
Remember me







The excess glucose in the blood characteristic of diabetes mellitus (DM) causes complications such as diabetic foot syndrome (DFS) in the lower limb.1 The International Diabetes Federation, World Health Organization, International Working Group of the Diabetic Foot, Madrid Diabetic Association, and Spanish Diabetes Federation recommend the involvement of a multidisciplinary team and prevention to halt the progression of DM and its complications.2–6
Among the measures patients can use for self-management of complications is the frequent use of emollients to care for the skin on their feet.7 This recommendation stems from the knowledge that cutaneous xerosis of the feet is one of the most common conditions among patients with type 2 DM8 given the pathology-specific alterations in type I collagen formation,9,10 impaired keratinocyte proliferation, and migration9,11 and imbalance in natural moisturizing factors.12
Although skin problems are common in patients with type 2 DM, awareness and choice of treatment are commonly poor.13 However, skin dryness can be counteracted with moisturizers that strengthen the barrier function of impaired skin.14 Xerosis, if treated appropriately in early stages, can reduce morbidity in patients with DM and prevent complications including infection, ulceration, and gangrene that could lead to amputation.15
Urea, a natural hydrating agent, is part of the stratum corneum’s water-soluble fraction located in the outermost layer of the epidermis.16 Urea has multiple properties, most notably its ability to exert specific gene-regulatory activities affecting messenger RNA expression of certain genes, which play a role in keratinocyte differentiation, enhancing the skin’s protective barrier function.14 Urea may be part of a physically induced molecular biological network to promote healing mechanisms in various skin conditions.17 This molecule, in concentrations of 10% in combination with other molecules of similar characteristics, is effective in improving foot skin quality in patients with DM.18–20 Urea is a cornerstone for improving foot skin quality and the topical treatment and prevention of xerotic and hyperkeratotic skin conditions.21 Unfortunately, there are few studies investigating the skin of patients with DM,22–26 and existing findings are inconsistent.22
Therefore, the authors focused on determining the effects of specific foot creams containing 10% urea in patients with DFS. The objective was to evaluate the cost-effectiveness of two specific foot creams containing 10% urea available in pharmacies (higher-cost option) versus supermarkets (lower-cost option) in patients with DFS.
METHODSA prospective randomized clinical trial of analyzed data from 20 randomized feet belonging to 10 individuals was conducted in a specialized diabetic foot unit between November 2021 and April 2022. One investigator identified and invited patients to participate in the study, following their order of arrival at the unit. The local ethics committee approved the project protocol on October 14, 2021 (code 21/633-EC_X). The researchers complied with the ethical code of the Declaration of Helsinki, and all participants provided written, informed consent.
Inclusion criteria were patients 18 years or older with DFS manifesting as deep or superficial sensory impairment, neurologic involvement diagnosed by Semmes-Weinstein monofilament and Rydel-Seiffer tuning fork, metabolic syndrome, normal ankle-brachial index, and no cognitive impairment. Patients with hypersensitivity or allergy to any of the components of either cream were excluded.
Authors used data from studies previously conducted with the GRANMO sample size calculator to determine sample size. They calculated the means of two independent samples based on the primary quantitative variable and the primary scale for the risk assessment and skin quality of the foot skin of patients with DFS with a common SD of 1.5 and a minimum difference to be detected of 0.7. Based on this, a sample of 19 patients was necessary for a study power of 80.0% and a type 1 error of 5.0%, with a predictable dropout rate of 15.0%.
Based on the recruited sample (Figure 1), one researcher randomized feet into two groups using a simple randomization table. Participants and the evaluating researcher were blinded to group assignments. The creams were packaged in identical containers and dispensed to patients according to their assigned group. Another researcher provided the correct patient education materials based on group assignments.
