
Remember me

Eosinophilic esophagitis (EoE) is a chronic, immune-mediated disease characterized by esophageal dysfunction and eosinophilic infiltration of the esophageal mucosa, defined as ≥15 eosinophils per high-power field (eos/hpf) (1). EoE can affect patients across a wide age range, and common symptoms include feeding intolerance or aversion, vomiting, heartburn, and regurgitation in children, as well as food impaction and, most commonly, dysphagia in adolescents and adults (2,3). Adding to the complexity of EoE presentation, symptoms are nonspecific and may not directly correlate with disease severity, and there are no established pathognomonic symptoms of EoE in children and adolescents (4–6). The rapidly increasing prevalence of EoE, estimated at approximately 34.2 cases per 100,000 people globally, represents a growing health problem that poses a significant burden for health care systems (7,8). The prevalence of EoE is slightly higher in children and adolescents (aged <16 years; 38.3 cases per 100,000 [USA/Canada]) than in adults (aged ≥18 years; 31.9 cases per 100,000 [USA/Canada]) (8).
Despite the increasing prevalence of EoE (9), there is no US Food and Drug Administration-approved swallowed topical corticosteroid for the treatment of EoE (10). Management strategies are typically limited to off-label use of swallowed topical corticosteroids, proton-pump inhibitors (PPIs), or elimination diets (5,11). As off-label pharmacologic therapies are not specifically optimized for esophageal delivery, they may provide inadequate treatment in patients with EoE (12–14). Few studies to date have examined the efficacy and safety of topical corticosteroids in pediatric or adolescent populations with EoE (5,15).
Budesonide oral suspension (BOS) is a novel, immediate-release, topical corticosteroid optimized as a viscous suspension for patients with EoE, with the aim of lengthening residency time at the esophageal mucosal surface after swallowing (12,13). The efficacy and safety of BOS 2.0 mg twice daily (b.i.d.) were previously established in 2 randomized, double-blind, placebo-controlled phase 2 and phase 3 studies in adolescents and adults with EoE (aged 11–40 years [phase 2] and 11–55 years [phase 3]) (12,13,15,16).
To improve our understanding of the specific response of late-childhood and adolescent patients to BOS, a pooled post hoc analysis from these 2 completed clinical studies was performed to evaluate the efficacy and safety of BOS 2.0 mg b.i.d. in patients aged 11–17 years with EoE over 12 weeks versus placebo.
METHODS Study Design and PopulationData from patients with EoE aged 11–17 years were pooled from 2 completed clinical studies: phase 2 (MPI 101-06; ClinicalTrials.gov identifier: NCT01642212) and phase 3 (SHP621-301; ClinicalTrials.gov identifier: NCT02605837). Primary data from these 2 clinical studies have been published previously (12,13). Both studies were multicenter, 12 weeks, double-blind, and placebo-controlled (12,13); patients underwent upper endoscopy and biopsy at screening, followed by symptom assessment for 4 weeks, during which they received single-blind placebo to assess dosing compliance and to mitigate a potential dysphagia symptom response to placebo. Upon completion of the screening period, eligible patients were randomized to BOS 2.0 mg b.i.d. or placebo (1:1 and 2:1 in the phase 2 and phase 3 studies, respectively), given as a 10 mL oral suspension in the morning and evening for up to 12 weeks (12,13).
Collectively, data were obtained between 2012 and 2019. Study protocols were approved by the institutional review board at each center in accordance with the International Conference on Harmonization and Good Clinical Practice Guidelines and reported as per the Consolidated Standards of Reporting Trials statement. All patients or their parents/legal guardians provided written informed consent prior to participating in the studies. Patients were eligible for inclusion in either study if they had a confirmed diagnosis of EoE according to the 2011 consensus diagnostic guidelines (17); specifically, histologic evidence of EoE (a peak eosinophil count of ≥15 eos/hpf [≥2 esophageal levels]) during screening and did not respond to a high-dose PPI study for ≥6 weeks (12,13). Patients were also required to have symptoms of dysphagia, measured by the Dysphagia Symptom Questionnaire (DSQ), a scoring instrument validated in adolescents and adults aged 11–40 years with EoE (18,19), for ≥4 days in any 2 consecutive weeks during the screening period and in the 2 weeks before randomization.
