
記住我

Patients treated in ICUs for an extended period have limited mobility and often are connected to a ventilator, increasing their risk of pressure injury (PI).1 A study conducted in Australia found that patients treated in the ICU were four times more at risk for PI development than patients treated outside the ICU.2 The incidence of PI in ICU patients varies by country, with reported incidences of 4.3% on average in China, 5.1% in the US, and 12.5% in France.3 In Turkey, the PI rate among ICU patients varies from 5.9% to 40.6% and reaches 95.6% in ICU patients hospitalized for 10 or more days.4,5
Pressure injuries can cause severe pain and discomfort, prevent healing due to secondary factors, prolong hospital stays, and reduce the patient’s quality of life.6,7 Complications such as infection, sepsis, osteomyelitis, and fistula may occur, and the risk of mortality increases if inadequate attempts are made to prevent and treat PIs.5 The complexity and long duration of PI treatment also increase the cost burden.8 Treatment costs for patients with PIs in the US are estimated to be up to USD $11,000 per person and USD $27 billion per year.9,10 Canada spends CAD $210 million per year on PI treatment. According to the Australian Wound Management Association, the cost of treating a stage 2 PI is AUD $400 per month, and the cost of treating a stage 4 PI is AUD $27,000.11 In Turkey, the annual PI cost is estimated to be USD $1.425 billion.10 Thus, PI prevention is a primary goal because PIs cause related complications, prolong hospitalization periods, increase the cost of care, decrease the quality of life, and are an important indicator of healthcare quality.12
Assessing PI risk using a valid measurement tool and regular repositioning are the most effective and inexpensive methods to prevent PIs. In addition, healthcare providers frequently apply barrier creams to areas of skin at risk for PI development as a preventive measure.13 Barrier creams form a layer between the skin and external factors that helps protect skin integrity by removing the irritant effect of external factors on the skin and any excessive moisture that may occur.14 Barrier creams do not have a standard active ingredient and may contain acrylate terpolymer, dimethicone, paraffin, and isopropyl palmitate. In addition to barrier creams, other creams may be used in clinics as well, such as zinc oxide cream. Zinc oxide is a trace element that plays a vital role in human physiology and is necessary for the repair, proliferation, growth, and strengthening of the immune system.15 Topically applied zinc oxide provides hemostasis in the tissue at risk, increases platelet activation, creates an immune response, and supports enzymatic reactions required for tissue growth.16 Although previous studies have compared zinc oxide creams with barrier creams, there is no definite conclusion about which is most effective for PI prevention.15,17
The aim of this study was to compare the retrospective results of zinc oxide creams and barrier creams in patients who were treated in ICUs and were at risk of PI development to determine their effects on maintaining skin integrity and preventing PI.
