizable. The practice data were collected in 2018 (Table 1).
TABLE 1. - Variables and data sources Quantitative data Qualitative data GP single-owner practice with NPExtraction data from patient information system
Reimbursement information:
Information about personnel:
Number
Hours per week
Salary
Function
Roster data
Interviews with GP, PA, NP, primary care RN, GP assistant, and GP managers:
Interviews with NP/PA:
Task profile
Motivations
Barriers
Working hours
GP single-owner practice with PA GP in association with NP GP in association with PA Validation A group of 13 GPs provided their experience with PAs and NPs. The 13 GPs represented seven solo practices (employing three PAs and four NPs) and six GP associations (employing four PAs and two NPs).To obtain information on quality, accessibility, patient experience, and workload, we interviewed clinicians and support staff. The data were enriched with roster details and information on the practice operation. In total, 23 individual interviews were held, and between five and eight interviews were undertaken with each practice. The interviewees included the solo GPs and at least two GPs in the group practices. Each employed PA or NP was interviewed. In addition, the GP assistant, medical assistant, primary care RN, GP manager, and, where available, a GP resident or NP student were interviewed (Table 2). Participation was voluntary, and participants were not compensated or rewarded for their contributions. None of the interviewees declined, dropped out, or refused to answer questions. One of the two researchers/interviewers recorded all interviews individually and coded and matched them for consistency. Following the interviews, the codes of the two researchers (AJK and YG) were compared and discussed until a consensus was reached.20
TABLE 2. - Characteristics of assessed general practices P1 with one NP (One GP as owner) P2 with one PA (One GP as owner) P3 with one NP (Association of GPs) P4 with one PA (Association of GPs) Number of enrolled patients 2,262 4,235 9,805 4,912 Number of GPs 1 (1 FTE) 4 (2.3 FTE) 5 (3.9 FTE) 2 (1.3 FTE) Number of NPs 1 (0.58 FTE) - 1 (0.95 FTE) - Number of PAs - 1 (1 FTE) - 1 (0.78 FTE) Number of interviews 5 5 8 5 Practice arrangement of the interviewee1 GP
1 NP
2 GP assistants
1 GP manager
1 GP
1 PA
1 GP assistant
1 primary care RN
1 GP manager
2 GPs
1 GP resident
1 NP
1 student NP
1 primary care RN
1 medical assistant
1 GP manager
1 GP
1 PA
1 GP assistant
1 primary care RN
1 GP manager
The findings from the four GP practices were presented to a reference group of 13 GPs to affirm that the sampled practices were typical and not distorted by confounding. This reference group, drawn from a university medical school, reflected on the findings throughout. The discussion with the reference group, led by an independent chair, focused on the results of the practices examined and compared those results with results of the practices of the 13 GPs. The opinions, ideas, and beliefs about whether these four select practices represented Dutch GPs were recorded.
Quantitative data collectionTo understand the effects on production and calculate the ROI, medical and financial quantitative data were collected, along with quantitative information about the employment of the PA or NP. The procedures, patient schedules, patterns of business, and annual reports supplemented the administrative data. These data were used to calculate the ROI component of this study. In the Netherlands, GPs use a standardized computer system to administer and store patient encounter data. The electronic General Practice Information System (GPIS) consists of routine care, health insurance information, morbidity information, history of contact with healthcare providers, and patient information. The GPIS-linked administrative and encounter data are used to submit billable claims to healthcare insurance companies to reimburse services and to registries for research purposes.21 The four practices made their GPIS available to the research team, including financial and patient care data. The quantitative data were extracted from the GPIS for enrolled patients, as were the International Classification of Primary Care (ICPC) codes and the number of visits per day, week, and year correlated with the type of healthcare provider. The patient's reason for a visit (that is, presenting complaint) was compiled separately. In addition, the reimbursement returns and other financial data were extracted from the practice's information system or derived from the business operations. To gain insight into the pecuniary aspects of a GP practice, the financial data for 2018 were examined as the most recent year of the research. In Practice #2 (P2), the PA worked clinically for 8 months in 2018, and the data were extrapolated to 12 months.
A central focus was the labor costs and benefits associated with the PA or NP and their contribution to the overall production in each general practice. Therefore, we included data on personnel information, the number of employees, employee function, hours worked per week, salary, and roster (schedule information) from the information system. In interviews, we gathered information on task profiles, workload, working hours, motivations, and barriers to employment. The billable revenues generated by the PA or NP relevant to their employment were assessed. The data obtained from the GPIS of the four practices also were obtained from the 13 GP practices that served as the reference group for validation purposes.