Key exclusion criteria in both studies were: immunomodulatory therapy use (eg, rituximab or dupilumab), or anticipated use, during the 8 weeks before the screening endoscopy or during the study period; swallowed topical corticosteroid use for EoE or systemic corticosteroid use for any condition, or anticipated use, during the 4 weeks before the screening endoscopy or during the study period; presence of a high-grade esophageal stricture precluding passage of a standard adult upper endoscope during the screening endoscopy; and following a 6-food elimination or a pure liquid diet (12,13).
Additional inclusion and exclusion criteria are reported elsewhere (12,13).
Efficacy EndpointsEfficacy endpoints examined for this pooled analysis were the proportion of patients who achieved histologic responses (≤6, ≤1, and <15 eos/hpf [all esophageal levels ]) at week 12 of therapy and the proportion of patients who achieved a dysphagia symptom response (≥30% reduction in DSQ score (18,19) from baseline) at week 12 of therapy. The proportion of patients with a clinicopathologic response at week 12, defined as a combined histologic and dysphagia symptom response (≤6 eos/hpf and ≥30% reduction in DSQ score from baseline) and the least-squares (LS) mean of the change in peak eosinophil counts, EoE Histology Scoring System (EoEHSS) total score ratios (TSRs) (grade [severity] and stage [extent]) (20), total EoE Endoscopic Reference Scores (EREFS) (21), and DSQ scores, from baseline to week 12 of therapy, were also assessed. Changes in peak eosinophil counts, EoEHSS TSRs, and EREFS from baseline to week 12 of therapy were also examined by esophageal level. Changes in EREFS from baseline to week 12 of therapy were also examined by individual feature (exudates, rings, edema, furrows, and strictures).
Safety AssessmentsSafety assessments included adverse event monitoring, physical examinations, measurements of vital signs, body weight and height, dual X-ray absorptiometry (DXA) for bone mineral density, routine clinical laboratory tests, and adrenocorticotropic hormone (ACTH) stimulation tests (SHP621-301 study only). An abnormal ACTH stimulation test result was defined as a peak ACTH-stimulated cortisol level of ≤18 μg/dL after stimulation with 250 μg of synthetic ACTH.
Statistical AnalysesFor responder analyses (ie, histologic, dysphagia symptom, and clinicopathologic responses), treatment groups were compared using the Cochran-Mantel-Haenszel test, stratified by dietary restriction (dietary restriction or no dietary restriction). Patients without efficacy data available at week 12 of therapy were classified as nonresponders. Patients were considered dysphagia symptom nonresponders if they had fewer than 8 days of DSQ diary data reported in the 2 weeks before the final treatment evaluation (12).
For analyses of continuous endpoints, an analysis of covariance model was used to compare treatment groups, with the baseline score of the endpoint being included as a continuous covariate. As this was a post hoc analysis, P values reported are nominal. Safety was assessed descriptively using the safety set, which included all patients who received ≥1 dose of BOS 2.0 mg or placebo during the double-blind treatment phase.
EthicsStudy protocols were approved by the institutional review board at each center in accordance with the International Conference on Harmonization and Good Clinical Practice Guidelines and reported as per the Consolidated Standards of Reporting Trials statement. All patients or their parents/legal guardians provided written informed consent prior to participating in the studies.