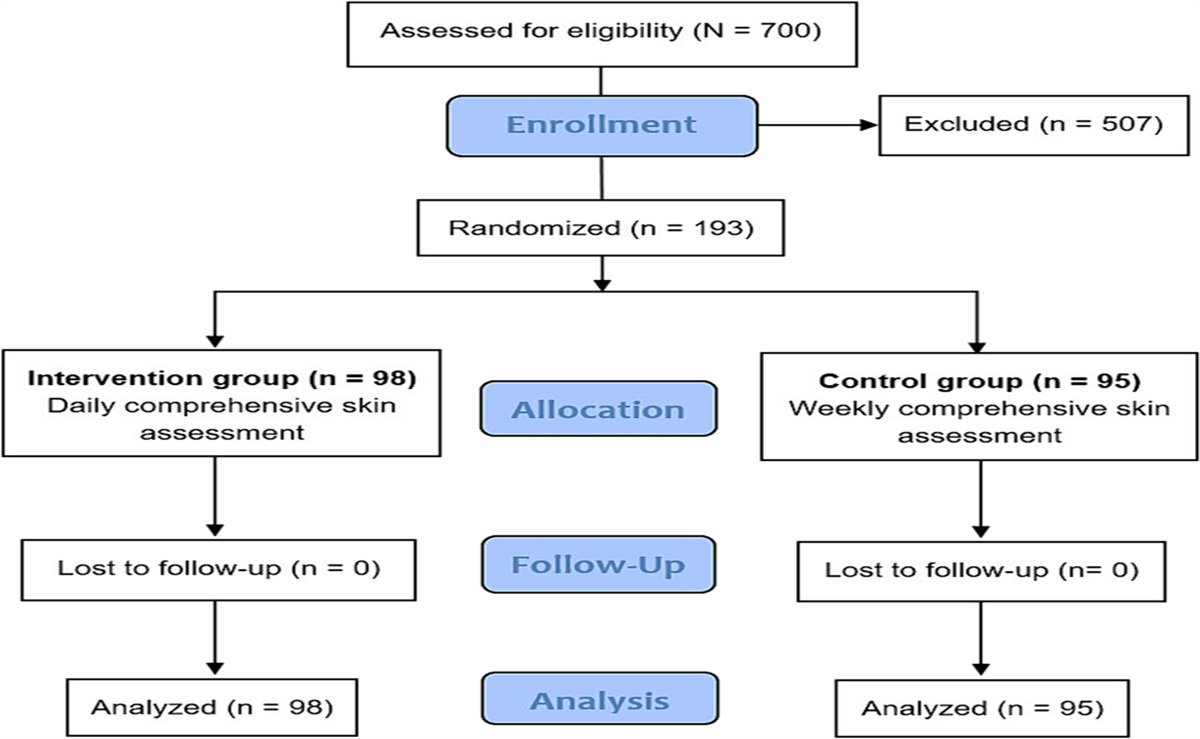
METHODS Design and SettingThis retrospective, cross-sectional study was conducted in the ICUs of a training and research hospital. The study population consisted of a total of 318 patients treated in the ICUs (neurology and respiratory diseases) over a 6-month period, from January to June 2022.
ParticipantsThe researchers first identified patients treated in the neurology and respiratory ICUs by searching the medical records through the hospital’s electronic system. Patients were included in the study if they (1) were 18 years or older, (2) did not have a PI or had a stage 1 PI at admission to the ICU, (3) scored 13 or lower on the Braden Scale (high risk), (4) were treated for 72 hours or longer, and (5) were regularly repositioned during their stay in the ICU. In line with standard intensive care procedure, patients in the ICUs at the study site were repositioned at 2-hour intervals to prevent PI development. However, patients with unstable hemodynamic parameters, including acute respiratory distress, spinal cord injury, or shunt surgery, cannot be repositioned. Only patients who could be repositioned regularly were included in the study to ensure homogeneity in the sample groups. Patients with stages 2, 3, and 4 and unstageable PIs and those with Braden Scale scores greater than 13 were excluded from the study. All patient data were recorded by the hospital’s electronic system and archive file scanning.
In the neurology ICU, a cream containing 40% zinc oxide and Hamamelis virginiana distillate with tissue shrinkage (astringent), local hemostatic, and anti-inflammatory effects is routinely used. The hospital wound care team began applying a cream containing zinc oxide in the first neurology ICU as a pilot wound care protocol, and barrier creams were used as part of a standard wound care protocol for protective purposes in other ICUs. Barrier creams used in the respiratory ICU contain two main active ingredients: allantoin and dimethicone. Other excipients of the barrier creams used in this study are vaseline, olive oil, mineral oils, monopropylene glycol, betaine, and D-panthenol.
Data in this study were collected at the time of this pilot implementation. The researchers selected the respiratory ICU for comparison because patients had similar mean ages and PI rates in both ICUs, and these data were accessible because the principal researcher had previously worked in this unit. Therefore, patients in the neurology ICU were included in group 1 (zinc oxide cream), and the patients in the respiratory ICU comprised group 2 (classic barrier cream).
Data CollectionIn both ICUs, nurses record sociodemographic characteristics of the patients and assess and stage PIs during hospitalization and at ICU discharge using the Pressure Ulcer Healing Assessment Scale (PUSH) and the PI classification guidelines developed by the National Pressure Injury Advisory Panel, European Pressure Ulcer Advisory Panel, and Pan Pacific Pressure Injury Alliance. Nurses evaluate ICU patients for PIs twice daily, in the morning and night shifts. Hence, researchers obtained this information from the patient files.