Data analysisAll qualitative data from semistructured interviews were recorded, transcribed, coded, and processed in ATLAS.ti, a computer program for qualitative data analysis. A coded list of questions was developed before the interviews, and the codes were used to compare transcribed responses.
ROIThe ROI of adding an employee to a practice was viewed as a straightforward but key measure of profit derived from the investment (employment). This measure was used to evaluate the rank attractiveness of the new hire in terms relative to cost.
All quantitative data were extracted from the GPIS. The total production of the practice and the production of the GP, PA, or NP, along with the overall financial turnover, were analyzed based on ICPC and were calculated as part of the general practice characteristics. The financial annual effects of employing a PA or NP were calculated using billable care as income generated by their employment, and the costs were salary costs, including 35% overhead. The cost of education or training was not included because the government finances healthcare professional education and universal healthcare insurance.
Next, the quantitative and qualitative data were presented as preliminary findings and discussed with the GP reference group. A set of validated results were agreed upon and advanced as reportable.
RESULTS Characteristics of general practicesThe number of GPs ranged from one to five in general practice offices, and the full-time equivalent (FTE) of the GP ranged from 0.58 to 1 (Table 2). The FTE for the PA ranged from 0.78 to 1, and the NPs from 0.58 to 0.95.
Across the four practices, the patient census ranged from 2,262 to 9,805 (mean of 5,303). The number of empaneled patients per FTE GP was 2,599 (1,841 to 3,778). When the NP or PA was added to a GP practice, patients per FTE clinician (GP, NP, or PA) averaged 1,774 (1,283 to 2,315). The average number of consultations (encounters), home visits, telephone sessions, and procedures performed by GPs over the four practices per year converted to FTE was 6,839; for the NPs, 2,636; and for the PAs, 4,926. The list of ICPCs consisted of 1,257 diagnoses and spanned a broad spectrum of conditions. All four practices had similar patient populations and diagnoses. The most common conditions seen by GPs, PAs, and NPs were musculoskeletal, dermatologic, and respiratory disorders. The two PAs saw a broader range of patient diagnoses in the four practices than the NPs: GPs averaged 493 unique ICPCs, PAs 369, and NPs 205 (Table 3). However, the NPs in both practices were involved with more time-consuming older adults than the GP or the PA.
TABLE 3. - Number of different ICPC diagnoses in 2018 Practice Number or span of ICPC diagnoses Percentage of PA or NP ICPC diagnoses compared with the GP P1 NP 263 58 GP 455 P2 PA 401 77 GP 523 P3 NP 146 25 GP 589 P4 PA 336 83 GP 405Based on the interviews, the practice staff's most frequently mentioned effect of the new PA or NP was that each could offset the workload demands of the practice, giving the GP more time for complex patients. The division of labor resulting from PA and NP employment implied better productivity and improved efficiency, which appears to have increased GP job satisfaction. The increased time for patients as a result of the new employee was mentioned by the staff but not quantified.
Some of the comments about the qualitative aspects of the PA/NP were:
GP2: The PA provides “less stress for the GP and more relief of workload with more time per patient and more time for management tasks.” PA2: The PA “helped [alleviate] the increase in work pressure for the GP.” A comment from the GP reference group was that the NP or PA seems to know their boundaries or roles well. A comment from a GP was that the PA or NP had more time per consultation than a [typical] GP. This time was perceived by the patient and staff as a quality-of-care enhancement. Another comment was that a solo practice lacked the time commitment to train or guide [on-board] the PA or NP. ROIThe productivity of the NP and PA expressed as a percentage of billable services (such as consultations, home visits, and telephone consultations) was 70% to 100%, with an average of 71% for the NPs and 85% for the PAs. The other tasks were nonbillable aspects of care, such as completing forms, insurance concerns, and addressing administrative issues. NPs were involved in more in-home visits and telephone consultations than PAs, who primarily provided care during consultations (Figure 1). Except for the fourth practice (P4), about 30% of the tasks were listed as other. No traceable differences were found between practices owned by GPs or group practices.
 FIGURE 1.:
FIGURE 1.: Percentage of billable production in 2018
The ROI of PAs and NPs was positive in three practices (Figure 2). In P2 (one GP and one PA), the PA's employment costs exceeded the PA's revenue, with an ROI of 91%. This was due to a relatively large portion of the PA's duties (about 30%) being administrative, not billable, and the PA having a relatively high salary.