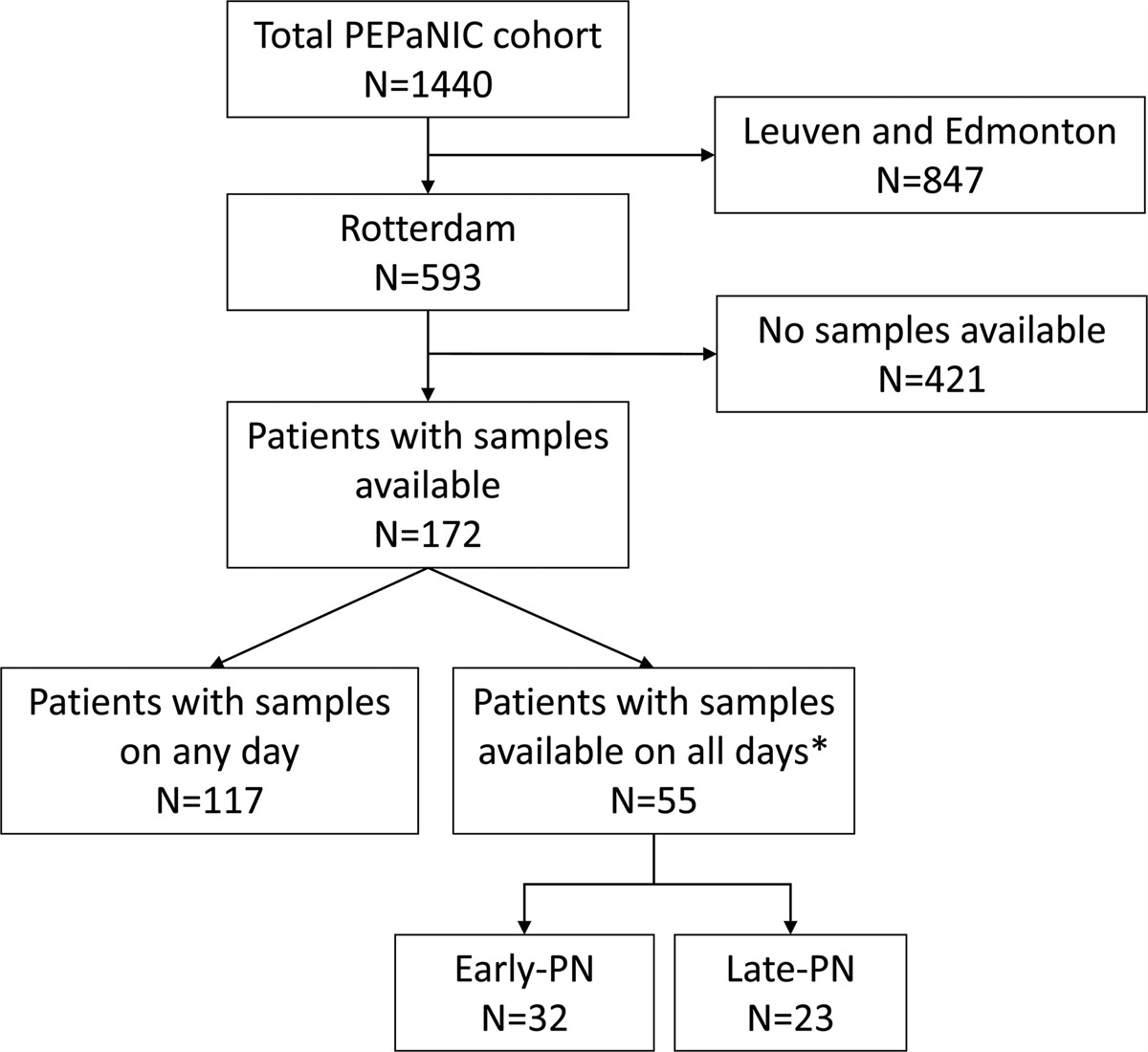
RESULTS Baseline Demographics and Clinical CharacteristicsOverall, 76 patients aged 11–17 years were randomized to receive ≥1 dose of BOS 2.0 mg b.i.d. (n = 45) or placebo (n = 31); Figure 1, Supplemental Digital Content 1, https://links.lww.com/MPG/D315, presents the Consolidated Standards of Reporting Trials flow diagram. The mean (standard deviation [SD]) age was 14.7 (2.2) years and 14.3 (1.7) years for the BOS and placebo groups, respectively. Most patients were male (BOS, 66.7% [30/45]; placebo, 74.2% [23/31]) and white (BOS, 88.9% [40/45]; placebo, 87.1% [27/31]) (Table 1). Overall, baseline demographics and clinical characteristics were similar in the BOS and placebo groups (Table 1). Mean (SD) peak eosinophil counts for BOS- and placebo-treated patients were 91.6 (64.7) eos/hpf and 122.7 (77.3) eos/hpf, respectively. Mean (SD) DSQ scores were also similar at baseline for BOS-treated (29.1 [14.2]) and placebo-treated (28.0 [13.3]) patients.