Pressure Ulcer Healing Assessment ScaleThe National Pressure Injury Advisory Panel initially developed this tool to monitor changes in PIs.18 It includes three subdimensions: tissue type, exudate amount, and area of the PI in centimeters squared (length × width). For tissue type, scores range from 0 to 4 (4 = necrotic tissue; 3 = no necrotic tissue, but there is crusting present; 2 = granulation present and the wound is clean; 1 = epithelialization; and 0 = wound is completely closed). In terms of exudate amount, no exudate is scored as 0 points, low is 1 point, medium is 2 points, and high is 3 points. The value obtained from the wound area is evaluated on a 10-point scale. Scores on the three subdimensions are totaled to create the overall PUSH score, which ranges from 0 to 17, with higher scores indicating greater wound severity.18,19
PI stagingAccording to the classification system, PIs are classified as stage 1, 2, 3, or 4, unstageable, or deep-tissue injury. Wound size and depth, wound edges, odor, exudate, infection, presence of tunnelling, and pain indicators were evaluated during classification.20
EthicsBefore beginning the study, permission was obtained from Sakarya University, Faculty of Medicine, Non-Interventional Ethics Committee (June 30, 2022; decision no. E-71522473-050.01.04-145940-176). The participating center granted access to medical electronic records and archive files. The first author had access to the patient data. To ensure anonymity, each patient record was assigned an ID number. The data were not copied from the patient files and stored elsewhere. The second author rechecked all data for accuracy. This study was performed in line with the principles of the Declaration of Helsinki.
Data AnalysisData were evaluated using SPSS 22 software (IBM Corp). The authors analyzed the descriptive characteristics of the sample by number, percentage distribution, mean, and SD. They used a χ2 test for between-group comparisons of categorical variables such as sex and intensive care treatment. Kurtosis and skewness values were examined to determine whether the research variables showed a normal distribution.21,22 Parametric methods were used in the analysis of the data. If the data were normally distributed, the means of continuous variables between the study groups were compared using an independent t test. Continuous variables were tested using the Pearson correlation analysis. The statistical significance level was accepted as P < .05.
RESULTSA total of 95 patients met the inclusion criteria, 48 in group 1 (zinc oxide cream) and 47 in group 2 (barrier cream; Table 1). Table 2 shows patients’ sociodemographic and clinical characteristics by group. In terms of the average length of hospital stay, patients in group 1 remained in the hospital longer on average than those in group 2 (group 1 mean, 22.77 [SD, 14.84] days vs group 2 mean, 13.66 [SD, 9.51] days; P = .040). The groups did not differ by age (group 1 mean, 71.71 [SD, 13.67] years vs group 2 mean, 68.64 [SD, 12.54] years; P = .482), Braden Scale score during hospitalization (group 1 mean, 9.94 [SD, 1.37] versus group 2 mean, 10.19 [SD, 1.03]; P = .075), PUSH score during hospitalization (group 1 mean, 3.19 [SD, 3.25] vs group 2 mean, 2.77 [SD, 2.98]; P = .463), sex (P = .475), or PI stage during hospitalization (P = .607). Regarding the initial PI stage at ICU admission, 47.9% of the patients in group 1 had no PIs, and 52% had a stage 1 PI. In comparison, 53% of the patients in group 2 had no PI, and 46.9% had a stage 1 PI.
Table 1. - INCLUSION CRITERIA FOR PARTICIPANT SELECTION (N = 95) Inclusion Criteria Group 1: Neurology ICU, n Group 2: Respiratory ICU, n Patients treated between January 1, 2022, and June 30, 2022 130 188 Patients with no PI or stage 1 PI 116 164 Patients with a Braden Scale score ≤13 76 98 Patients treated for ≥72 h 64 56 Patients repositioned at 2-h intervals 51 50 Patients with no missing health record data 48 47 Patients included in the study 48 47Abbreviation: PI, pressure injury.