 Figure 1.:
Figure 1.: STUDY FLOWCHART
The researchers expected to see improvement in skin quality in both groups, as both groups received a similar product with 10% urea indicated for this purpose. The evaluation of the skin changes was done by classifying each foot using the Questionnaire for the Evaluation of Injury Risk and Skin Quality of the Foot of the Patient with DFS (QERSQ; Figure 2), which uses a scale of 0 to 12 points to rate skin condition (0, adequate; 12, severe impairment). This questionnaire takes into account the characteristics of the skin of the foot and the guidelines used in dermatologic questionnaires for skin assessment. Intraobserver and interobserver validation (observers grouped according to training and experience) was carried out to ensure scientific rigor. The intraobserver Pearson correlation was 0.984, the senior interobserver Pearson correlation was 0.905, and the junior interobserver Pearson correlation was 0.334. Accordingly, when used by a provider with adequate training and experience, the QERSQ is considered valid. The QERSQ was not performed by novice raters in the present study: an experienced investigator specializing in the diabetic foot assessed study participants using the QERSQ tool.
 Figure 2.:
Figure 2.: QUESTIONNAIRE FOR EVALUATING THE RISK OF INJURY AND SKIN QUALITY OF THE FOOT OF THE PATIENT WITH DIABETIC FOOT SYNDROME
Investigators recorded data from two visits from each participant; visit 0 took place when the patient consented to participate in the study, and visit 1 took place 30 ± 2 days after visit 0. At visit 0, investigators collected baseline demographic data, a blinded researcher performed the first QERSQ assessment, and the patient received the corresponding material for each participating foot according to randomization. Participants were given a labeled cosmetic bag containing six prefilled syringes of cream A (purchased from a pharmacy) or cream B (purchased from a supermarket) to apply to each of their feet according to randomization. The patient was instructed to apply the assigned cream to the dorsum and sole of the designated foot at the rate of 2 mL per day for 30 days (Figure 3). The composition of both creams is as follows:
 Figure 3.:
Figure 3.: PREMEASURED MATERIAL DELIVERED TO THE PATIENT10% urea cream-prefilled syringes and kit.Abbreviations (in Spanish): PD, right foot; PI, left foot.
Cream A (pharmacy): aqua, glycerin, urea, cetearyl alcohol, sodium, lactate, caprylic-capric-triglyceride, ethylhexyl cocoate, hydrogenated coco-glycerides, octyldodecanol, microcrystalline wax, liquid paraffin, aluminum starch octenylsuccinate, dimethicone, sorbitan stearate, lactic acid, phenoxyethanol, peg-40 castor oil, sodium cetearyl sulfate, carbomer Cream B (supermarket): aqua, urea, glycerin, citric acid, liquid paraffin, cetearyl ethylhexanoate, cetearyl alcohol, glyceryl stearate, peg-100 stearate, shea butter, dimethicone, sodium hydroxide, avocado oil, tocopheryl acetate, tocopherol, microcrystalline wax, paraffin, parfum, acrylates/c10-30 alkyl acrylate crosspolymer, xanthan gum, caprylyl glycol, phenoxyethanol, citronellolAt visit 1, the patient returned the syringes received to assess adherence to the intervention. The same blinded researcher reassessed foot skin quality using the QERSQ During this visit, patients were also asked to complete a simple questionnaire for each foot, assessing their perceptions of the assigned cream in terms of odor, color, texture, absorption, and overall satisfaction, on a scale from 1 (dislike very much) to 10 (like very much).
Finally, after 3 months of follow-up, the blinded evaluating researcher surveyed participants (in person) to determine whether they had continued to adhere to the application of the cream as a preventive tool and their thoughts on the outcomes achieved.
Statistical analyses were performed using SPSS version 25.0 (IBM Corp). Descriptive analyses were performed. Means and SDs were calculated for quantitative variables as well as frequency distributions and percentages for qualitative variables. Statistical analysis was carried out to test for significant differences, taking into account their distribution using the Student t test or the Mann-Whitney U test; differences were considered statistically significant at P < .05 for a 95% CI.