TABLE 1. - Baseline demographics and clinical characteristics of patients aged 11–17 years with eosinophilic esophagitis (EoE) included in the pooled post hoc analysis Demographic/characteristics BOS 2.0 mg b.i.d.b.i.d. = twice daily; BOS = budesonide oral suspension; DSQ = Dysphagia Symptom Questionnaire; EoE = eosinophilic esophagitis; EoEHSS = EoE Histologic Scoring System; eos/hpf = eosinophils per high-power field; EREFS = EoE Endoscopic Reference Score; PPI = proton-pump inhibitor; SD = standard deviation; TSR = total score ratio.
*TSRs were calculated as normalized ratios after adjusting for missing data (such as no lamina propria available to assess fibrosis) and were calculated for each esophageal level (proximal, middle, and distal).
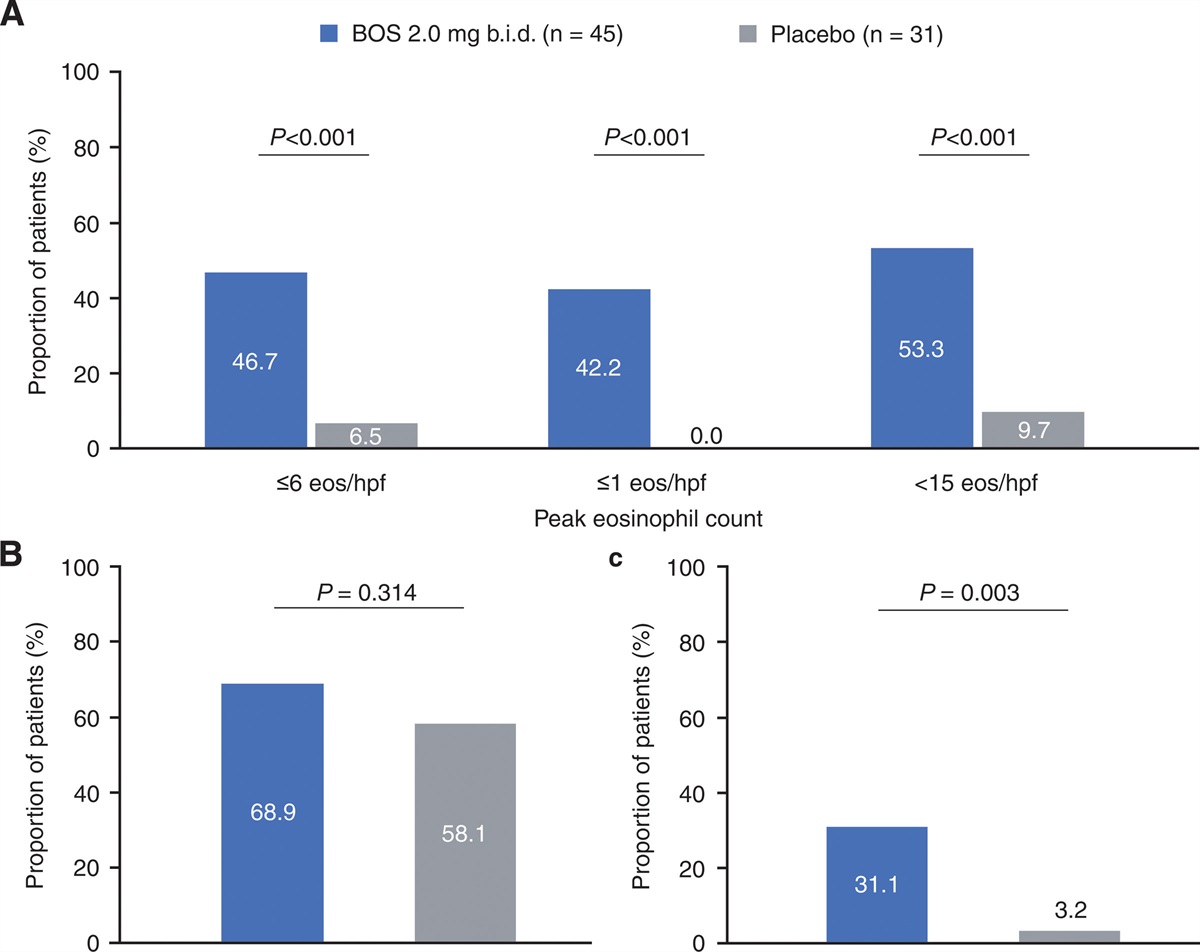
At week 12 of therapy, significantly more BOS-treated than placebo-treated patients achieved histologic responses (≤6 eos/hpf: 46.7% vs 6.5%; ≤1 eos/hpf: 42.2% vs 0.0%; <15 eos/hpf: 53.3% vs 9.7%; all comparisons, P < 0.001; Figure 1A). The proportion of patients who had a dysphagia symptom response was numerically, but not statistically, different between treatment groups (68.9% of BOS-treated patients had a ≥30% reduction in DSQ score from baseline to week 12 of therapy compared with 58.1% of placebo-treated patients; P = 0.314; Figure 1B). Significantly more BOS-treated (31.1%) than placebo-treated (3.2%) patients achieved a clinicopathologic response (ie, ≤6 eos/hpf and ≥30% reduction in DSQ score from baseline to week 12 of therapy; P = 0.003; Figure 1C).
