
Remember me



Workplace violence (WPV) against healthcare workers is a serious occupational hazard that negatively impacts their productivity, job satisfaction, retention, and quality of patient care.1-4 Although WPV can be prevented, the incidence has increased steadily over the last decade. In a national survey of 7399 nurses working in acute care hospitals, 72% experienced at least 1 WPV in the previous year, mainly from patients and visitors: verbal abuse (65%), physical assault (28%), and sexual harassment (13%).5 According to the US Bureau of Labor Statistics, hospital workers are 6 times more likely to experience WPV-related nonfatal injuries than all workers.6 Despite the extent of violence and its significance, 88% of 2010 healthcare workers who experienced WPV did not file formal incident reports in a healthcare system database, whereas fewer than half had reported informally to their supervisors.7 In another study, half of the nurses did not know what types of violence to report because they believed only assaults with sustained physical injuries should be reported.8 Various factors may contribute to the underreporting: misperception that “it is part of the job,” nature of patient medical conditions, inconsistent and time-consuming incident report system, fear of retaliation from the management, perception of lack of management accountability and follow-up, and unclear definition of WPV.2,9,10 Thus, underreporting may misrepresent the true magnitude of WPV and hinder the prevention effort.
Many governing bodies have promulgated laws and requirements to reduce the violence against healthcare workers. In 2021, The Joint Commission published the R3 Report of the new and revised WPV Prevention Standards in 3 domains for all Joint Commission–accredited hospitals, effective January 1, 2022.11 The leadership domain requires establishing a WPV prevention program with 1 designated leader and a multidisciplinary team. The human resource domain includes providing resources, training, and education to leadership, staff, and licensed practitioners as a part of the WPV prevention program. The environment of care domain includes 3 requirements: analyzing the worksite and WPV incidents annually; establishing processes for continuous monitoring, reporting, and investigating of WPV; and reporting and investigating WPV based on the established processes. The Joint Commission rationalized that the standardized methods of collecting and reporting WVP incidents could make it possible to accurately measure the effectiveness of prevention programs and allow hospitals to improve such programs continuously.
The State of California passed a law requiring hospitals to implement a WPV prevention plan in 2014.12 The WPV was defined as the “use of physical force against a hospital employee” or the use of weapons regardless of injury. Hospitals are required to report all violent incidents to the California Division of Occupational Safety and Health, which in turn is required to post the information on its website. However, an analysis of the past 3-year public database indicates considerable variation in data collection and reporting practice among hospitals.13 The authors identified inconsistent reporting of WVP incidents as a major problem in assessing the effectiveness of preventive measures.
Various strategies have been recommended to prevent and manage violent behaviors. These include screening and flagging potentially violent patients, activating behavior response teams, staff education and training, and postassault debriefing.14-16 A Cochrane review of staff education and training studies showed no significant direct effects on the incidence of patient violence, although educational programs may have improved knowledge and attitudes among healthcare workers.17 Another Cochrane review that included interventional studies from 2 psychiatric units and an emergency department showed that regular violence-risk assessments reduced aggression against healthcare workers.18 However, bundled multicomponent violence-reduction programs, such as policy and environmental changes and staff training, did not reduce overall aggression rates. These Cochrane reviews concluded that there is a need for standardized and validated violence frequency measures that also collect violence intensities.
In the new and revised WPV Prevention Standards, The Joint Commission defined WPV as “an act or threat occurring at the workplace that can include any of the following: verbal, nonverbal, written, or physical aggression; threatening, intimidating, harassing, or humiliating words or actions; bullying; sabotage; sexual harassment.”11 As more organizations implement standardized processes to collect and report WPV, The Joint Commission expects hospitals to implement performance benchmarks and evaluate the efficacy of preventive programs, further enabling adjustments to improve the results. Such a process should include a standardized tool to collect the various types of WPV as defined by The Joint Commission and the violence intensities. The Violent Event Severity Tool (VEST) was developed to address these needs. This study aimed to explore: 1) the perceived utility of the VEST and WPV prevention programs; 2) the severity of various violent events and incident reporting; and 3) the predictors of physical assault and sexual harassment among nurses.