Abbreviations: PI, pressure injury; PUSH, Pressure Ulcer Healing Assessment Scale.
aIndependent t test.
bPearson χ2 test.
At ICU discharge, the two groups differed in terms of mean PUSH score (Table 3). Whereas the mean PUSH score for group 1 was 3.83 (SD, 4.39), it was 6.79 (SD, 4.40) for group 2 (P < .001). Further, the groups also differed by PI stages at ICU discharge (P = .044), with more patients in group 2 having stages 2 and 3 PIs. In group 1, 10.4% of patients had a stage 2 PI and 4.2% had a stage 3 PI at discharge. In contrast, in group 2, 27.6% of patients had a stage 2 PI, and 8.5% had a stage 3 PI.
Table 3. - COMPARISON OF ZINC OXIDE CREAM AND BARRIER CREAM GROUPS ACCORDING TO DISCHARGE PUSH SCALE SCORE AND PI STAGE (N = 95) Variable Zinc Oxide Cream Group (n = 48), Mean ± SD or n (%) Barrier Cream Group (n = 47), Mean ± SD or n (%) Test Statistic P PUSH output total 3.83 ± 4.39 6.79 ± 4.40 −-3.237a <.001 PI stage at discharge 8.116b .044 No PI 21 (43.7) 10 (21.3) Stage 1 20 (41.7) 20 (42.6) Stage 2 5 (10.4) 13 (27.6) Stage 3 2 (4.2) 4 (8.5)Abbreviations: PI, pressure injury; PUSH, Pressure Ulcer Healing Assessment Scale.
aIndependent t test.
bPearson χ2 test.
An ideal topical agent would quickly heal wounds, reduce mortality and morbidity by preventing bacterial contamination and sepsis, and be easily accessible and inexpensive.23 Efforts are underway to discover the most suitable agent with these characteristics for preventing or improving PIs. Topical zinc in the form of zinc oxide or calamine lotion has been widely used in ICUs for many years to treat various types of wounds, including PIs, because of its anti-inflammatory and antimicrobial effects. However, it is essential for healthcare professionals to choose the most appropriate wound care product for patients to minimize pain, exudate, smell, stress, and anxiety while shortening recovery time. Therefore, this retrospective study aimed to compare the efficacy of zinc oxide and barrier creams for PI prevention. The results indicate that zinc oxide cream has more positive effects on preventing PIs than barrier cream in terms of PUSH scores and PI stages.
Previous research has shown that zinc-containing preparations support wound healing, control bacterial infection in the tissue area, and help granulation tissue form in the wound area.24 In a retrospective study evaluating the efficacy of dimethicone and zinc-based barrier cream compared with hyperoxygenated fatty acids in preventing PIs in patients at high or very high risk, the authors noted that the dimethicone and zinc-based barrier cream had a positive effect on preventing PIs in patients for 7 days, although there was no statistically significant difference between the groups.25 The topical application of zinc may reduce debris and necrotic material, increasing epithelialization and accelerating wound healing.25 In their meta-analysis Song et al26 evaluated the effectiveness of zinc therapy for PI treatment, reporting that patients who received a zinc supplement had improved PI healing and PUSH scores in comparison with those in the control group.