 FIGURE 1.:
FIGURE 1.: The proportion of patients (11–17 years) with eosinophilic esophagitis (EoE) who had (A) a histologic response (≤6, ≤1, and <15 eos/hpf), (B) a dysphagia symptom response (≥30% reduction in DSQ score from baseline)a, and (C) a clinicopathologic response (≤6 eos/hpf and ≥30% reduction in DSQ score from baseline) at week 12 with BOS 2.0 mg b.i.d. or placeboa. P values: Cochran-Mantel-Haenszel test stratified by diet restriction. aDSQ combined scores required ≥8 reported diaries over a 14-day period. b.i.d. = twice daily; BOS = budesonide oral suspension; DSQ = Dysphagia Symptom Questionnaire; eos/hpf = eosinophils per high-power field.
At week 12 of therapy, BOS-treated patients had greater improvements from baseline (ie, greater reductions in scores) than patients who received placebo in LS mean (standard error of the maximum mean [SEM]) peak eosinophil counts (−70.2 [7.4] eos/hpf vs −24.6 [9.1] eos/hpf; P < 0.001; Figure 2A), EoEHSS grade and stage TSRs (grade: −0.24 [0.03] vs −0.05 [0.03]; stage: −0.21 [0.02] vs −0.01 [0.03]; both, P < 0.001; Figure 2B), and total EREFS (−4.1 [0.6] vs −2.1 [0.7]; P = 0.021; Figure 2C). Additionally, BOS-treated patients had greater improvements than placebo-treated patients in LS mean (SEM) peak eosinophil counts, EoEHSS scores, and EREFS from baseline to week 12 across all esophageal levels examined (Table 2). Improvements in LS mean (SEM) EREFS from baseline to week 12 were also found to be greater in BOS-treated than placebo-treated patients for most individual features (Table 2). Changes from baseline to week 12 in LS mean (SEM) DSQ scores were similar in treatment groups (BOS vs placebo: −13.8 [1.8] vs −11.1 [2.1]; P = 0.331; Figure 2D).
TABLE 2. - Summary of peak eosinophil counts, EoE Histology Scoring System (EoEHSS) total score ratios (TSRs), and Endoscopic Reference Scores (EREFS) in patients aged 11–17 years with eosinophilic esophagitis (EoE) treated with budesonide oral suspension (BOS) 2.0 mg b.i.d. or placebo at week 12 of therapy and changes from baseline, stratified by esophageal levels Efficacy outcomes BOS 2.0 mg b.i.d.ANCOVA = analysis of covariance; b.i.d. = twice daily; BOS = budesonide oral suspension; EoE = eosinophilic esophagitis; EoEHSS = EoE Histologic Scoring System; eos/hpf = eosinophils per high-power field; EREFS = EoE Endoscopic Reference Score; LS = least-squares; SEM = standard error of the mean; TSR = total score ratio.
*BOS, n = 41; placebo, n = 28.
†BOS, n = 42; placebo, n = 27.
‡BOS, n = 44; placebo, n = 29.
§ANCOVA model with treatment group as the factor and baseline peak eosinophil count as a continuous covariate.
∥BOS, n = 41; placebo, n = 26.
¶BOS, n = 41; placebo, n = 27.