Methods Study Design and ParticipantsA cross-sectional survey was conducted among healthcare workers attending the 2022 ANCC National Magnet® conference and ANCC® Pathway to Excellence® conference in Philadelphia, Pennsylvania, October 12 to 15, 2022. Healthcare workers visiting the exhibit hall were invited to participate in the study.
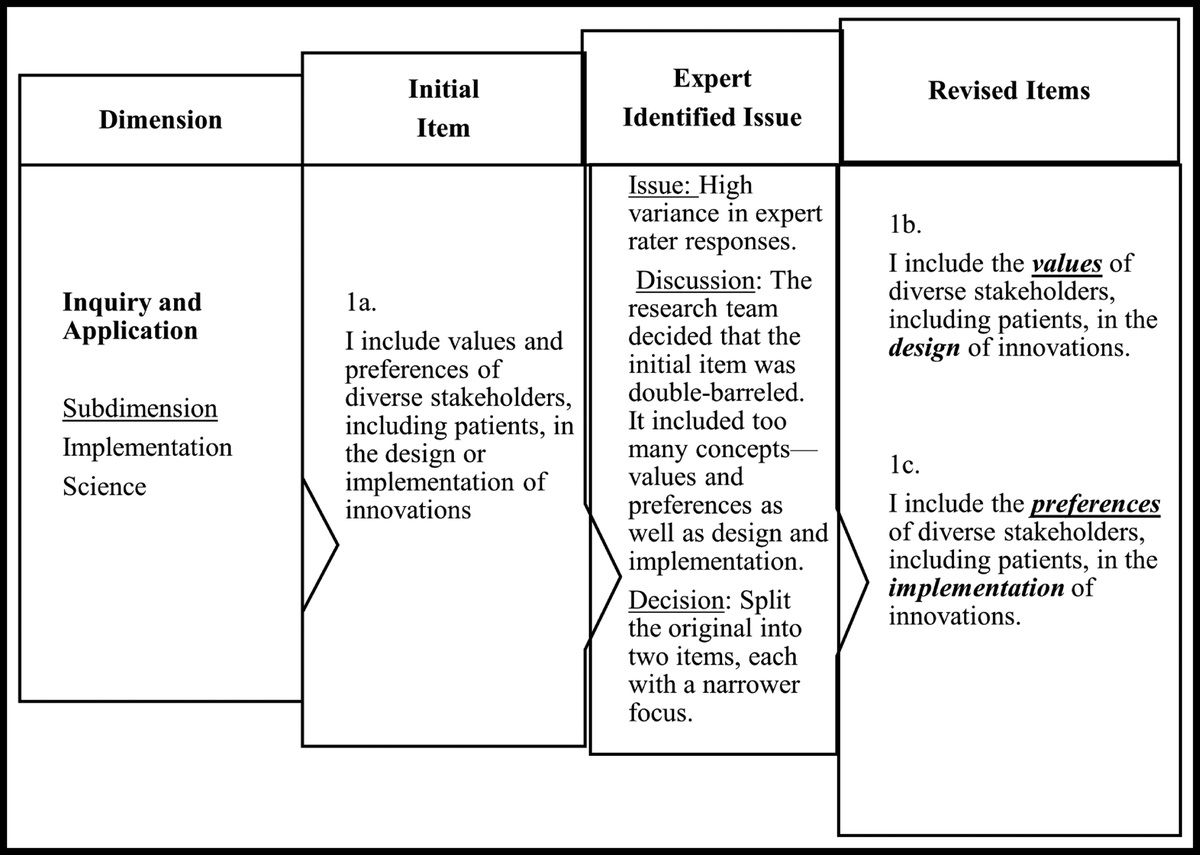
InstrumentsThe study survey included the VEST, 12 questions regarding participants' perceptions, and demographic data. The VEST comprises operational definitions of 6 types of patient violence based on the literature review and The Joint Commission's standards: physical assault, sexual harassment, physical threat, verbal threat, written threat, and verbal abuse. The 1st 5 types of patient violence include 4 severity grades: mild, moderate, severe, and life-threatening severities with assigned numerical grades of 1, 2, 3, and 4, respectively. For example, physical assault refers to violence involving physical contact with intent to cause bodily harm. Grade 1 physical assault is associated with no physical injury, whereas grade 4 is associated with life-threatening physical injury. The 6th type, verbal abuse, includes only grades 1 to 3 severity. This grading system is analogous to that used to collect and report drug adverse effects.19 The 1st author with expertise in instrument development and WPV drafted the VEST. A clinician with expertise in drug adverse effects performed face validity testing.