 FIGURE 2.:
FIGURE 2.: Cost and reimbursement of PAs and NPs in 2018
In P3, the NP often managed older adults and received additional reimbursement for home visits. In P4, the PA mainly performed consultations that differed in quantity and diversity, at least from those of the GP in the same practice.
Content validation of the reference groupAfter collecting and analyzing the data from the four case studies, focus interviews were undertaken with the GP experts. In the validation or reference group, 10 of the 13 GPs had experience with an NP or PA in their practice. An overview of their characteristics can be found in Table 4.
TABLE 4. - Characteristics of reference group GPs who had experience with a PA or NP Practice Number of PAs or NPs Number of enlisted patients GP A GP as owner 2 PAs Unknown GP B GP in association 1 PA 5,000 GP C GP in association 2 PAs 140,000 GP D GP in association 2 NPs 2,300 GP E GP as owner 1 PA 5,000 GP F GP in association 2 NPs 9,000 GP G GP as owner 1 NP Unknown GP H GP in association 3 NPs Unknown GP I GP in association 2 NPs 3,500 GP J GP in association 4 NPs UnknownA summary of comments made by the GP reference group:
Reduction of workload and patient panel growth were recognized reasons for hiring a PA or NP. The diversity in the background and work experience of the PAs and NPs was considered in the hiring interview. The characteristic that stood out most was that the PA or NP had a broad range of caseloads across all age groups. The NP's role often involved care of older adults and long-term care more than the PA's role. One comment from the representative GPs was that PA and NP onboarding could take up to 1.5 years to achieve maximum employment. In addition to productivity, sharing the workload, and a sense of collaboration, many suggested another clinician (PA or NP) could be considered to handle a growing caseload. This added clinician factor could not always be calculated into maximum production gains but was noted by many interviewees as an attribute that could further improve office flow. DISCUSSIONAnalyzing the broadly drawn data from four Dutch general practices seems to have revealed the subjective value of an employed PA or NP on GPs' workload and the objective value of the ROI. At the same time, no difference was found between practices owned by GPs or GP group practices. In the aggregate, each of the PAs or NPs was productive and saw many patients. Clearly, these clinicians were value-added and helped to reduce the GP's workload. In three of the four cases, the ROI was positive. In P2, the PA was engaged more in improving the administrative aspects of the practice early in his employment and, consequently, reduced reimbursable productivity. However, the organizational improvement activity was considered temporary, and later the PA was focused full-time on patient care.
The gathered data in this study show a division of labor in the annual output of services that involves a PA or NP in a typical Dutch general practice. The effect on workload was attributed, as evidenced by the interviews with GPs, to the fact that a PA or NP accounts for some of the productivity, which is supplemented by performing additional tasks. These aspects have alleviated some of the perceived workloads of the GPs. Three of the practices in this study enrolled more patients than the national average of 2,085 patients per FTE. Although the results are confined to four out of 500 GP practices in the Netherlands, they are representative, broadly speaking, of how GPs could benefit financially and subjectively by employing PAs and NPs.
Understanding the favorable effect of incorporating a PA or an NP in a medical practice is a growing healthcare professional labor topic in Europe and North America.22,23 For example, Halter and colleagues in the United Kingdom found that PAs were increasingly used in significant medical consultation roles in primary care.24 Pany and colleagues validated a series of studies in the United States that team-based care produces better outcomes than solo practitioners.25 Leach and colleagues noted that the outcomes for patients with chronic diseases treated by PAs, NPs, or physicians revealed no differences, suggesting that a broad range of care can be collectively managed by PAs, NPs, and physicians.26
Our study showed that in addition to their reimbursed productivity, PAs and NPs saw a wide variation in patient conditions: the PA saw 75% of the same conditions and the NP 42% of the same conditions as seen by the GP. The consensus of the reference group was that this addition to the staff contributed to offsetting some of the GP workload.
The literature on PA and NP employment ROI is scarce. However, two systematic reviews on PAs and NPs spanned 72 cost-effectiveness studies.18,27 The reviews concluded that PAs and NPs are cost-effective in most employment cases, either as a physician substitute or as a complement to improve care output. The ROI was positive in the few instances where it was calculated, because of the relatively high productivity for which revenue was obtained compared with wages.
Primary care providers in the Netherlands, where PAs and NPs are increasingly used, found that employing these clinicians was valuable.17,28 Such findings are seen globally.24,25,29,30 What works best for one clinician or practice is copied by others—but perhaps more importantly, the best practice policy tends to affect all clinicians. In adult medicine, PAs and NPs produce the same outcome as GPs, suggesting that best practices are emulated.
