Payers, such as state Medicaid programs and commercial insurers, face significant financial challenges in covering CGTs due to high upfront costs for these treatments and uncertain long-term effectiveness [3, 27]. Using a case study of paying for CGTs for hemophilia A and B for a state Medicaid program (Colorado), our study has three main findings that can inform how insurers determine coverage and negotiate payment rates for CGTs. First, using real-world data generates very different estimates of breakeven times relative to published literature on clinical trials and cost-effectiveness analyses. Second, estimated costs, cost offsets, and breakeven times depend upon the eligibility criteria for treatment, such as disease severity. Third, as CGTs are often used to treat relatively rare conditions, there is substantial variation in the cost of treatment prior to gene therapy, which increases uncertainty about breakeven time. To address the challenges of paying for CGTs, state Medicaid agencies, as well as some commercial payers, are considering alternative payment models such as VBCs to spread payment over time and tie payment to longer-term treatment performance. However, setting appropriate contract terms requires accurate estimates of the actual costs of the standard of care.
By comparing the impact of using actual or literature-based cost inputs in the simulation, for hemophilia A and B, we find literature-based cost inputs for current treatments are higher. Medicaid real-world data indicate that only 5% of patients with hemophilia A and 13% of patients with hemophilia B are associated with the costs of standard care suggested by the economic evaluations (around $633,000 for hemophilia A and $689,000 for hemophilia B). This leads to an overly optimistic expectation regarding breakeven time and thus an underestimation of financial risks for the payer of covering CGT. This is likely because economic evaluations rely on cost estimates assuming protocol-based use of the drug and prices that do not reflect Medicaid payments. The reviewed economic evaluations (Online Resources 4 and 5) rely on medication protocols for dosage and frequency, patient weights based on US averages, and unit costs from sources such as Redbook and Medi-Span Price Rx Basic. The lower RWD costs might be attributed to several factors. Prices tend to fluctuate over time, whereas economic evaluations typically rely on constant prices. Additionally, existing literature often assumes complete adherence to prophylaxis, whereas our observations reveal variations in patient-level utilization. Furthermore, the types and share of factor therapies utilized in this study differ from the assumptions made in the literature.
Varying assumptions about eligibility for a CGT change estimated breakeven time and budget impact of paying for these therapies. While clinical expertise should inform the determination of eligibility criteria, VBCs should be designed with consideration for the associated breakeven point, driven by the eligibility criteria. We used the requirement of at least six claims for factor therapies or emicizumab for individuals with hemophilia A and a minimum of four claims for factor therapies for hemophilia B to identify potentially eligible patients. For this population, the base case results suggest a longer payback period than what is indicated by cost estimates derived from the current body of literature. However, altering this criterion has significant implications for spending and the budget, leading to substantial impacts on estimated breakeven time and how Medicaid should structure VBCs.
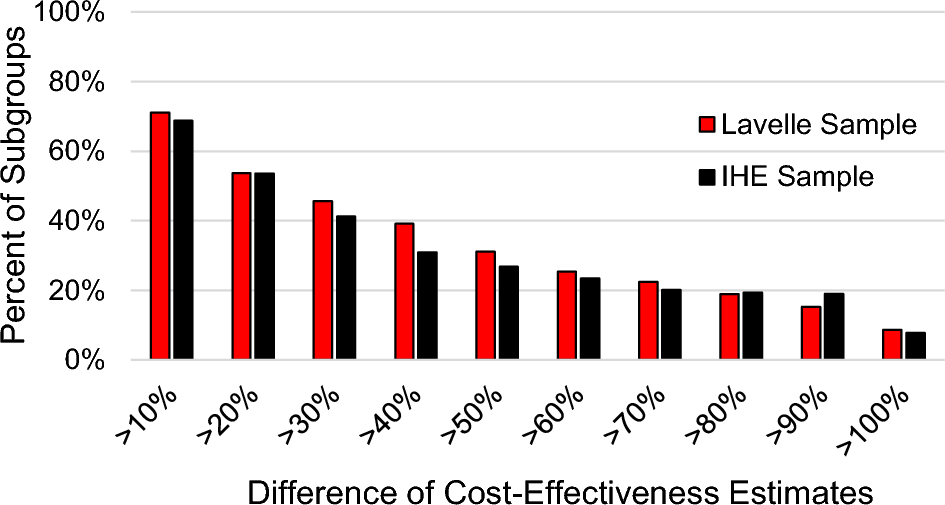
State Medicaid agencies should also design VBCs to account for substantial variations in the costs of treatment that serve as alternatives to CGT. The magnitude of standard deviation we observed (83–99% of the mean cost) in hemophilia A and B aligns with the findings of previous studies utilizing claims data [30, 31]. This underscores the importance of accounting for cost variations in cost simulations, as point estimates in economic evaluations often fail to capture these variations adequately. Although our estimation suggests an average breakeven period of 8 and 6 years when providing gene therapy to patients with hemophilia A or B, respectively, taking into account uncertainty reveals that the likelihood of reaching breakeven within 10 years is approximately 48% for hemophilia A and 59% for hemophilia B. One option to address uncertainty is to pool risk with other state Medicaid programs by developing VBCs that encompass several states. The CMS Centers for Medicare & Medicaid Innovation (CMMI) will test a model to achieve this type of risk pooling, or states may independently choose to pool together [28]. A second option is to construct a more financially conservative VBC where reimbursement to the drug manufacturer is lower or a warranty for refund is set over a longer time period.