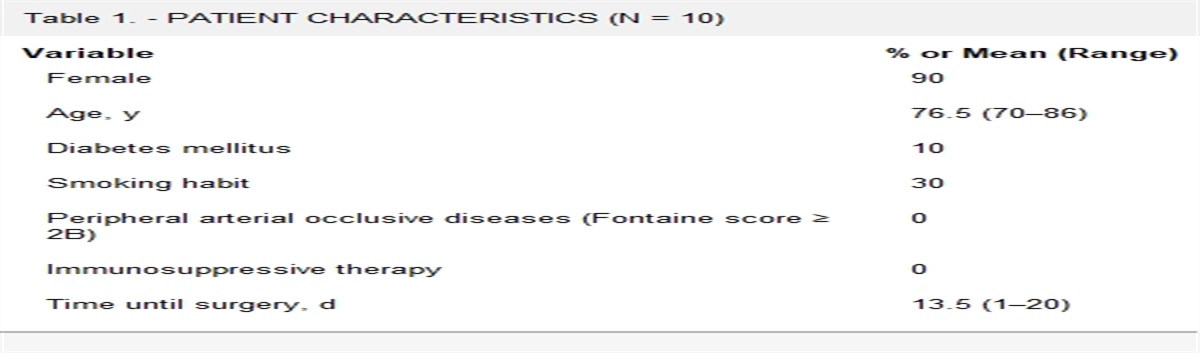
RESULTSThe skin quality of 20 feet belonging to 10 patients was assessed (Table 1). The skin quality of the participants’ feet was significantly improved (P < .001) between visit 0 and visit 1. The improvement scores obtained were 4.22 ± 2.72 points for the group that used the cream purchased in a pharmacy and 3.27 ± 2.14 points for the participants who used the cream purchased in a supermarket. These differences in improvement were not statistically significant between the two groups (P = .395). Although clinical improvement was observed in all participants, there was no appreciable between-group difference in skin quality. The improvement manifested visually as a decrease in xerosis and hyperkeratosis and reduced signs of injury risk, such as subkeratotic hematomas and dorsal redness of the toes (Figures 4 and 5). Participant scores for odor, color, texture, absorbency, and overall satisfaction did not differ significantly by cream (Table 2).
Table 1. - DESCRIPTIVE STATISTICS Variable Pharmacy Cream Group (n = 9), n (%) or Mean ± SD Supermarket Cream Group (n = 11), n (%) or Mean ± SD Male/female 2 (22.2)/7 (77.7) 3 (27.2)/8 (72.7) Age, y 74.3 ± 11.9 75.7 ± 11.5 Body mass index, kg/m2 28.5 ± 4.8 26.8 ± 5.2 Diabetes mellitus type 2 9 (100) 11 (100) Diabetes mellitus duration, y 15.3 ± 10.6 16.9 ± 9.8 Neuropathy 9 (100) 11 (100) Peripheral arterial disease 0 (0) 0 (0) High BP 6 (66) 9 (81) Hypercholesterolemia 7 (77) 9 (81) Wearing appropriate footweara 0 (0) 0 (0)aAppropriate footwear is understood as footwear that provides support on the back of the foot, has a rigid or semirigid counter, and has a sole of adequate thickness and appropriate material.
 Figure 4.:
Figure 4.: PATIENT SKIN CHANGES OVER TIMEA, Hyperkeratosis at the start of treatment. B, Reduced hyperkeratosis after 30 days of cream intervention. C, Xerosis at the start of treatment. D, Reduced xerosis after 30 days of cream intervention.Patients provided written consent for their images to be published.
 Figure 5.:
Figure 5.: REDUCTION OF THE SIGNS OF RISKA, Subkeratotic hematomas at the start of treatment. B, Decreased presence of subkeratotic hematomas after 30 days of cream intervention. C, Dorsal redness of the toes. D, Reduced dorsal redness of the toes after 30 days of cream intervention.
