
Remember me



Data were obtained from four international cohorts targeting middle-aged and older populations, namely, the China Health and Retirement Longitudinal Study (CHARLS) and Mexican Health and Aging Study (MHAS) from developing countries in the East and West, and the Health and Retirement Study (HRS) and Survey of Health, Ageing and Retirement in Europe (SHARE) from developed countries, which were designed to provide comparable results.
The CHARLS was approved by the Institutional Review Board and Ethics Review Committee of Peking University [16]; the MHAS was approved by the Institutional Review Boards and Ethics Committees of the University of Texas Medical Branch in the USA, the National Institute of Statistics and Geography (INEGI), and the National Institute of Public Health (INSP) in Mexico [17]; the HRS was approved by the institute for social research and survey research center of the University of Michigan [18]; and the SHARE was approved by the Ethics Committee of the University of Mannheim and the Ethics Committee of the Max Planck Society [19]. Written informed consent was obtained from all participants.
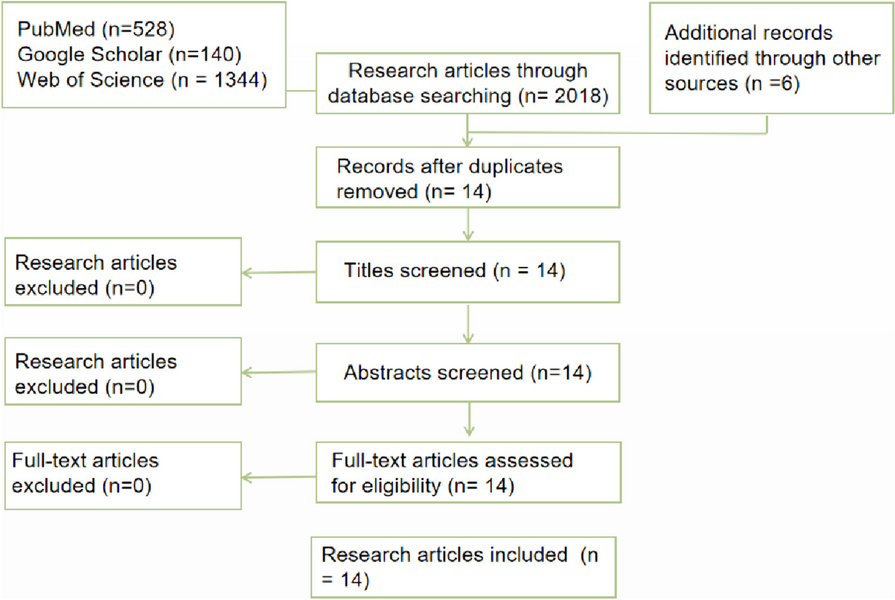
In this study, the CHARLS 2011–2018, MHAS 2012–2021, HRS 2012–2020, and SHARE 2013–2020 were utilized (Fig. 1).
Fig. 1
Flowchart of study. Notes: CHARLS, China Health and Retirement Longitudinal Study. MHAS, Mexican Health and Aging Study. HRS, Health and Retirement Study. SHARE, Survey of Health, Ageing and Retirement in Europe. CMDs, cardiometabolic diseases
Definition of internet use and digital exclusionIn the CHARLS, participants who reported using the internet within the last month were classified as internet users. For the MHAS, participants were considered internet users if they reported having internet access as part of their household electronics. In the HRS, participants were asked: ‘‘Do you regularly use the Internet (or the World Wide Web) for sending and receiving e-mail or for any other purpose, such as making purchases, searching for information, or making travel reservations?”. Those who answered yes were considered internet users. In the SHARE, participants were asked if they had used the internet within the past seven days, and those who answered yes were classified as internet users. Internet use among four cohorts was defined at baseline, and participants who did not meet these criteria were categorized as digital exclusion [2].