LIMITATIONS AND STRENGTHSWe questioned whether a dual distinction of a self-employed GP and a group practice of GPs could do justice to all the organizational differences in GP practices. To this end, we validated the generalizability of findings with a sample of GPs. The reference group confirmed that the outcomes of the four practices could be comparable to the approximately 500 GP practices in the Netherlands. A note was added that the 1-year familiarization period, as the inclusion criterion in this study, may be on the short side, and the effects of employability could improve after a year or two. Although relevant topics such as quality of care and patient satisfaction were not measured directly in our study, previous studies have shown positive effects of PA or NP employment on Dutch patient satisfaction, with at least equal or higher quality of care compared with care provided by physicians.17,18
All practices and the 13 GPs in the reference group were created through purposeful sampling with voluntary participation. This method has a risk of bias given the broad aspect of the research questions. More critical details such as observing patient-clinician interactions, time-motion studies, the role of general practice assistants or primary care RNs, and the effect of other office staff were the economic tradeoffs for the bigger picture.
A strength of the current study is the large number of interviews with different professionals and the in-depth answers we received. In addition, the participants came from a wide geographic area, and the variation in types of practices was thought to reflect the distribution of practices in the Netherlands.9 Another strength is that the interviews were conducted in a semistructured manner consistent across the four practices.
We have constructed a general representation of the activity of GPs employing a PA or an NP in the Netherlands. More importantly, the global movement reflects the work to include PAs and NPs in family medicine.31 Finally, this undertaking intended to set the stage for a more granular examination of activity in general medicine, how it expands to accommodate a change in the healthcare landscape, and move research to care outcomes.
CONCLUSIONSince PAs and NPs were introduced in Dutch healthcare, primary care practices have grown. The employment of PAs and NPs comes at a time of increased demand, an increase in the older population, and more complex patient care needs. This results in more frequent and prolonged visits to the general practice. We analyzed four representative general practices that employ PAs and NPs. Solo and group practices using PAs and NPs are productive primary care team members and PAs and NPs are worthwhile staff additions in each case. In all four GP practice analyses, the employment of a PA or NP made a valuable contribution to the practice flow while reducing GPs' workloads. In three of the cases, the ROI was positive. In the fourth case, the PA performed additional management tasks that led to a negative ROI. Nonetheless, PA and NP employment was evaluated as a positive contribution to general practice care. More robust research in a larger sample is needed to draw firmer conclusions.
REFERENCES 1. Kringos D, Boerma W, Bourgueil Y, et al. The strength of primary care in Europe: an international comparative study. Br J Gen Pract. 2013;63(616):e742–e750. 2. Freund T, Everett C, Griffiths P, et al. Skill mix, roles and remuneration in the primary care workforce: who are the healthcare professionals in the primary care teams across the world. Int J Nurs Stud. 2015;52(3):727–743. 3. Donabedian A. Evaluating the quality of medical care. Milbank Q. 2005;83(4):691–729. 4. World Health Organization and United Nations Children's Fund (UNICEF). Operational framework for primary health care: transforming vision into action. Technical series on primary health care. Geneva: World Health Organization; 2020. https://apps.who.int/iris/handle/10665/337641. Accessed August 29, 2023. 5. Batenburg B, van der L. Velden. Cijfers uit de registratie van huisartsen—een update van de werkzaamheidscijfers voor 2018 en 2019. [Figures from the register of GPs—an update of the employment figures for 2018 and 2019.] www.nivel.nl/sites/default/files/pdf/extra_uitgave_cijfers_registratie_huisartsen_2019.pdf. Accessed August 31, 2023. 6. Schäfer WLA, van den Berg MJ, Groenewegen PP. The association between the workload of general practitioners and patient experiences with care: results of a cross-sectional study in 33 countries. Hum Resour Health. 2020;18(1):76. 