Table 2. - COMPARATIVE ANALYSIS OF THE TWO CREAMS Feature Evaluated Pharmacy Cream, Mean ± SD Supermarket Cream, Mean ± SD P Odor 6.88 ± 3.58 7.81 ± 3.28 .541 Color 7.77 ± 3.63 9.00 ± 3.00 .424 Texture 7.11 ± 3.55 6.27 ± 3.74 .580 Absorption 7.11 ± 3.55 7.09 ± 3.26 .903 Overall satisfaction 8.22 ± 3.34 8.45 ± 3.45 .763According to participant evaluations at the end of the cream application intervention, seven (70%) of the participants considered a single daily application of the product adequate to improve the quality of their skin on the foot. Regarding dosage, eight (80%) of the participants agreed that 2 mL for a single daily application was sufficient. Nine (90%) of the participants stated that their participation in this study helped them to initiate and maintain this preventive practice to improve the quality of their foot skin and avoid complications, and they plan to continue to use it in the future. All participants (100%) considered this a good preventive strategy to improve the quality of their foot skin and avoid complications. After analyzing the data showing improvement attributable to the active ingredient studied in this work, the authors recommended that all participants continue to use foot creams containing 10% urea in their formulation.
DISCUSSIONThe cost of the pharmacy cream was more than 10 times higher than the cost of the supermarket cream (€10.55/100 mL [USD $11.44/100 mL] vs €1.51/125 mL [USD $1.64/125 mL]). This would mean an annual cost of €73 (USD $79) for the use of pharmacy cream and a cost of €7.30 (USD $7.90) for the use of the supermarket cream. The nearly identical improvement in foot skin quality observed between the two groups showed that both creams were effective. Therefore, the authors believe that providers should direct patients to the lower-cost product to increase patient motivation and adherence to this preventive tool.
Economics can have a significant impact on patient adherence to preventive strategies. Considering that no statistically significant differences in efficacy were found between the two products, neither in the clinical improvement noted nor in the patient perception of the product, low-cost and readily accessible urea creams may be a useful, accessible, and affordable option to promote self-care among patients with DFS.
In the assessment of the characteristics of the creams, the overall scores were very similar, with no statistically significant differences in any of the categories assessed. Both creams contain similar ingredients, which is consistent with the similar efficacy noted.
The authors recommend 2 mL/d of creams including 10% urea as the recommended dosage and frequency to improve the foot skin quality of patients with DFS. However, because of the lack of previous studies evaluating the impact of multiple active ingredients available for skin care in patients with DFS, it would be productive to develop new studies in this line of research to provide more data in this regard. This lack of literature precludes comparisons among active ingredients or different products. Therefore, the authors encourage further research that could contribute to our understanding of improving foot skin quality and/or the impact that available DFS prevention and management tools can have on the incidence of related complications.
LimitationsThe characteristics of this study, aimed at patients with DFS, meant that all patients were older than 65 years and belonged to the same target population, which limits extrapolation of these study findings to other target populations. Additional study limitations included the lack of available literature and the limited mechanisms or tools to assess the impact of the active ingredients. The authors also could not determine what effect the inactive ingredients contained in the creams may have had. It would be interesting to investigate rigorous and reliable assessment tools to evaluate foot skin quality. Accordingly, the authors plan future work aimed to enhance available preventive tools for patients with DFS to improve clinical practice.
CONCLUSIONSThe cream containing 10% urea purchased in a supermarket showed the same effectiveness as a cream purchased in a pharmacy. Because both improve foot skin quality in patients with DFS and the pharmacy cream increases the cost of treatment, the authors recommend using the supermarket cream as a preventive tool.