Definition of CMDs and deathCMDs in the CHARLS, MHAS, HRS, and SHARE included diabetes, heart diseases, and stroke. Diabetes in the CHARLS was defined as fasting plasma glucose ≥ 7.0 mmol/L, and/or random plasma glucose ≥ 11.1 mmol/L, and/or HbA1c ≥ 6.5%, and/or with physician diagnosis or treatment, while that in the MHAS, HRS, and SHARE was defined using physician diagnosis or treatment given data limitations. Furthermore, heart diseases and stroke in these cohorts were defined by participants’ self-reported physician diagnoses. The presence of two or more CMDs in the same individual was classified as CMM.
Death was confirmed through proxy respondents, such as family members, household members, or neighbors.
Measurement of depressive symptomsDepressive symptoms were assessed at baseline in the four cohorts using the Center for Epidemiological Studies Depression Scale (CESD) or the Europe-depression (EURO-D) scale. Detailed information can be found in eMethods in the Supplement.
CovariatesInformation on age, sex, education, household income, marital status, smoking history, drinking history, and hypertension was collected through face-to-face interviews or telephone interviews at baseline. Education was classified as less than high school, high school, and college or above. Household income was divided into first, second, and third tertiles in sequence. Marital status included married/cohabiting and single. Smoking and drinking history were classified as current smoking/drinking or not. Hypertension was defined using participants’ self-reported physician diagnoses.
Body mass index (BMI) was measured by trained health workers in the CHARLS, MHAS, HRS, and SHARE at baseline. However, for HRS respondents who had missing data on their BMI, self-reported BMI values were utilized. Abnormal weight was defined as BMI ≥ 25 kg/m2.
Statistical analysisThe baseline characteristics of included participants were described as medians with interquartile ranges (IQRs) for age given its skewed distribution, and frequency and per cent (%) for categorical variables. Missing data on covariates were multiply imputed using the ‘mice’ package in R.
The competing risk analysis based on subdistribution hazard regression was utilized to investigate the associations of internet use with new-onset diabetes, heart diseases, stroke, and CMM after excluding those with corresponding diseases at baseline and considering the competing risk of death in the CHARLS, MHAS, HRS, and SHARE, respectively. The proportional hazards assumption was verified using scaled Schoenfeld residual tests. All models were adjusted for age, sex, education, household income, marital status, current smoking, current drinking, abnormal weight, and hypertension.
Two sensitivity analyses were conducted: First, complete-case analysis after excluding those with missing data; Second, excluding new-onset CMDs and CMM within the next wave to account for potential latency time windows and avoid the potential reverse-causality bias.
The mediating role of depressive symptoms in the association of internet use with new-onset CMDs, CMM, and death in the CHARLS, MHAS, HRS, and SHARE was further investigated using the mediation analysis.
Furthermore, age (< 65, >=65)-, sex (men, women)-, education (less than high school, high school, college or above)-, household income (first, second, third tertiles)-, and marital status (married/cohabiting, single)-stratified associations of internet use with new-onset CMDs, CMM, and death in the CHARLS, MHAS, HRS, and SHARE were investigated to explore potential effect modifications.
Subsequently, patients with prior CMDs or CMM in the CHARLS, MHAS, HRS, and SHARE were included to explore the associations between internet use and death. The mediating role of depressive symptoms was also explored.
Random-effects meta-analysis was used to pool the subdistribution hazard ratios (sHRs) and corresponding 95% confidence intervals (CIs) from different cohorts to derive overall effect estimates. The heterogeneity of effect estimated across cohorts was tested using the Cochran Q test and I2 statistic.
Reporting of this study was done under Strengthening the Reporting of Observational studies in Epidemiology (STROBE) guidelines. Analyses were performed using SAS statistical software version 9.4 (SAS Institute) and R statistical software version 4.2.3 (R Project for Statistical Computing). All analyses were two-sided, and the P values of < 0.05 and 95% CIs that did not cross 1.00 were considered statistically significant.
Comments (0)