The impact of a low-flow state in severe AS patients treated with TAVI, either considering FR or SVi, was assessed and compared. The key findings of the present study are that: (1) a relevant proportion of patients with severe AS have low transvalvular flow states, either assessed using FR or SVi; (2) low-FR is associated with higher all-cause mortality post-TAVI; (3) SVi is associated with mortality after intervention, but not when dichotomized at < 35 mL/m2; (4) low-flow patterns are associated with clinical characteristics portraying worse outcomes and a higher estimated risk, and are not independently associated with worse survival.
The low-flow profile
In the present analysis of 489 patients undergoing TAVI, 62.6% presented low-SVi and/or low-FR, denoting that this low-flow status is highly prevalent in a “real-world” cohort of severe AS patients undergoing percutaneous treatment. Thus, further characterization, including the impact of specific management strategies, should be specifically addressed in this subset. In other severe AS cohorts, low-flow state, considering either SVi or FR, was found in 55% of the patients included [23, 24], reinforcing that this condition is not epidemiologically negligible.
Our results show that low-flow severe AS patients are of higher estimated surgical risk, and present more comorbidities, including coronary heart disease and previous percutaneous coronary intervention. Furthermore, a low-flow state is associated with aggravated symptoms of heart failure, based on NYHA classification.
Stroke volume index and flow rate – the same, only different?
There is uncertainty about which measure is the most suitable for assessing flow through the aortic valve, though the superiority of FR as a flow measure has been suggested [25, 26]. In a sub-analysis of the SEAS (Simvastatin and Ezetimibe in Aortic Stenosis) population, 21% of patients had low transaortic FR at baseline, but only 10% had low-SVi [13]. In another severe AS cohort, 50% of patients exhibited a low-SVi, but only 39% had low-FR [23]. In our population, 59.5% of patients had a low transaortic FR at baseline, but only 43.1% had a low SVi. As both measures are stroke volume dependent, it is expected that these are associated, and our results confirm a moderate positive correlation between them. However, almost one-fourth of patients presented discording flow-states if defined by FR or SVi, being low-FR but normal SVi the most frequent discordance (19.4%). This can be partly explained by the SVi dependence on BSA, contrary to FR [6]. Another potential source for discordance is the higher dependence of SVi on heart rate – patients with higher rates have lower left ventricular ejection time and thus may present with lower SVi despite normal FR [24].
The present study found an association between low-FR and female sex, older age, and lower BMI and BSA, which is in agreement with previous reports [7, 27, 28]. There are several causes pointed for FR (but not SVi) being lower among women, including a lower stroke volume (unindexed) [28], being the latter corrected to a tendentially lower BSA in female patients, which is not currently applicable for FR. On the other hand, AF was more frequent among low-SVi (but not low-FR) cases, which can be integrated in a context of no atrial systolic contribution to left ventricular filling, as well as impaired filling time due to poor ventricular rate control, as described in the literature [29].
A reduced transvalvular flow has recently been associated with a worse systolic function [7], and in the present study both low-FR and low-SVi patients exhibited a lower LVEF, and a higher frequency of low-EF cases. Furthermore, Baron S. et al. reported that ventricular dysfunction was not independently associated with one-year mortality after TAVI [30], suggesting that the prognostic value of FR and SVi is not related to differences in ventricular dysfunction.
Low-flow states can be associated with low transvalvular gradients and erroneously low AVA, since its true measurement is dependent on achieving sufficient transaortic flow to maximize the leaflets opening [5]. In the present analysis, AVA was lower in low-flow patients, according to FR or SVi definition, and low-SVi – but not low-FR - patients exhibited lower transaortic gradients, when compared to normal-SVi.
The role of assessing FR in patients with low-flow, low-gradient AS, and the added value of dobutamine stress echocardiography (SE) has been studied. Chahal et al. found that in patients with low-flow, low-gradient AS, a resting FR, but not SVi or LVEF, predicted AVA changes during SE, and a resting AVA measured under normal-FR state truly reflected AS severity, potentially obviating the need of SE [26]. In patients presenting a low SVi and low AVA, a normal FR suggests that the valvular opening forces are normal and that AS is truly severe, contrary to a potential underestimation of AVA in the context of a low FR [24].