REFERENCES 1. MedlinePlus. Diabetes mellitus. July 2023. https://medlineplus.gov/spanish/diabetes.html. Last accessed February 23, 2024. 2. Saeedi P, Petersohn I, Salpea P, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res Clin Pract 2019;157:107843. 3. World Health Organization. Diabetes datos y cifras. April 2023. www.who.int/es/news-room/fact-sheets/detail/diabetes. Last accessed February 23, 2024. 4. Schaper N, van Netten J, Apelqvist J, Bus C, Hinchliffe R, Lipsky B. IWGDF Practical guidelines on the prevention and management of diabetic foot disease. Diabetes Metab Res Rev 2020;36 Suppl 1:e3266. 5. Asociación Diabetes Madrid. Nuestra prevención en el cuidado de los pies. November 6, 2019. https://diabetesmadrid.org/nuestra-prevencion-en-el-cuidado-de-los-pies. Last accessed February 23, 2024. 6. Federación Española de Diabetes. Prevención Diabetes mellitus. Accessed October 15, 2020. https://www.fedesp.es/portal/1/main_noticias.aspx?idnoticia=2548&idportal=1. 7. van Netten JJ, Raspovic A, Lavery LA, et al. Prevention of foot ulcers in the at-risk patient with diabetes: a systematic review. Diabetes Metab Res Rev 2020;36(S1):1–22. 8. Lechner A, Akdeniz M, Tomova-Simitchieva T, et al. Comparing skin characteristics and molecular markers of xerotic foot skin between diabetic and non-diabetic subjects: an exploratory study. J Tissue Viability 2019;28(4):200–9. 9. De Macedo GMC, Nunes S, Barreto T. Skin disorders in diabetes mellitus: an epidemiology and physiopathology review. Diabetol Metab Syndr 2016;8(1):63. 10. Singh N. Preventing foot ulcers in patients with diabetes. JAMA 2005;293(2):217. 11. Blakytny R, Jude EB. Altered molecular mechanisms of diabetic foot ulcers. Int J Low Extrem Wounds 2009;8(2):95–104. 12. Rawlings AV, Harding CR. Moisturization and skin barrier function. Dermatol Ther 2004;17(s1):43–8. 13. Legiawati L, Bramono K, Indriatmi W, et al. Oral and topical Centella asiatica in type 2 diabetes mellitus patients with dry skin: a three-arm prospective randomized double-blind controlled trial. Evid Based Complement Alternat Med 2020;2020:1–13. 14. Grether-Beck S, Felsner I, Brenden H, et al. Urea uptake enhances barrier function and antimicrobial defense in humans by regulating epidermal gene expression. J Invest Dermatol 2012;132(6):1561–72. 15. Pendsey S. Understanding diabetic foot. Int J Diabetes Dev Ctries 2010;30(2):75. 16. Celleno L. Topical urea in skincare: a review. Dermatol Ther 2018;31(6):e12690. 17. Dirschka T. Mode of action of urea. Int J Clin Pract 2020;74(S187). 18. Symmers WStC, Kirk TS. Urea as a bactericide, and its application in the treatment of wounds. Lancet 1915;186(4814):1237–9. 19. Kligman AM. Dermatologic uses of urea. Acta Derm Venereol 1957;37(2):155–9. 20. Lacarrubba F, Nasca MR, Puglisi DF, Micali G. Clinical evidences of urea at low concentration. Int J Clin Pract 2020;74(S187). 21. Micali G, Lacarrubba F. Optimising the use of urea in dermatology. Int J Clin Pract 2020;74(S187). 22. Behm B, Schreml S, Landthaler M, Babilas P. Skin signs in diabetes mellitus: skin signs in DM. J Eur Acad Dermatol Venereol 2012;26(10):1203–11. 23. Sakai S, Kikuchi K, Satoh J, Tagami H, Inoue S. Functional properties of the stratum corneum in patients with diabetes mellitus: similarities to senile xerosis. Br J Dermatol 2005;153(2):319–23. 24. Seirafi H, Farsinejad K, Firooz A, et al. Biophysical characteristics of skin in diabetes: a controlled study. J Eur Acad Dermatol Venereol 2009;23(2):146–9. 25. Yoon HS, Baik SH, Oh CH. Quantitative measurement of desquamation and skin elasticity in diabetic patients. Skin Res Technol 2002;8(4):250–4. 26. Yosipovitch G, Tur E, Cohen O, Rusecki Y. Skin surface pH in intertriginous areas in NIDDM patients: possible correlation to Candidal intertrigo. Diabetes Care 1993;16(4):560–3.
Comments (0)