
Remember me



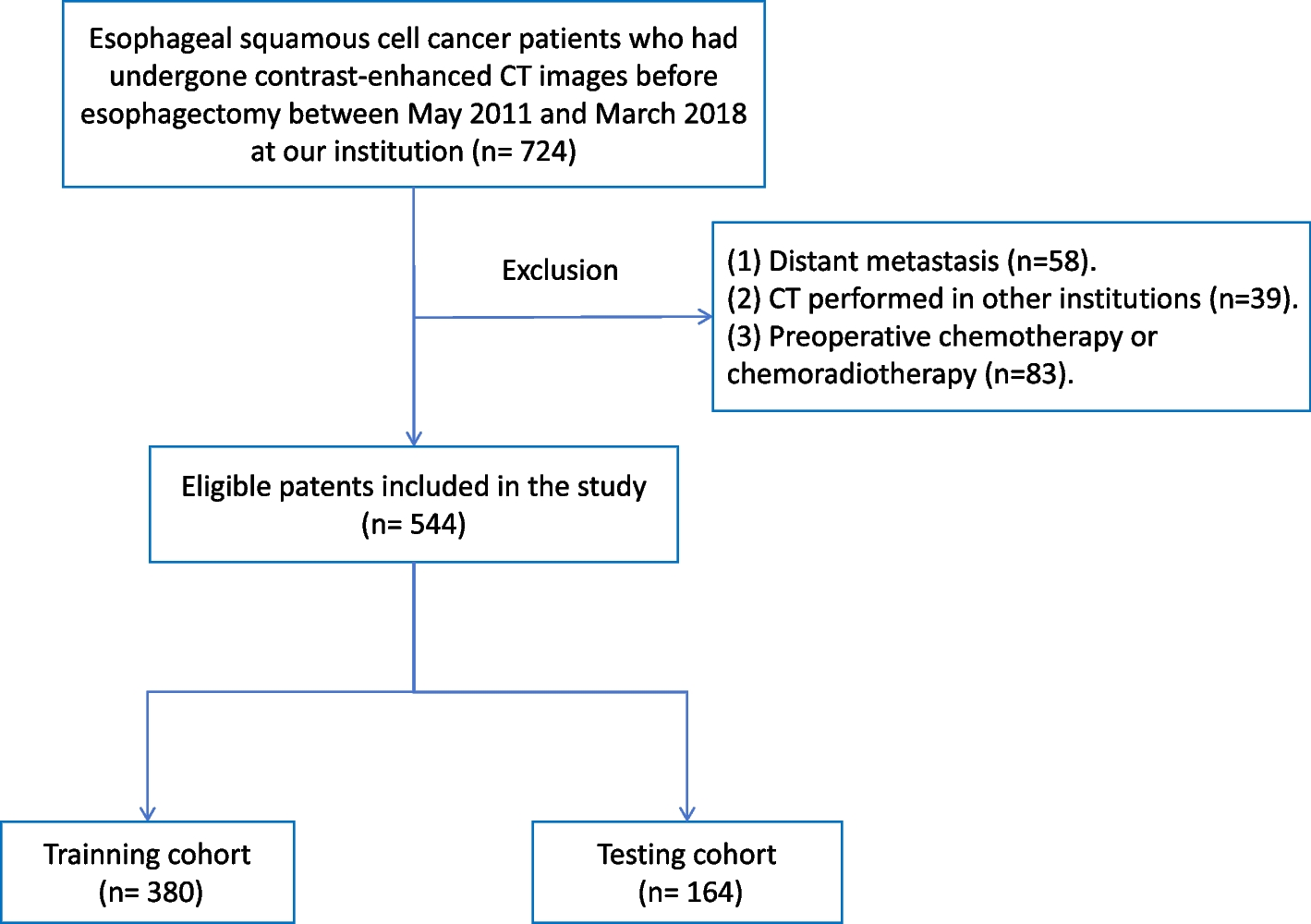


Sixty-seven patients with histological proven HCC (57 men and 10 women; median age, 57 [range, 32–83] years old) were enrolled in our study (Fig. 1). The most common etiology was hepatitis B infection (n = 46, 68.7%), and eighteen patients presented with cirrhosis. Fifty-nine treatment-naive patients received paired 18F-FDG and 18F-FAPI PET examinations for initial staging, and 8 patients with recurrent HCC underwent paired examinations for restaging. 26.9% (18 of 67) of patients had intrahepatic lesions invading macrovascular, and 19.4% (13 of 67) of patients were identified to have extrahepatic metastasis (6 patients with lymph node metastasis and 9 patients with distant metastasis) (Table 1).
Table 1 Baseline patient characteristics of the enrolled patients 18F-FDG PET and 18F-FAPI PET in detection of intrahepatic lesionsIn the initial staging group of 59 patients (a total of 234 lesions), the detecting rate of 18F-FAPI PET for intrahepatic lesions is significantly higher than 18F-FDG PET among patients with T1-3 stages (detail in Table 2, Figs. 2 and 3) [T1: 93.8% (15/16) vs. 31.3% (5/16), P = 0.0006; T2: 100% (13/13) vs. 38.5% (5/13), P = 0.0016; T3: 100% (14/14) vs. 35.7% (5/14), P = 0.0006; T4: 100% (16/16) vs. 100% (16/16), P > 0.05], and the lesions in T2-4 stage patients were more clearly characterized by higher activity (median SUVmax, T2: 9.9 vs. 5.3, P = 0.0339; T3: 10.9 vs. 5.5, P = 0.0085; T4: 12.9 vs. 14.5, P = 0.0457) and clearer boundaries (median TBR, T2: 5.0 vs. 1.7, P = 0.0002; T3: 6.6 vs. 2.1, P = 0.0001; T4: 10.2 vs. 3.1, P < 0.0001) in 18F-FAPI PET than in 18F-FDG PET (Supplementary Fig. 1a & b).
