
Remember me
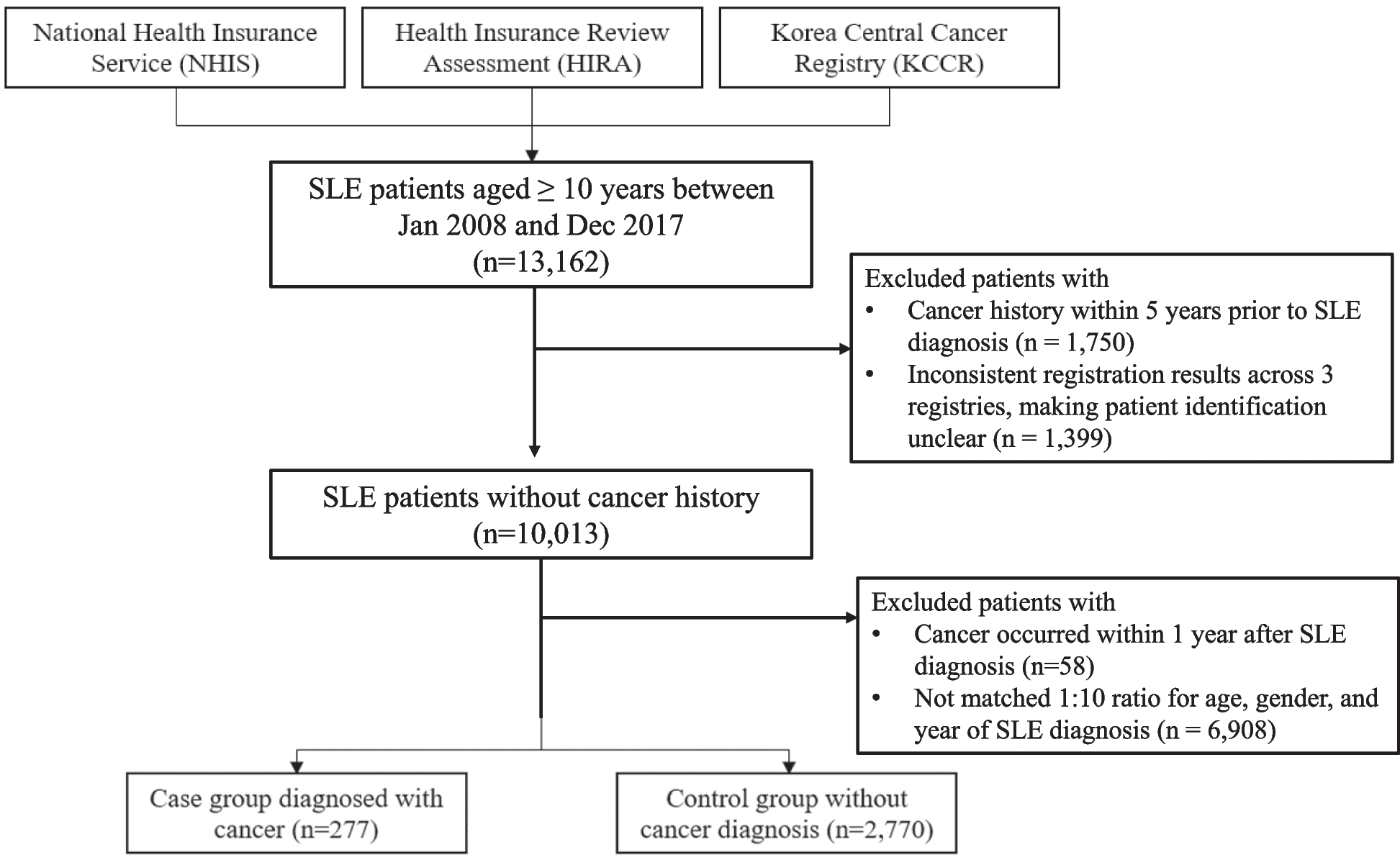


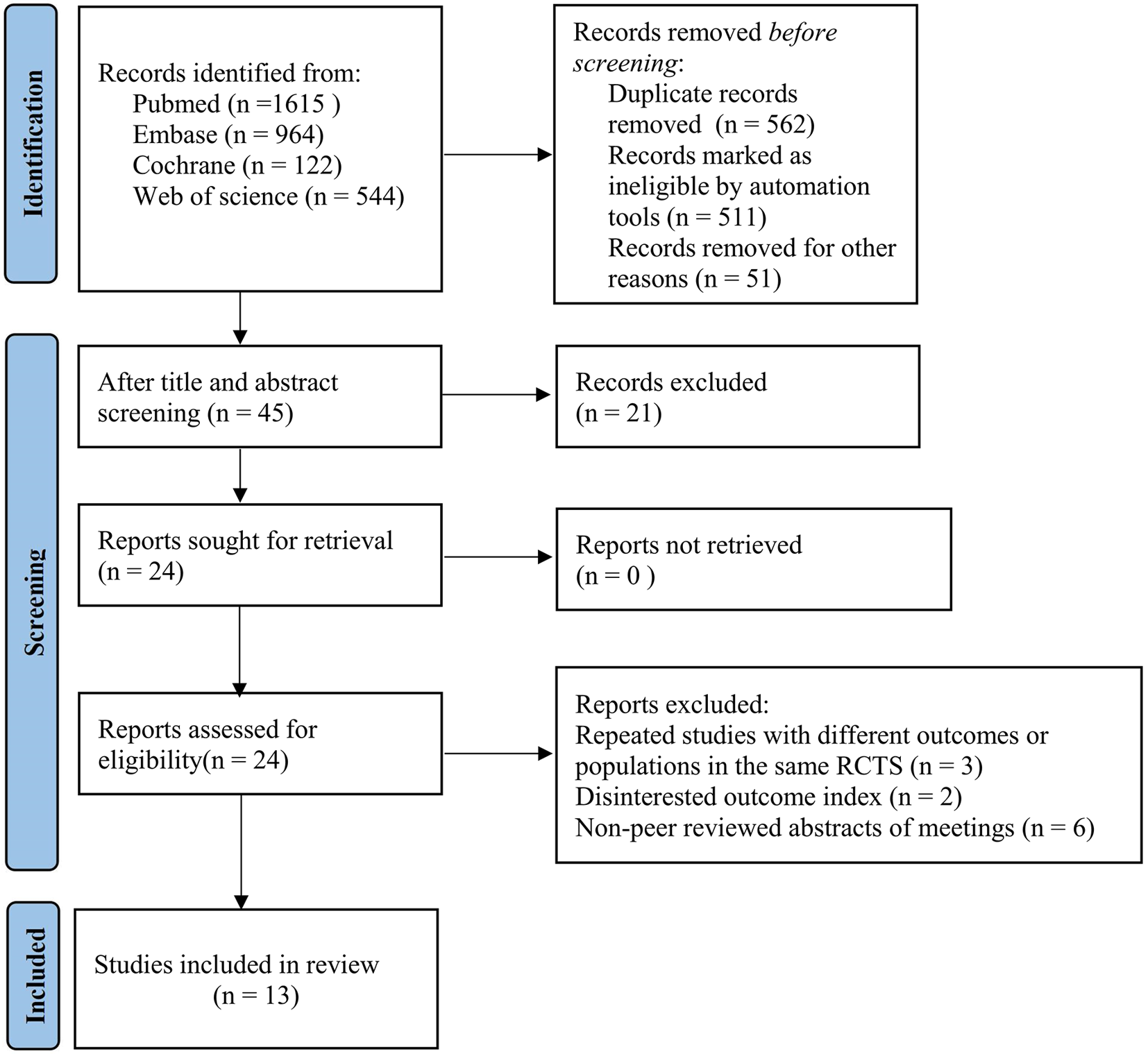
Of 3035 unique articles identified in electronic searches and 2077 articles screened from secondary sources, we included 43 articles in the systematic review of the prevalence of sustained remission/LDA after discontinuation and 37 studies in the scoping review of predictors (Fig. 1). Of the 43 articles in the systematic review, 22 articles reported induction-withdrawal studies and 22 articles reported studies of maintenance TNFi discontinuation, with 1 article including both groups [22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64]. Data on predictors were reported in 12 induction-withdrawal articles [27, 33,34,35,36, 39, 41, 43, 65,66,67,68] and 22 maintenance discontinuation articles [44, 46, 47, 49,50,51,52, 54,55,56, 59,60,61,62, 64, 69,70,71,72,73,74,75,76].