#EoEHSS TSRs (range, 0–1).
**ANCOVA model with treatment group as factors and baseline histopathologic epithelial features combined TSR of grade or stage as a continuous covariate.
††EREFS (range, 0–20).
‡‡BOS, n = 44; placebo, n = 30.
§§ANCOVA model with treatment group as the factor and baseline endoscopy score as a continuous covariate.
¶¶EREFS individual features (range, 0–1 [edema and strictures], 0–2 [exudates and furrows], and 0–3 [rings]).
 FIGURE 2.:
FIGURE 2.: Change from baseline to week 12 in patients (11–17 years) with eosinophilic esophagitis (EoE) in LS mean (SEM) (A) maximum peak eosinophil counts, (b) EoEHSS TSRs (grade and stage), (c) total EREFS, and (d) DSQ score following BOS 2.0 mg b.i.d. or placebo. P values: analysis of covariance models. b.i.d. = twice daily; BOS = budesonide oral suspension; DSQ = Dysphagia Symptom Questionnaire; EoEHSS = EoE Histologic Scoring System; eos/hpf = eosinophils per high-power field; EREFS = EoE Endoscopic Reference Score; LS = least-squares; SEM = standard error of the mean; TSR = total score ratio.
Safety AssessmentsBOS 2.0 mg b.i.d. was well tolerated in patients aged 11–17 years. No substantial differences in adverse events were observed between patients who received BOS and those who received placebo. Treatment-emergent adverse events (TEAEs) were mild or moderate in severity, and no severe or serious adverse events were observed in either treatment group. The most commonly reported treatment-emergent events were: infections (BOS, 26.7%; placebo, 22.6%) and gastrointestinal disorders (BOS, 11.1%; placebo, 25.8%). The most frequently reported of these were nasopharyngitis (BOS, 8.9%; placebo, 9.7%), diarrhea (BOS, 2.2%; placebo, 9.7%), and vomiting (BOS, 2.2%; placebo, 9.7%) (Table 1, Supplemental Digital Content 2, https://links.lww.com/MPG/D316, summarizes TEAEs in patients aged 11–17 years with EoE at week 12 of therapy with BOS 2.0 mg b.i.d or placebo). No study discontinuations or deaths occurred as a result of TEAEs. There were no clinically meaningful changes in vital signs (including body weight and height), physical examination findings, or clinical laboratory test results. Figure 2, Supplemental Digital Content 3, https://links.lww.com/MPG/D317, provides further details. DXA scans were performed in a total of 25 BOS-treated and 12 placebo-treated participants (SHP621-301 study only) (12) and did not demonstrate any impact of BOS on bone density or growth (Table 2, Supplemental Digital Content 4, https://links.lww.com/MPG/D318). The proportion of patients who reported an abnormal shift in cortisol levels after stimulation with synthetic ACTH (250 µg) from baseline to week 12 of therapy was similar for BOS- and placebo-treated patients (SHP621-301 study only) (Table 3, Supplemental Digital Content 5, https://links.lww.com/MPG/D319).
DISCUSSIONThis post hoc analysis demonstrated BOS 2.0 mg b.i.d. substantially improved histologic, endoscopic, and clinicopathologic responses in patients aged 11–17 years with EoE compared with placebo over 12 weeks.
At all thresholds examined, a greater proportion of BOS-treated than placebo-treated patients achieved histologic responses. Importantly, a greater proportion of patients who received BOS than placebo achieved a clinicopathologic (histologic and dysphagia symptom) response. BOS-treated patients also had greater improvements from baseline to week 12 in LS mean peak eosinophil counts, EoEHSS grade and stage TSRs, and total EREFS (and for most individual features of EREFS) than placebo-treated patients. In contrast, the proportion of patients who achieved a dysphagia symptom response, assessed by the DSQ (12,18), was numerically, but not statistically significantly, greater for BOS-treated than placebo-treated patients. Over 12 weeks of therapy, BOS was well tolerated; TEAEs were mild or moderate in severity and were generally similar in patients who received BOS and in those who received placebo. No severe or serious adverse events were reported, and an abnormal ACTH stimulation test result was recorded in a greater proportion of placebo-treated than BOS-treated patients. Reports of oral or esophageal candidiasis were low and were more frequent in patients who received BOS than placebo.