The majority of research examining zinc’s effects on wound healing has been carried out in animal models. Zinc oxide administered topically for 12 days was useful in treating full-thickness excisional wounds in rats, regardless of nutrition status.27 Arslan et al23 compared the effectiveness of zinc oxide and silver sulfadiazine in healing burn wounds in rabbits. They found that zinc oxide cream containing 20% zinc oxide and 80% petroleum jelly was more effective than silver sulfadiazine in the treatment of burns, in terms of epithelialization, epidermal maturation, and scar formation. Recently, studies evaluating the effectiveness of zinc oxide nanoparticles have gained attention. Zinc oxide nanoparticles have unique antibacterial properties that prevent wound infection by inhibiting the colonies of Staphylococcus aureus and Escherichia coli in wounds and supporting wound healing.23
Further, many previous studies that examined the effectiveness of zinc oxide creams for a variety of wound types were conducted with small samples and inconsistent in terms of methodology and generalizability of results. Chuangsuwanich et al28 compared two wound dressing protocols, alginate silver dressing and silver zinc sulfadiazine cream, in terms of PI healing and cost-effectiveness and reported that there were no significant between-group differences in PUSH score, wound size, or reduction in exudate volume. In addition, the tissue type score and treatment cost were found to be significantly lower in the alginate silver group. In a randomized controlled study, researchers compared the efficacy of topical streptokinase-streptodornase solution (Varidase) with that of zinc oxide on necrotic PIs. Necrotic tissue removal was observed in six patients (43%) treated with Varidase and seven patients (50%) treated with zinc oxide within 8 weeks. Although there was no significant difference between the two treatments, both topical applications were equally effective in treating necrotic tissue.29
Baatenburg de Jong and Admiraal17 compared the efficacy of Cavilon barrier film (3M) and zinc oxide oil in patients with at least moderate skin damage due to urinary incontinence. Using both products resulted in an improvement in skin condition at the end of 14 days. Those authors reported that the barrier film was more cost-effective because it required fewer applications and resulted in fast healing.17 Ramirez Razor et al30 compared two different zinc oxide-based skin ointments for the treatment of dermatitis associated with urinary or fecal incontinence. The intervention groups were administered a structured skin care regimen for 1 week with Calmoseptine ointment or Desitin maximum strength diaper rash paste. At the end of the study, a significantly higher number of participants in the Calmoseptine group as compared with the Desitin group completely recovered on day 6, and there was a greater reduction in the affected area on all the follow-up days.30 Similarly, Lian31 examined the use of barrier products to prevent and manage incontinence-associated dermatitis and found that there was no significant difference in efficacy between petrolatum, zinc oxide oil, and polymer-based barrier film and that polymer-based barrier film was more cost-effective than petrolatum or zinc oxide.
In their study comparing the efficacy of topical zinc oxide and honey barrier cream in individuals with inflammatory intertrigo, Nijhuis et al32 found no significant difference in the treatment effect between the intervention groups at the end of 21 days and noted that both methods could be used as an alternative to intertrigo treatment. Ågren et al33 compared the efficacy of topical zinc oxide in the secondary healing of pilonidal wounds. Although the closure time of open pilonidal wounds was shorter with zinc oxide treatment, the topical zinc oxide did not significantly accelerate healing.
A systematic review found that there was very low-quality evidence indicating that zinc-based compression bandages and topical zinc in combination with compression therapy are effective in healing venous leg ulcers.15 In addition, a meta-analysis comparing the efficacy of 13 different types of dressings (including hydrocolloids, alginates, protease modulating dressings, foams, contact layers, windings containing honey and cadexomer iodine, and saline gauze) and six topical agents (collagenase, silver sulfadiazine, zinc oxide, phenytoin, honey, and iodine) found that when combined with the risk of high bias the evidence was largely low or very low precision and that no generalization could be made in terms of the superiority of an agent.34
In the present study, use of a zinc-containing cream more effectively prevented PI than did the barrier cream. These results may differ from the previous literature because of greater PI awareness by healthcare professionals working in ICUs, the age of the patients, the length of hospital stay, and the differences in sample size. In addition, it is essential to understand comorbidities such as cardiovascular disease, diabetes, and neurodegenerative disorders, which are common in patients hospitalized in the ICU, and to consider conditions such as malnutrition, polypharmacy, incontinence, and immobility that may affect PI treatment. Further, the zinc oxide cream used in this study contains H virginiana as an excipient. The anti-inflammatory, antioxidant, and antiproliferative effects of H virginiana extracts may have increased the effectiveness of the zinc oxide on PI prevention and healing.35
LimitationsThe retrospective and cross-sectional design of this study is the most critical limiting factor. Zinc oxide cream is used only in a single ICU at the study hospital, leading to difficulty in obtaining complete patient records that met the inclusion criteria and thus limiting the sample size. In addition, significant risk factors for PI, such as comorbidity status and types of chronic diseases, intubation status, diet, and body mass index could not be examined. Laboratory findings such as hemoglobin, total protein, and albumin also were not evaluated.