For the content validity testing, the VEST was submitted to a panel of 9 nurse educators with expertise in patient care at acute care hospitals to ensure that the violence types and severity grade definitions are relevant. They rated the degree of relevance on a 4-point Likert scale, ranging from 1 (not relevant) to 4 (highly relevant). The content validity index (CVI) assessed agreement among the panel members, with CVI ≥80% considered acceptable. Some definitions were reworded based on the CVI and the panel's comments. For example, verbal threat initially did not have grade 4 severity but was added according to the recommendation of an expert in behavioral and mental health. After the content validity testing, another group of clinicians in an acute care hospital reexamined the VEST, resulting in further rewording and clarification of the several definitions.
The 12 questions in the survey probed participants' perceptions over 4 pertinent topics. The 1st topic asked about the VEST's ease of use, applicability, and usefulness on the 5-point Likert scale, ranging from 1 (strongly disagree) to 5 (strongly agree). The 2nd topic asked the participants whether they filed an incident report on their worst patient-violence experience and to rate their satisfaction with the incident report filing process and follow-up. The 3rd topic was the proactive identification of potentially violent patients, a computerized search of patients' electronic health records (EHRs) for prior violence, and automated notification of potentially violent patients. The final topic was the participants' perceptions of their organization's WPV prevention program, satisfaction, and protection from patient violence. Demographic data were also collected, including age, gender, ethnicity, educational background, professional role, workplace, and years of work experience.
Data Collection ProceduresThe university's institutional review board and conference leaders reviewed and approved this study. A waiver of signed informed consent was granted because there were minimal risks involved in this anonymous survey. Participants were informed about the nature of the study and asked to fill out the survey if they agreed to participate. They were reminded of their voluntary participation and that they could withdraw from the study without any penalty. Completion of the survey indicated consent to the study.
Data AnalysisDescriptive statistics were performed to assess the sample characteristics and types and severities of the patient violence experienced by the participants. In this study, the grades 2 to 4 physical assault and sexual harassment were used as dependent variables because they involve physical injury and physical contact, respectively. To explore the predictors of the dependent variables, these grades and the demographic variables were recoded as dichotomous variables (grades ≥2 = “1”; none or grade 1 = “0”). Bivariate Kendall's τ tests were performed to explore the correlations between the dichotomous dependent and demographic variables. The statistically significant demographic variables from Kendall's τ tests were entered into multivariate logistic regression procedures with backward elimination to explore predictors of physical assault and sexual harassment. The SPSS version 29.0 (IBM Corp, Armonk, New York) was used for all data analyses. The 2-sided significance level was set at P < 0.05.
Results Sample CharacteristicsTable 1 describes the sample characteristics. The average age was 42 years, and most were female (80.2%). A majority were Caucasians (59.4%), were clinical nurses (53.1%), had baccalaureate degrees (53.1%), and worked in the emergency department (59.4%). The average work experience was 12 years, and most participants experienced patient violence (93.8%).
Table 1 - Sample Characteristics (N = 96) n (%) Age, mean (range), y 42 (20-63) Gender Male 18 (18.8) Female 77 (80.2) Ethnicity Caucasian 57 (59.4) Hispanic 10 (10.4) Asian/Pacific Islander 14 (14.6) African American 9 (9.4) Multiethnic/other 6 (6.2) Educational background BSN 51 (53.1) MSN 25 (26.0) Other master's degree 5 (5.2) Diploma/associate degree 7 (7.3) PhD/DNP 5 (5.2) Other 2 (2.1) Professional role Clinical nurse 51 (53.1) Nurse manager 21 (21.9) Director 6 (6.3) Educator 3 (3.1) CNO/leadership 5 (5.2) Other 9 (9.3) Workplace unit Emergency departments 57 (59.4) Medical-surgical units 10 (10.4) Critical care/step-down units 13 (13.6) Psychiatric units 6 (6.3) Pediatric units 2 (2.1) Perioperative unit/recovery units 4 (4.2) Other 3 (3.1) Work experience, mean (range), y 12 (1-40) Experienced patient violence 90 (93.8)Abbreviations: CNO, chief nursing officer; DNP, doctor of nursing practice.
