As previous studies have postulated a possible causal relationship between lower BMD and ASMs, not only for enzyme-inducing drugs but also for e.g. valproic acid [18, 19], gabapentin [20] and in animal models also with third generation ASMs such as levetiracetam [21], lamotrigine and topiramate [22], an assessment of the effects on bone health of a compound such as ESL appears interesting from a clinical perspective.
In this longitudinal prospective study investigating the effects of ESL on bone health, no significant group effects on BMD or on laboratory parameters of bone metabolism were found in 26 patients enrolled at the two participating study centres. Intra-individually, however, two patients passed the threshold for osteopenia measured at the femoral neck during the 1-year observation period.
ESL is a third generation ASM, which, like OXC, is a weak enzyme inducer of CYP3A4 and UDP-glucuronyltransferase, with a smaller effect size and effects on a smaller range of enzymes than carbamazepine. The overall (S)-licarbazepine to (R)-licarbazepine ratio of ESL is 20:1, which is considered to be advantageous towards OXC (ratio 4:1), since (S)-licarbazepine is thought to be more effective, less toxic and more efficient at crossing the blood–brain barrier than (R)-licarbazepine [23].
We hypothesized that ESL may exert similar effects on bone metabolism as reported in some of the studies assessing OXC, despite differences related to its molecular structure and partially distinct metabolic properties. In our study, we aimed to describe the effect of ESL on bone health for the first time, while at the same time adding information to the already existing body of evidence of weak enzyme inducers on BMD and on laboratory parameters of bone metabolism. Most studies evaluating ASM effects on bone mineral metabolism are cross-sectional. Longitudinal studies such as ours focusing on the effects of single agents provide better evidence for causal relationships.
Measurement of BMD is the most commonly used predictor of fracture risk in postmenopausal women and older men, thus it is a suitable primary outcome parameter when studying the effects of ASM on bone health.
Data on potentially detrimental effects on bone density of some enzyme inducing ASMs like CBZ and OXC are heterogeneous, yet undisputed for PHT. In a longitudinal study of premenopausal women with epilepsy on ASM monotherapy, Pack et al. [7] found that those patients receiving PHT sustained significant femoral neck bone loss after 1 year of treatment but did not have bone loss at other sites. In contrast, patients treated with carbamazepine, valproate, or lamotrigine had no loss in bone mass at any site. The femoral neck bone loss in young, premenopausal women treated with PHT monotherapy for 1 year was 2.6%, which was eight times greater than described in a larger cohort of women without ASM treatment [7]. In these women, lower serum 25-hydroxyvitamin D concentrations were associated with higher parathyroid hormone, bone alkaline phosphatase, and urine N-telopeptide levels, a biochemical pattern consistent with secondary hyperparathyroidism and increased bone remodeling. Not all studies found significant changes in BMD or bone metabolism during therapy with CBZ [24,25,26], yet several investigations showed increased bone turnover in epilepsy patients [3, 27].
In our study, the proportion of postmenopausal women was 19.2% (n = 5). Among the six patients with osteopenia at the baseline screening with DEXA scans there was only one postmenopausal woman aged 59, the other five patients were male, mean age 40.2 ± 9.7 years. This finding makes it seem likely that a relevant proportion of epilepsy patients outside the special risk group of postmenopausal women have an increased susceptibility to bone mass loss due to a variety of possible predisposing factors, including treatment with ASM.
For OXC, the evidence on catabolic effects on bone structure is unequivocal. One study in 14 children treated with OXC showed that serum ALP was elevated and BMD values were lower in patients after more than 1 year of treatment compared with healthy controls [5]. Since data collection in this cross-sectional study was performed only at one point of time, the causality of these findings with OXC treatment remains unclear. Notably, in our study, 24 of 26 patients had at least one metabolic parameter outside the standard range at baseline prior to introduction of ESL, pointing to the complex attribution of the effects of individual ASMs on bone health in cross-sectional studies. Another study in 34 children with newly diagnosed epilepsy reported a significant decrease in 25-OHD levels after 18 months of monotherapy with OXC, without a correlation between 25-OHD levels and BMD [11]. Comparing 44 children treated with OXC with a healthy control group, Babacan et al. [28] showed that serum levels of calcium, osteocalcin, 25-hydroxyvitamin D, and BMD did not differ significantly between the study and control group. In contrast, serum levels of parathyroid hormone, alkaline phosphatase and phosphorus were higher within the group on OXC treatment, and calcitonin levels were lower [28]. Mintzer et al. [6] reported 24 adult patients on monotherapy with OXC and 21 on CBZ to have reduced 25-OHD-levels and elevated parathyroid hormone and bone specific alkaline phosphatase after treatment periods longer than 1 year, as compared with healthy controls.
On the other hand, the study of Koo et al. [13] did not find negative effects on BMD and on biochemical markers in 41 drug naïve epilepsy patients who were treated with OXC for about 1 year, similar to findings of Cetinkaya et al. [12] in 28 adult epilepsy patients.