CONCLUSIONSThe prevention and management of PIs require various approaches, including risk assessment, formulation of preventive measures, and interventions that promote wound healing. In this study, zinc oxide creams had more positive effects on healing PIs than barrier creams. However, there is a need for further research with a prospective, crossover design and larger samples; randomized controlled trials; and meta-analyses to determine if updates are needed in the current standard of care for the prevention or management of PIs in intensive care patients.
REFERENCES 1. Avci O. Evaluation of patients with pressure sores in the intensive care unit. Turk Clin J Nurs Sci 2019;11(3):239–44. 2. Coyer F, Miles S, Gosley S, et al. Pressure injury prevalence in intensive care versus non-intensive care patients: a state-wide comparison. Aust Crit Care 2017;30(5):244–50. 3. Lin FF, Liu Y, Wu Z, et al. Pressure injury prevalence and risk factors in Chinese adult intensive care units: a multi-centre prospective point prevalence study. Int Wound J 2022;19(3):493–506. 4. Tanrikulu F, Dikmen Y. Pressure injuries in intensive care patients: risk factors and precautions. J Hum Rhythm 2017;3(4):177–82. 5. Kurtuluş Tosun Z, Bölükbaşi RP. Pressure wound prevalence and affecting factors in elderly patients in intensive care units. J Intensive Care Nurs 2015;19(2):43–53. 6. Karaca Sivrikaya S, Sarikaya S. Yoğun Bakim Hastalarinda Basi Ülseri, Önleme Ve Hemşirelik Bakimi. Yoğun Bakim Hemşireliği Dergisi 2020;24(2):139–49. 7. Edsberg LE, Langemo D, Baharestani MM, Posthauer ME, Goldberg M. Unavoidable pressure injury: state of the science and consensus outcomes. J Wound Ostomy Continence Nurs 2014;41(4):313–34. 8. Gencer ZE, Ünal E, Özkan Ö. Basinç Ülserleri Tedavi Maliyetleri Etkililik Analizi; Konvansiyonel ve Modern Yara Bakim Tedavi Maliyetlerinin Karşilaştirilmasi. Akd Med J 2019;5(2):201–8. 9. Krzemińska S, Borodzicz A. Profilaktyka przeciwodleżynowa i metody prognozowania ryzyka rozwoju odleżyn w oddziałach intensywnej terapii. Pielęgniarstwo w Anestezjologii i Intensywnej Opiece 2016;2(4):117–24. 10. Ba P, Wendong C, Marcio M. Pressure ulcer history model to estimate the clinical impact of prevention and treatment interventions. THETA (Toronto Health Economics and Technology Assessment Collaborative). https://theta.utoronto.ca/publications-kt/reports#menu1. Last accessed September 20, 2023. 11. Australian Wound Management Association. Pan Pacific Guideline for the Prevention and Management of Pressure Injury (2012). https://www.awma.com.au/files/publications/2012_awma_pan_pacific_guidelines.pdf. Last accessed September 19, 2023. 12. Gupta P, Shiju S, Chacko G, et al. A quality improvement programme to reduce hospital-acquired pressure injuries. BMJ Open Qual 2020;9(3):e000905. 13. Tayyib N, Coyer F, Lewis PA. Implementing a pressure ulcer prevention bundle in an adult intensive care. Intensive Crit Care Nurs 2016;37:27–36. 14. Bliss DZ, Zehrer C, Savik K, Smith G, Hedblom E. An economic evaluation of four skin damage prevention regimens in nursing home residents with incontinence: economics of skin damage prevention. J Wound Ostomy Continence Nurs 2007;34(2):143–52. 15. O’Connor S, Murphy S. Chronic venous leg ulcers: is topical zinc the answer? A review of the literature. Adv Skin Wound Care 2014;27(1):35–44. 16. Lin P, Sermersheim M, Li H, Lee P, Steinberg SM, Ma J. Zinc in wound healing modulation. Nutrients 2018;10(1):16. 