Values are expressed as n (%) unless otherwise indicated. The percentage may not add up to 100% because of missing data or rounding.
Most participants agreed or strongly agreed that the VEST is easy to use (79.0%), as well as relevant (85.4%) and useful (85.2%) in reporting violent events. Most participants also agreed that proactive identification of patients (82.5%) and an automated notification (84.5%) could prevent or reduce the severity of patient violence. However, only 36% felt adequately protected from patient violence at their workplace. A majority reported that their organization has a WPV prevention program (75.3%), but only 43.3% were satisfied or very satisfied with their program.
The Severity of Violent Events and Incident ReportingFigure 1 depicts the 6 types of patient violence and their severity. A majority of participants experienced grades 2 to 4 violent events, including physical assault (51.6%), physical threat (65.0%), verbal threat (69.0%), and verbal abuse (69.1%). In contrast, only a minority experienced grades 2 to 4 written threat (16.5%) or sexual harassment (25.8%). Of the participants experiencing patient violence, only 55.6% filed an incident report. Figure 2 shows the percentages of incident report filing at various severity of physical assault (Figure 2A) and sexual harassment (Figure 2B). Among the participants who experienced grade 1 physical assault, only 38% filed an incident report. However, as the severity of the physical assault increased, the percentage who filed incident reports also increased with 70% and 100% filing for grades 3 and 4, respectively. Similarly, only 47% of participants reporting grade 1 sexual harassment filed an incident report, whereas the filing increased as the severity of harassment increased, with 80% and 100% filing for grades 3 and 4, respectively. Among those who filed an incident report, only 45% were satisfied or very satisfied with the filing process, with 38% being satisfied with their organization's follow-up after the incident.
 Figure 1:
Figure 1: Type and severity of violent events experienced by participants.
 Figure 2:
Figure 2: Incident reports filed versus severity of the physical assault and sexual harassment.
Predictors of Physical Assault and Sexual HarassmentBivariate Kendall's τ correlations between demographic variables and the dependent variables were performed. For the physical assault, working in critical care/step-down units correlated positively, whereas age correlated negatively. For the sexual harassment, working in critical care/step-down or psychiatric units correlated positively, but working in the emergency department correlated negatively. Table 2 shows the results of multivariate logistic regression procedures to explore the predictors of physical assault and sexual harassment. For the physical assault, working as clinical nurse was a significant positive predictor (odds ratio [OR], 3.17; 95% confidence interval [CI], 1.10-9.19), whereas age (OR, 0.94; 95% CI, 0.89-0.99) and working in medical-surgical units (OR, 0.13; 95% CI, 0.02-0.72) were significant negative predictors. For the sexual harassment, working in critical care/step-down units (OR, 8.00; 95% CI, 2.08-30.7) and psychiatric units (OR, 8.00; 95% CI, 1.32-48.5) were significant positive predictors.
Table 2 - Predictors of Physical Assault or Sexual Harassment OR 95% CI a P Physical assault (grades 2-4) Age 0.94 0.89-0.99 0.031 Clinical nurse 3.17 1.10-9.19 0.033 Critical care/step-down units 7.13 0.77-66.2 0.084 Medical-surgical units 0.13 0.02-0.72 0.019 Sexual harassment (grades 2-4) Critical care/step-down units 8.00 2.08-30.7 0.002 Psychiatric units 8.00 1.32-48.5 0.024aBy multivariate logistic regression.
The VEST appears to be a useful and relevant tool for standardized collection and reporting of various types and intensities of WPV. The use of the VEST would help healthcare organizations meet the new and revised Joint Commission requirements to implement standard processes for “continually monitoring, internally reporting, and investigating” WPV. The VEST would further facilitate organizations to benchmark and evaluate the efficacy of their WPV prevention programs through consistent measurement of the relevant endpoints, such as violent incidents and their severities. Finally, the tool would support compliance with the external governing body mandates and promote transparency through standardized reporting of WPV.