Fig. 1
Flow diagram of study inclusion. Error bars represent 95% confidence intervals
Sustained remission/LDA in induction-withdrawal studiesThese studies included 5 double-blind controlled trials [22,23,24,25,26], 1 open-label trial [27], and 16 studies in which TNFi discontinuation was observational [28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43] (Table 1 and Supplemental Table 3).
Table 1 Proportion of patients with sustained remission or low disease activity in induction-withdrawal studiesThe criterion for TNFi discontinuation was DAS28 < 3.2 in 9 studies, DAS28 < 2.6 in 9 studies, and other indicators in 4 studies. The number of patients who discontinued TNFi ranged from 2 to 200 (median 34; total 1183), with larger samples in the trials. Seven studies examined etanercept, 5 examined infliximab, 5 examined adalimumab, 2 examined certolizumab, and 3 examined various TNFi. Follow-up varied from 24 to 96 weeks. Thirteen studies reported results at 37–52 weeks after TNFi discontinuation, and 6 studies reported results at 24–36 weeks. The proportion of patients with sustained remission/LDA after TNFi discontinuation varied widely (Table 1).
Remission prevalence after discontinuationIn the pooled analysis, 58% had DAS28 < 3.2 and 52% had DAS28 < 2.6 at 37–52 weeks after discontinuation, with high heterogeneity among studies (Fig. 2 and Supplemental table 4).
Fig. 2
Pooled proportions having sustained remission/low disease activity at 37–52 weeks after either discontinuation or continuation of tumor necrosis factor inhibitor treatment in induction-withdrawal studies. Circles represent the DAS28 < 3.2 outcome, squares represent the DAS28 < 2.6 outcome, and triangles represent the SDAI ≤ 3.3 outcome. Closed symbols represent tumor necrosis factor inhibitor discontinuation arms, and open symbols represent continuation arms. Error bars represent 95% confidence intervals
Only four studies reported SDAI-based results, and 40% of patients had SDAI ≤ 3.3 after discontinuation. The proportion remaining in remission/LDA was therefore lower with more stringent definitions of remission. At 24–36 weeks after TNFi discontinuation, 36% of patients maintained DAS28 < 3.2, 73% had DAS28 < 2.6, and 12% had SDAI ≤ 3.3 (Supplemental table 4).
Sensitivity analysis and study heterogeneityThe double-blind controlled trials were rated as having a low or moderate risk of bias, while the open-label trial was rated as having a high risk of bias (Supplemental Fig. 1). Seven observational studies were judged as having a serious risk of bias (Supplemental Fig. 2). In the sensitivity analysis, pooled results were similar when only studies with low or moderate risk of bias were examined (Fig. 2 and Supplemental table 4).
We explored potential heterogeneity by disease activity, duration of RA, and study design among the 9 studies that reported DAS28 < 2.6 outcomes at 37–52 weeks. Among the six studies that required DAS28 < 2.6 at the time of discontinuation [23, 27, 28, 32, 36, 39], the proportion with DAS28 < 2.6 at follow-up 1 year later was 58% (95% CI 33, 82), compared to 42% (95% CI 20, 67) among the three studies that required DAS28 < 3.2 at TNFi discontinuation [22, 24, 26] (p = 0.42). Among the six studies in early RA [22, 23, 26,27,28, 32], the pooled proportion with DAS28 < 2.6 at follow-up was 63% (95% CI 42, 82), compared to 32% (95% CI 17, 49) in three studies in established RA [24, 36, 39] (p = 0.05). Among the five controlled trials [22,23,
Comments (0)