The prognostic value of low-flow and how it should be managed
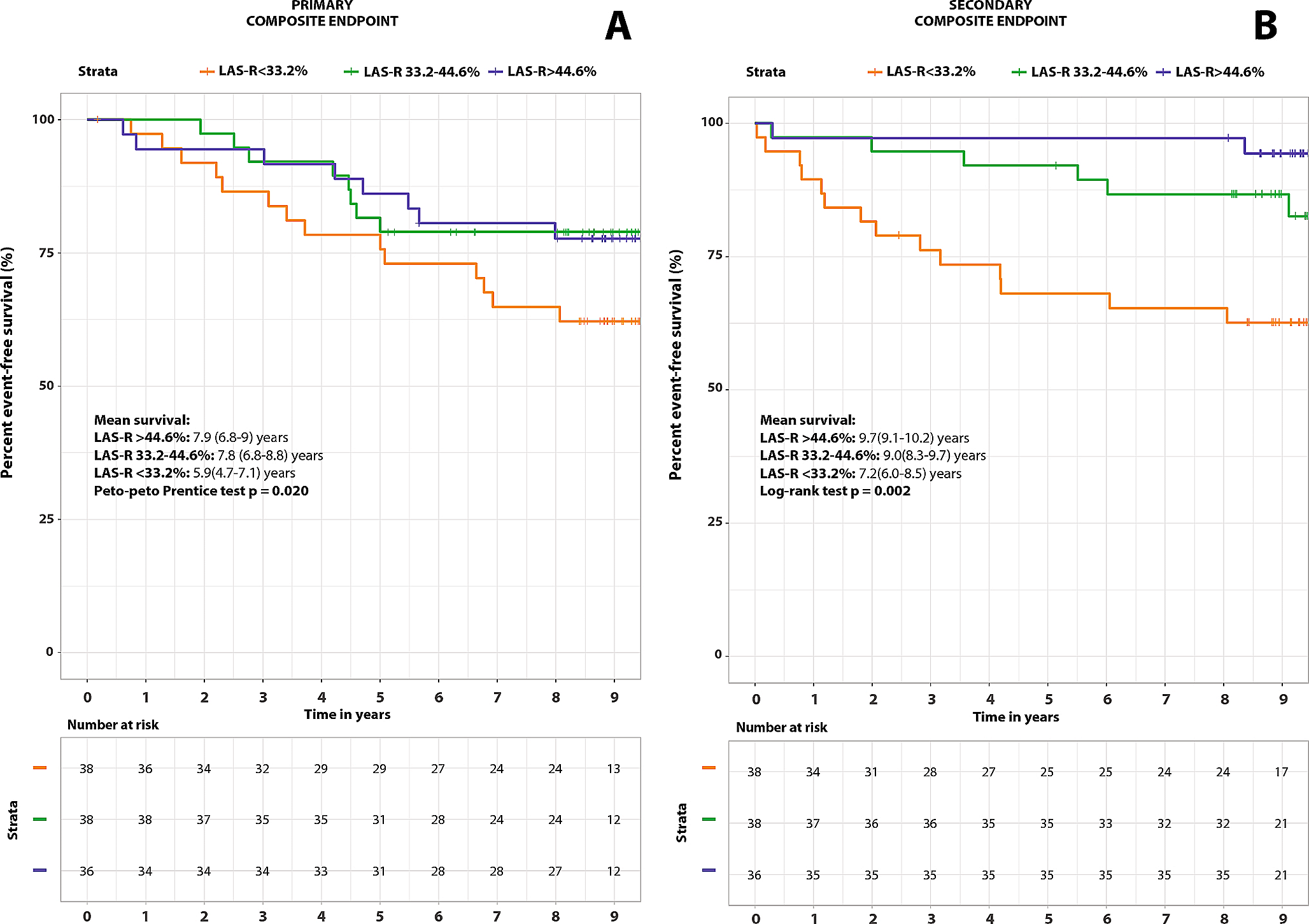
There was an association between low-FR and a 36% higher mortality in patients undergoing TAVI for severe AS. This was consistent with findings from another study on patients proposed for aortic valve intervention, including valvuloplasty and surgical or transcatheter replacement, in which a low-FR had HR = 2.95 for all-cause mortality after procedure, even after adjusting to other factors, including EuroSCORE II [15]. In the present study, there was a tendency towards a higher mortality after TAVI in low-FR patients when corrected to EuroSCORE II, though not reaching statistical significance (p = 0.065). Additionally, a low-FR seems to be associated with higher mortality across different AS states, as this was also seen in initially asymptomatic mild to moderate AS patients [13].
Regarding the prognostic value of SVi in severe AS patients proposed for TAVI, our results denoted that there was a trend towards reduced five-year survival of patients with SVi < 35 mL/m2 versus normal-SVi counterparts, though it did not reach statistical significance (p = 0.085). In fact, a low-SVi has been consistently associated with a higher mortality after TAVI – according to a meta-analysis, there is a 59% increase in one-year mortality after intervention [10]. It can be hypothesized that these findings were not replicated in the present study possibly due to a relatively low number of patients included. Nevertheless, in the present study, when considering SVi as a continuous variable, a higher SVi was associated with a reduction in mortality after TAVI. Therefore, we speculate that, in our population, there is an association between SVi and survival after intervention, but not when dichotomized at a < 35 mL/m2 threshold. Concerns have been raised regarding the optimal cut off to prognostically-define a low-SVi patient, and if it should vary according to sex – namely 40 mL/m2 and 32 mL/m2 for men and women, respectively, according to a study in surgically-treated aortic stenosis patients [31].