Our findings have direct implications for designing VBCs. In the examples provided for CGTs in hemophilia A or B, since the payment is made up front, Medicaid does not have the opportunity to link the payment to expected outcomes over time. A VBC ensures patient access to the gene therapy offering a payback or refund mechanism if the therapy does not deliver the expected results. To enter into a VBC, Medicaid must first understand the cost-offset potential of the CGT, which is a function of the uncertainty around eligibility for the CGT, and the heterogeneity in costs spent on usual care. A deep understanding of how these sources of uncertainty and heterogeneity can provide Medicaid with trade-offs when evaluating the terms of a VBC. For a generic example applicable to CGTs that have large cost offsets, these trade-offs may include higher (lower) refund amounts with shorter (longer) contract durations evaluated at varying levels of eligibility.
4.1 Limitations
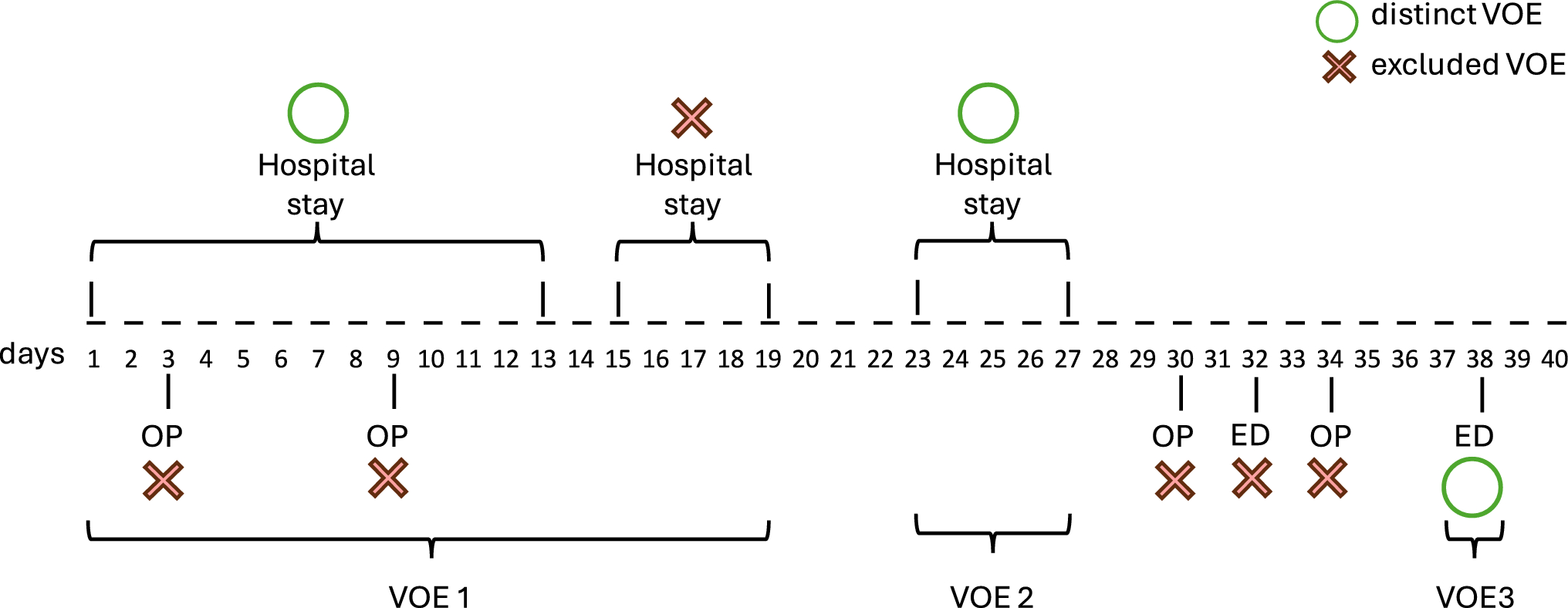
Our analysis has certain limitations. The data we used was specific to Colorado, and therefore may not be representative of the experience of other state Medicaid plans. However, we believe the methodology is transferable to other states and can be used by other Medicaid organizations to design VBCs. The analysis did not account for loss to follow-up. Therefore, it should be acknowledged that savings projected in our simulations may not be fully realized by Medicaid only, as patients have the potential to switch to another payer, such as Colorado’s state healthcare exchange or employer-sponsored insurance. These savings will then be realized at a broader health system level. We recognize that the number of factor claims does not necessarily correspond to the utilization of prophylactic therapy. If available for analysis, the total international units of factor replacement products administered during a specific timeframe may offer a more precise metric for use in value-based agreements. Nevertheless, based on the literature we have reviewed, the number of claims appears to serve as a reliable proxy for indicating the requirement for regular treatment (prophylaxis) and may be indicative of a more severe disease.



Comments (0)