17. Baatenburg de Jong H, Admiraal H. Comparing cost per use of 3 M Cavilon No Sting Barrier Film with zinc oxide oil in incontinent patients. J Wound Care 2004;13(9):398–400. 18. Thomas D, Rodeheaver G, Bartolucci A, et al. Pressure Ulcer Scale for Healing: derivation and validation of the PUSH tool. The PUSH Task Force. Adv Wound Care 1997;10(5):96–101. 19. Stotts NA, Rodeheaver GT, Thomas DR, et al. An instrument to measure healing in pressure ulcers: development and validation of the Pressure Ulcer Scale for Healing (PUSH). J Gerontol A Biol Sci Med Sci 2001;56(12):M795–9. 20. European Pressure Ulcer Advisory Panel, National Pressure Injury Advisory Panel and Pan Pacific Pressure Injury Alliance. Prevention and Treatment of Pressure Ulcers/Injuries. Haesler E, ed. EPUAP/NPIAP/PPPIA; 2019. 21. Tabachnick BG, Fidell LS. Using Multivariate Statistics. 6th ed. Pearson; 2013. 22. George D, Mallery P. IBM SPSS Statistics 26 Step by Step: A Simple Guide and Reference (16th ed). Routledge; 2019 23. Arslan K, Karahan Ö, Okuş A, et al. Comparison of topical zinc oxide and silver sulfadiazine in burn wounds: an experimental study. Turk J Trauma Emerg Surg 2012;18(5):376–83. 24. Jones P, Williams D. The use and role of chain and its compounds in wound healing. Met Ions Biol Syst 2004;41:139–83. 25. Garcia-Carretero R, Ballesteros-Ubeda MV, Martínez-Alvarez A, Martinez-Gimeno ML. Retrospective cohort noninferiority analysis of barrier cream in preventing pressure injuries. Adv Skin Wound Care 2021;34(5):255–60. 26. Song YP, Wang L, Yu HR, et al. Zinc therapy is a reasonable choice for patients with pressure injuries: a systematic review and meta-analysis. Nutr Clin Pract 2020;35(6):1001–9. 27. Hallmans G, Lasek J. The effect of topical zinc absorption from wounds on growth and the wound healing process in zinc-deficient rats. Scand J Plast Reconstr Surg 1985;19(2):119–25. 28. Chuangsuwanich A, Chortrakarnkij P, Kangwanpoom J. Cost-effectiveness analysis in comparing alginate silver dressing with silver zinc sulfadiazine cream in the treatment of pressure ulcers. Arch Plast Surg 2013;40(5):589. 29. Ågren MS, Strömberg HE. Topical treatment of pressure ulcers. A randomized comparative trial of Varidase and zinc oxide. Scand J Plast Reconstr Surg 1985;19(1):97–100. 30. Ramirez Razor B, Buckley V, Quiambao P, Dofitas R, Baltazar W. Incontinence-Associated Dermatitis (IAD) Study: blinded assessment and treatment with chain oxide-based ointment. WCET J 2014;34(4):13–23. 31. Lian Y. Barrier products in the treatment of incontinence-associated dermatitis. Nurs Stand 2016;30(47):59–69. 32. Nijhuis W, Houwing R, van der Zwet W, Jansman F. A randomized trial of honey barrier cream versus chain oxide ointment. Br J Nurs 2012;21(20):9–10,12-3. 33. Ågren MS, Ostenfeld U, Kallehave F, et al. A randomized, double-blind, placebo-controlled multicenter trial evaluating topical zinc oxide for acute open wounds following pilonidal disease excision. Wound Repair Regen 2006;14(5):526–35. 34. Westby MJ, Dumville JC, Soares MO, Stubbs N, Norman G. Dressings and topical agents for treating pressure ulcers. Cochrane Database Syst Rev 2017;6(6):CD011947. 35. Cheesman MJ, Alcorn S, Verma V, Cock IE. An assessment of the growth inhibition profiles of Hamamelis virginiana L. extracts against Streptococcus and Staphylococcus spp. J Tradit Complement Med 2021;11(5):457–65.
留言 (0)