Incorporating the VEST into EHR could allow the simple and easy collection of WPV regularly as a part of routine nursing assessments. Our previous studies of patient violence in medical-surgical units and emergency departments indicated that the violence occurs in 1% to 3% of the patients.20,21 For nonviolent patients, the VEST can be completed quickly by responding “no” to the 1st question of whether any violent event has occurred. Therefore, the documentation burden of the VEST would be minimal for nonviolent patients. For the 1% to 3% of patients with violent incidents, the reporting nurses would 1st select the relevant type(s) of violence observed and then check off the appropriate severity of the incident. Thus, the VEST can be completed in 1 to 2 minutes for most of the violent incidents.
The violence severity grading system in the VEST appears to be valid for physical assault and sexual harassment as shown by the analysis of incident report filing versus the severity grades. As the VEST-defined violence grade increased from grade 1 to grade 4, increasing proportion of participants perceived violence to be serious enough to file an incident report, which supports the validity of the VEST severity grading system. In this study, as the violence severity increased from grade 1 to grade 4, the proportion of participants who filed incident reports increased monotonically from 38% to 100% for physical assault and from 47% to 100% for sexual harassment.
The current study findings further indicate that only a minority of the participants felt adequately protected from violence in their organization, and fewer than half were satisfied with their WPV prevention programs. This perception of low organizational support is consistent with a previous national survey of nurses, in which fewer than half felt that their organization valued employees' health and safety.5 These poor perceptions are likely due to a lack of effective WPV prevention programs that garner strong staff engagement. A recent study of a comprehensive, multicomponent bundled violence reduction program in a psychiatric emergency department showed a reduction in assaults following the implementation.15 Nevertheless, during the early phases of the program implementation, there was an apparent increase in assaults, which may have been due to heightened awareness of WPV. Interestingly, the staff reported that the most effective component of the program was flagging patients based on high-risk scores from a violence risk-screening tool.
Using a validated risk-screening tool may assist staff in identifying patients at high risk for violence and allow the implementation of focused, preemptive violence prevention measures. In our previous studies, Aggressive Behavior Risk Assessment Tool (ABRAT) was effective in identifying potentially violent patients with satisfactory sensitivities and specificities in acute care medical-surgical units and emergency departments.20,21 Focusing preventive interventions on a small fraction of the patients at high risk of violence could allow better resource utilization than an indiscriminate, universal precaution recommended by the Occupational Safety and Health Administration.22 Thus, a combined use of a validated screening tool, such as ABRAT, and a standardized tool for collecting violent incidents (eg, VEST) could facilitate the implementation of a standardized process for continual monitoring, analyzing, and reporting of WPV and an organization's prevention programs.
Surprisingly, healthcare workers in critical care or step-down units were 8-fold as likely to experience sexual harassment, similar to those in psychiatric units. Even though this result was statistically significant, it should be taken as preliminary because only 16% of the participants worked in critical care or step-down units. As expected, the participants' age was a significant negative predictor of physical assault, with each year of age associated with 6% lower odds of physical assault. Nurses with longer clinical experience may be better able to handle violent patients and avoid violent incidents.
LimitationsThere are several limitations to this study. First, the study was conducted among Magnet conference attendees visiting the exhibit hall. Thus, the highly selected nature of the conference attendees and self-reported survey responses may have introduced bias, and the results may not be generalizable to other healthcare workers. Second, the retrospective collection of the violent event experienced by the participants and its severity may have resulted in recall bias. Third, it is likely that the small sample size in this study reduced the statistical power to detect any additional predictors of the violent events. Finally, the relationship between the predictors and violent events in this cross-sectional study should not be taken as a cause-and-effect relationship. Further studies are needed to assess the utility of the VEST in collecting violent event types and severity data and its usefulness in evaluating the efficacy of violence prevention and mitigation programs.
ConclusionsThe VEST appears to be a useful and relevant tool for standardized collecting and reporting various types and intensities of violence. The VEST may help organizations comply with the new and revised Joint Commission requirements and implement standardized processes for monitoring WPV incidents. Future studies of the VEST incorporated into EHR and its use to examine the efficacy of violence prevention and mitigation programs are needed.