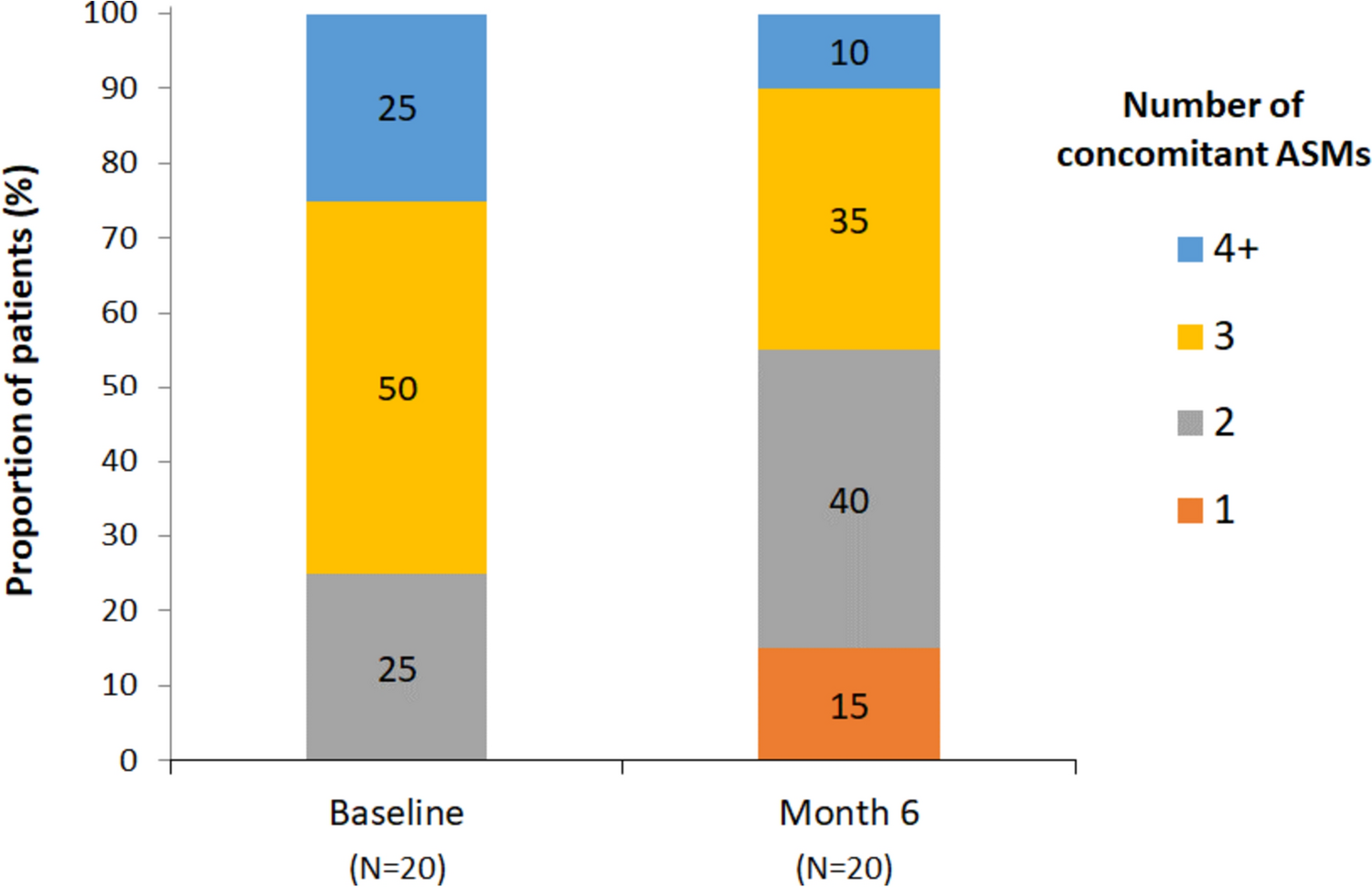
We here for the first time report the results from an observational real world longitudinal study focusing on the effects of ESL on BMD and on bone metabolism. Since effects on bone health of new ASMs are not evaluated during controlled trials, real world data with sufficiently long exposure periods are crucial to estimate the risk new agents may pose to bone health. The mean number of concomitantly administered ASMs in our patient population was 1.19 (± 0.98); maximum 3 ASMs. No patient took ASMs known to have enzyme-inducing effects. Nine patients received ESL as monotherapy. None of the patients received comedication with other drug classes that increase the risk of osteoporosis, such as selective serotonin reuptake inhibitors (SSRIs) or proton pump inhibitors. Thus, the observational conditions in our study allow us to draw conclusions on pharmacological effects of ESL on bone health.
It needs to be considered that besides the potentially detrimental effects of ASMs on bone health, ASM use may be associated with poor health, other medical conditions, lifestyle behaviour and neurological impairments that can also lead to greater rates of bone loss. Since immobilization was one of the exclusion criteria for our study, we aimed to rule out this potentially important factor as a confounding variable. In other studies on bone health in epilepsy patients an apparent association between ASM use and bone loss might be due, at least to some extent, to these confounding factors.
As significant effects were found neither on bone density nor on bone metabolism at the group level in our study, and as confounding variables in the form of anabolic effects are not likely to have influenced the results significantly, this prospective study design provides the first evidence that ESL has no detrimental effects on bone health after exposure to the drug for 1 year.
4.1 Limitations
Key limitations of the study are the small patient cohort and a relatively short follow-up period. Larger cohorts would provide more robust statistical power, and longer follow-up periods can reveal trends or consequences that may not manifest within a year. Furthermore, for the 2/26 patients in whom the osteopenia threshold was crossed during the treatment period, it cannot be automatically assumed that ESL treatment was the (only) cause; notably these patients were an otherwise healthy young man aged 31 years and a postmenopausal woman aged 51 years. Another limitation is the potential lack of diversity in the patient population. The patients included in the study may not adequately represent the broader population of epilepsy patients who might be prescribed ESL. This could limit the generalizability of the findings. Further information on larger patient cohorts with longer follow-up periods are needed to see if weak enzyme-inducing ASMs as ESL may exert adverse effects on bone health in susceptible subgroups.


留言 (0)