These findings are in line with those seen in the overall population of patients aged 11–55 years with EoE from the phase 3 study (SHP621-301), for whom there was a difference in reduction in peak eosinophil count of −47.6 eos/hpf for BOS versus placebo at week 12 of therapy, compared with −45.6 eos/hpf for our pooled pediatric subpopulation (12). Our results are also consistent with findings from a pediatric study that found significantly reduced peak eosinophil counts throughout the esophagus in BOS-treated compared with placebo-treated patients aged 2–18 years. Peak eosinophil counts were reduced by 52.6% (P = 0.009) for a medium dose of BOS (total daily dose: 1.4 or 2.0 mg, depending on the patient’s age) and 94.1% (P < 0.001) for a high dose of BOS (total daily dose: 2.8 or 4.0 mg), compared with placebo, at week 12 of therapy (22). The previous study also found a similar dysphagia symptom response in BOS and placebo groups at week 12 of therapy, although the investigators did not measure the treatment response using a validated instrument or require a symptom threshold for study entry (22). The lack of statistical significance for dysphagia symptom response could be attributed to the high placebo response rate, which was also observed in a post hoc analysis of symptom response to placebo in patients with EoE aged 11–40 years (23). Symptom reporting is inherently challenging, particularly for esophageal dysphagia, and in children, in whom studies in EoE have demonstrated age- and race-dependent differences in symptom presentation (24,25), with resulting adaptive behaviors such as eating modifications possibly affecting perceptions of dysphagia. The DSQ is also not powered specifically for an adolescent population, for whom eating modifications are common (26). However, the DSQ has been validated in patients aged 11–40 years with EoE, for whom statistically significant reductions in DSQ scores for BOS compared with placebo have been observed (12,13).
To date, few studies have examined efficacy of swallowed topical corticosteroids in patients younger than 18 years with EoE (12,13,27,28). Swallowed fluticasone propionate (880 µg b.i.d.) has previously shown efficacy in reducing esophageal eosinophilia compared with placebo in patients aged 3–18 years (28). Further, in a comparative open-label study in patients with EoE aged 1–16 years, oral prednisone suspension/tablet 1 mg/kg b.i.d. achieved greater histologic improvements than fluticasone propionate (27). Similar to our study, the proportions of patients who received fluticasone propionate and placebo who achieved a peak eosinophil count of ≤6 eos/hpf in both the proximal and distal esophagus were significantly greater between treatment groups (fluticasone propionate vs placebo: 55% vs 18%; P > 0.05) (28). Topical corticosteroids are generally preferable in localized conditions such as EoE, because they have fewer reports of systemic adverse events (16). This highlights the need for more head-to-head, randomized controlled studies to provide evidence-based insights into the efficacy and safety of swallowed topical corticosteroids in adolescents with EoE.
It is important to note the limitations of this study. This analysis was conducted post hoc and therefore was not powered for an adolescent subpopulation; thus, the sample size was small and may not be sufficient to assess differences generalizable to the population in terms of dysphagia symptom response to treatment. Additionally, stringent entry criteria were applied for both studies, which predominantly enrolled patients with moderate or severe disease, many of whom presented with fibrostenosis, and PPI-unresponsive eosinophilia (12,13). Moreover, there is a well-established discordance between histology and patient-reported symptoms in mucosal and gastrointestinal conditions (29,30), including but not limited to EoE (31), and in particular for individuals who have undergone endoscopic dilation (32–34). This disparity has also been observed in recent phase 2 and 3 clinical studies which, like our analysis, found a high dysphagia symptom response in placebo-treated patients with EoE (35,36). This high placebo response rate could potentially be a result of small sample population or inherent subjectivity of patient-reported outcomes such as the DSQ used to assess symptoms in these studies. It is also possible by the time patients with EoE reach adolescence, modified or compensatory eating and dietary habits have reduced or masked symptom severity (37,38). As such, symptom assessment alone for diagnosis and monitoring of EoE may be insufficient (39). Nonetheless, our study found improvements in the histologic response post-treatment, as well as concomitant improvements in additional efficacy outcomes including EoEHSS grade and stage TSRs, total EREFS, and DSQ scores. The combination of histologic and symptom ou
Comments (0)