References 1. Gates DM, Gillespie GL, Succop P. Violence against nurses and its impact on stress and productivity. Nurs Econ. 2011;29(2):59–66 quiz 67. 2. Phillips JP. Workplace violence against health care workers in the United States. N Engl J Med. 2016;374(17):1661–1669. 3. Zhao SH, Shi Y, Sun ZN, et al. Impact of workplace violence against nurses' thriving at work, job satisfaction and turnover intention: a cross-sectional study. J Clin Nurs. 2018;27(13–14):2620–2632. 4. Arnetz JE, Arnetz BB. Violence towards health care staff and possible effects on the quality of patient care. Soc Sci Med. 2001;52(3):417–427. 5. Ulrich B, Cassidy L, Barden C, et al. National nurse work environments—October 2021: a status report. Crit Care Nurse. 2022;42(5):58–70. 6. US Bureau of Labor Statistics. Fact sheet. Workplace violence in healthcare 2018. April 8, 2020 https://wwwblsgov/iif/factsheets/workplace-violence-healthcare-2018htm. Accessed January 10, 2023. 7. Arnetz JE, Hamblin L, Ager J, et al. Underreporting of workplace violence: comparison of self-report and actual documentation of hospital incidents. Workplace Health Saf. 2015;63(5):200–210. 8. Song C, Wang G, Wu H. Frequency and barriers of reporting workplace violence in nurses: an online survey in China. Int J Nurs Sci. 2021;8(1):65–70. 9. Arnetz JE. The Joint Commission's new and revised workplace violence prevention standards for hospitals: a major step forward toward improved quality and safety. Jt Comm J Qual Patient Saf. 2022;48(4):241–245. 10. Morphet J, Griffiths D, Innes K. The trouble with reporting and utilization of workplace violence data in health care. J Nurs Manag. 2019;27(3):592–598. 11. The Joint Commission. R3 Report Issue 30: workplace violence prevention standards. 2021. https://www.jointcommission.org/standards/r3-report/r3-report-issue-30-workplace-violence-prevention-standards/. Accessed January 3, 2023. 12. California Legislative Information. SB-1299 Workplace violence prevention plans: hospitals (2013-2014). https://leginfo.legislature.ca.gov/faces/billNavClient.xhtml?bill_id=201320140SB1299. Accessed February 3, 2023. 13. Odes R, Chapman S, Ackerman S, et al. Differences in hospitals' workplace violence incident reporting practices: a mixed methods study. Policy Polit Nurs Pract. 2022;23(2):98–108. 14. Ferron EM, Kosny A, Tonima S. Workplace violence prevention: flagging practices and challenges in hospitals. Workplace Health Saf. 2022;70(3):126–135. 15. Okundolor SI, Ahenkorah F, Sarff L, et al. Zero staff assaults in the psychiatric emergency room: impact of a multifaceted performance improvement project. J Am Psychiatr Nurses Assoc. 2021;27(1):64–71. 16. Wong AH, Ray JM, Cramer LD, et al. Design and implementation of an agitation code response team in the emergency department. Ann Emerg Med. 2022;79(5):453–464. 17. Geoffrion S, Hills DJ, Ross HM, et al. Education and training for preventing and minimizing workplace aggression directed toward healthcare workers. Cochrane Database Syst Rev. 2020;9(9):CD011860. 18. Spelten E, Thomas B, O'Meara PF, et al. Organisational interventions for preventing and minimising aggression directed towards healthcare workers by patients and patient advocates. Cochrane Database Syst Rev. 2020;4(4):CD012662. 19. US Department of Health and Human Services. Common Terminology Criteria for Adverse Events. 2017. https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/ctcae_v5_quick_reference_5x7.pdf. Accessed February 1, 2023. 20. Kim SC, Ideker K, Todicheeney-Mannes D. Usefulness of Aggressive Behaviour Risk Assessment Tool for prospectively identifying violent patients in medical and surgical units. J Adv Nurs. 2012;68(2):349–357. 21. Kim SC, Kaiser J, Bulson J, et al. Multisite study of Aggressive Behavior Risk Assessment Tool in emergency departments. J Am Coll Emerg Phys Open. 2022;3(2):e12693. 22. Occupational Safety and Health Administration. Guidelines for preventing workplace violence for healthcare and social service workers. 2016. https://www.osha.gov/sites/default/files/publications/osha3148.pdf. Accessed December 17, 2022.
Comments (0)