The prognostic performance of low-FR and low-SVi has been previously compared. Both are associated with worse outcomes in severe AS patients [16], including low-gradient subset [23]. While Alexandru et al. concluded that both had similar accuracy in predicting death, Sen et al. found that SVi, but not FR, improve risk reclassification when compared with clinical and echocardiographic predictors in low-gradient severe AS patients for a composite endpoint of death and heart failure hospitalization [23].
There are some controversies regarding the additive prognostic role of FR and SVi. In normal-SVi patients, a low-FR is associated with worse prognosis in moderate and severe AS patients [27], but this was not seen in low-gradient severe AS patients who underwent aortic valve procedures [15]. In low-SVi patients, a low-FR predicted higher mortality after valvular intervention [15]. On the other hand, SVi has an impact on mortality on low-FR and normal-FR low-gradient severe AS patients [23], but did not impact survival among treated-AS normal-FR and low-FR patients [15].
Given the difficulty in managing low-flow patients, some studies have suggested that treating them by valvular intervention rather than medically may result in a better prognosis [7]. Saeed et al. reported that all-cause mortality was significantly lower in the aortic valve intervention group (including surgical, transcatheter and balloon aortic valvuloplasty) compared with standard medical treatment, both when low-flow was defined by FR (13.6 vs. 52.3%, p < 0.001) and SVi (15.1 vs. 45.9%, p < 0.001) [32]. Another study demonstrated the superiority of valvular intervention over medical treatment, with TAVI reducing mortality in low-flow patients (HR: 0.48, p = 0.004) [9]. The present study reveals that, despite being associated with worse survival after intervention, the relationship between low-flow states and mortality seems to be related to an underlying clinical context of comorbidities and more advanced cardiac disease, as the association lost statistical significance when adjusted to EuroSCORE II. Therefore, a low-flow condition should not, per se, condition the decision for percutaneous intervention, but alternatively be integrated in an appropriate procedural risk assessment.
Discordant values of AS assessments are stated to occur both at preserved and reduced LVEF [33]. In our population, LVEF was lower and more frequently reduced in both low-FR and low-SVi patients. When reclassifying our population according to this parameter in preserved- versus reduced-EF at a 50% cut off, neither flow parameter retained any prognostic value.
Nevertheless, in the present study, there was a clear symptomatic benefit from performing TAVI in these severe AS patients, with a reduction in heart failure symptoms, evaluated through a substantial functional improvement of NYHA class at six-month, irrespectively of flow state. Thus, a similar symptomatic improvement might be expected in treated low-flow versus normal-flow patients. Given the poor prognosis of severe AS medically treated and the clear symptomatic benefits of TAVI in these patients, this procedure should be considered as a viable treatment option in patients with low-flow AS, whether assumed using FR or SVi.
Transaortic flow rate – where should we draw the line?
The most adequate cut-off defining low-flow according to FR remains conflicting, with studies using a wide variety of cut-offs, ranging from 200 to 250 mL/s. Namasivayam et al. referred to “low-FR” as below the median found in the respective study population (242 mL/s) [27], while other groups found 211 mL/s as the best cut-off value for predicting death from all-causes [14]. The first reported cut-off of 200 mL/s was described in an in vitro experience, considering a normal cardiac output of 5 L/min [34]. As the cut-off of 200 mL/s was the most reported in the literature and for which there was stronger evidence [13, 15, 24,25,26, 34], it was the one considered for the present analysis.
Limitations and strengths
The present study is a retrospective single-center analysis, and marginally non-significant findings might have been conditioned by an insufficient number of patients included. About 25% of patients undergoing TAVI were excluded due to incomplete echocardiographic data, potentially representing a selection bias. As our population was limited to cases with severe AS subjected to TAVI, no extrapolations of this data should be taken for medically or surgically treated low-flow patients. Also, echocardiographic measurements are severely operator-dependent, with an inherent random variability of the collected data, registered blindly to the endpoints defined. Additional information about the cause of death (cardiovascular vs. non-cardiovascular) was not available, as well as other endpoints, such as hospitalizations during follow-up, and therefore no further conclusions could be drawn.
This study is one of the few that questions whether FR represents a mortality predictor in patients who underwent percutaneous aortic valve intervention, and further details on the role of assessing SVi before TAVI as a prognostic marker.


留言 (0)