7. Faber MJ, Burgers JS, Westert GP. A sustainable primary care system: lessons from the Netherlands. J Ambul Care Manage. 2012;35(3):174–181. 8. Stadhouders N, Kruse F, Tanke M, et al. Effective healthcare cost-containment policies: a systematic review. Health Policy. 2019;123(1):71–79. 9. van Hassel D, Verheij RA, Batenburg R. Assessing the variation in workload among general practitioners in urban and rural areas: an analysis based on SMS time sampling data. Int J Health Plann Manag. 2019;34(1). 10. Zaat J. Continuïteit [Continuity]. Huisarts en Wetenschap. 2018;61:12–16. 11. van Braak M, Visser M, Holtrop M, et al. What motivates general practitioners to change practice behaviour? A qualitative study of audit and feedback group sessions in Dutch general practice. BMJ Open. 2019;9(5):e025286. 12. Smits M, Rutten M, Keizer E, et al. The development and performance of after-hours primary care in the Netherlands: a narrative review. Ann Intern Med. 2017;166(10):737–742. 13. van der Biezen M, Derckx E, Wensing M, Laurant M. Factors influencing decision of general practitioners and managers to train and employ a nurse practitioner or physician assistant in primary care: a qualitative study. BMC Fam Pract. 2017;18(1):16. 14. Capaciteits Orgaan. Recommendations 2021-2024 Advisory Committee on Medical Manpower Planning: Main report. https://capaciteitsorgaan.nl/app/uploads/2020/04/2020_02_12-Capaciteitsplan-2021-2024-Hoofdrapport-DEFINITIEF-EN.pdf. Accessed September 1, 2023. 15. Figueroa CA, Harrison R, Chauhan A, Meyer L. Priorities and challenges for health leadership and workforce management globally: a rapid review. BMC Health Serv Res. 2019;19(1):239. 16. White R, Keahey D, Luck M, Dehn RW. Primary care workforce paradox: a physician shortage and a PA and NP surplus. JAAPA. 2021;34(10):39–42. 17. Laurant M, van der Biezen M, Wijers N, et al. Nurses as substitutes for doctors in primary care. Cochrane Database Syst Rev. 2018;2018(7):CD001271. 18. van den Brink GTWJ, Hooker RS, Van Vught AJ, et al. The cost-effectiveness of physician assistants/associates: a systematic review of international evidence. PLoS ONE. 2021;16(11):e0259183. 19. Palinkas LA, Horwitz SM, Green CA, et al. Purposeful sampling for qualitative data collection and analysis in mixed method implementation research. Adm Policy Ment Health. 2015;42(5):533–544. 20. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. 21. Smeets HM, Kortekaas MF, Rutten FH, et al. Routine primary care data for scientific research, quality of care programs and educational purposes: the Julius General Practitioners' Network (JGPN). BMC Health Serv Res. 2018;18(1):735. 22. Park J. Nurse practitioner and physician assistant staffing in the patient-centered medical homes in New York State. Nurs Outlook. 2015;63(5):593–600. 23. Peckham A, Ho J, Marchildon G. North American Observatory on Health Systems and Policies. Policy innovations in primary care across Canada. https://naohealthobservatory.ca/wp-content/uploads/2019/08/NAO_RR1.pdf. Accessed September 1, 2023. 24. Halter M, Drennan V, Wang C, et al. Comparing physician associates and foundation year two doctors-in-training undertaking emergency medicine consultations in England: a mixed-methods study of processes and outcomes. BMJ Open. 2020;10(9):e037557. 25. Pany MJ, Chen L, Sheridan B, Huckman RS. Provider teams outperform solo providers in managing chronic diseases and could improve the value of care. Health Aff (Millwood). 2021;40(3):435–444. 26. Leach B, Morgan P, Strand de Oliveira J, et al. Primary care multidisciplinary teams in practice: a qualitative study. BMC Fam Pract. 2017;18(1). 27. Martin-Misener R, Harbman PR, Donald F, et al. Cost-effectiveness of nurse practitioners in primary and specialised ambulatory care: systematic review. BMJ Open. 2015;5(6):e007167. 28. van den Driesschen Q, de Roo F. Physician assistants in the Netherlands. JAAPA. 2014;27(9):10–11. 29. Morgan PA, Smith VA, Berkowitz TS, et al. Impact of physicians, nurse practitioners, and physician assistants on utilization and costs for complex patients. Health Aff (Millwood). 2019;38(6):1028–1036. 30. Conference Board of Canada. Value of physician assistants: understanding the role of physician assistants within health systems. https://capa-acam.ca/wp-content/uploads/2018/11/8107_Value-of-Physician-Assistants_RPT_FINAL.pdf. Accessed September 1, 2023. 31. Arya N, Gibson C, Ponka D, et al. Family medicine around the world: overview by region: the Besrour papers: a series on the state of family medicine in the world. Can Fam Physician. 2017;63(6):436–441.
Comments (0)