Table 2 Comparison of 18F-FDG PET/CT and 18F-FAPI PET/CT for the intrahepatic lesions of 67 patientsFig. 2
Nine representative patients with HCC underwent 18F-FDG & 18F-FAPI PET/CT imaging. 18F-FAPI PET/CT outperformed.18F-FDG PET/CT in detecting primary tumors (Patient No. 32, 33, 34, 49), intrahepatic subfoci (Patient No. 13, 38, 42, 47, 48), supraclavicular lymph node metastases (Patient No. 13, 48), retroperitoneum lymph node metastases (Patient No. 48), and comparable in detecting distant metastases (Patient No. 48)
Fig. 3
A 41-year-old male patient (Patient No. 51) with HCC (moderately differentiated) was confirmed by biopsy. 18F-FDG PET/CT displayed moderate uptake in the section II of the liver; However, the corresponding CT scan showed more nodules in other lobes of the liver. 18F-FAPI PET/CT detects greater radiotracer in primary lesions and other intrahepatic subfoci on both MIP (large arrow) and axial images (small arrow)
In the evaluation of recurrent tumors in 8 patients (a total of 24 lesions), there was no statistically significance in the sensitivity of detecting recurrent tumors between 18F-FAPI PET and 18F-FDG PET [100% (8/8) vs. 50.0% (4/8), P = 0.0769], while the TBR of 18F-FAPI PET/CT was significantly higher than that of 18F-FDG PET/CT for local recurrence (median TBR: 5.4 vs 1.4, P = 0.0078) (Table 2 and Fig. 4).
Fig. 4
A 57-year-old male patient (Patient No. 50) with recurrent HCC (moderately differentiated) was confirmed by postoperative pathology. 18F-FDG PET/CT displayed no uptake in this lesion, although the corresponding CT scan showed lamellar low-density shadow in right lobe of the liver. 18F-FAPI PET/CT revealed intense uptake (SUVmax 9.0; TBR 6.0) in the recurrent lesion on both maximum intensity projection (MIP) (large arrow) and axial images (small arrow)
As shown in Table 2, 18F-FAPI PET/CT depicted 92.2% of the intrahepatic lesions (238 of 258), which was much better than 41.1% (106 of 258) of 18F-FDG PET/CT (P < 0.0001). According to tumour size, 18F-FAPI PET detected significantly more intrahepatic lesions than 18F-FDG PET among different sizes subgroups, especially in the early stage HCC (Fig. 3) [≤ 2 cm: 88.1% (97/110) vs. 25.5% (28/110), P < 0.0001; > 2 cm and ≤ 5 cm: 89.9% (80/89) vs. 38.2% (34/89), P < 0.0001; > 5 cm: 100% (59/59) vs. 74.6% (44/59), P < 0.0001]. Besides, there were also significant differences in 18F-FAPI PET and 18F-FDG PET uptake among different tumor size groups (all P < 0.0001, Supplementary Fig. 1c & d).
A total of 18 patients had macrovascular invasion (16 patients for initial staging; 2 patients for restaging). There was no statistically significance in the sensitivity of detecting macrovascular invasion between 18F-FAPI PET and 18F-FDG PET [88.9% (16/18) vs. 100% (18/18), P = 0.486], and the SUVmax and TBR of 18 paired macrovascular invading lesions on 18F-FAPI PET/CT images were significantly lower than on 18F-FDG PET/CT images (P = 0.007 and P = 0.043, respectively) (Table 2).
18F-FDG PET and 18F-FAPI PET for assessment of lymph node metastasisAccording to the diagnostic criteria for lymph node metastases, 129 lymph nodes lesions in 7 patients were evaluated. The sensitivity of 18F-FAPI PET in detecting lymph node metastases was 97.9% (126/129), which was higher than 18F-FDG PET [89.1% (115/129), P = 0.01]. The TBR of 18F-FAPI PET in lymph node metastasis was significantly higher than that in 18F-FDG PET (6.3 vs 4.5, P < 0.0001), while there was no significant difference in SUVmax (7.3 vs 7.6, P = 0.7475) (Table 3 and Fig. 2). Sixty-four of 129 (48.8%) lymph node metastasis were greater than 1.0 cm in short diameter, and the detecting rate of 18F-FAPI PET and 18F-FDG PET for these lymph nodes both were 100%. For lymph node in short diameter (≤ 1.0 cm), the sensitivities of 18F-FAPI PET is significantly higher than 18F-FDG PET (Fig. 5) [95.4% (62/65) vs. 78.5% (51/65), P < 0.0001]. The TBR of 18F-FAPI PET in metastasis lymph node (≤ 1.0 cm) were significantly higher than 18F-FDG PET (5.0 vs. 3.3, P = 0.0016), but there was no significance in SUVmax between two agents (Supplementary Fig. 1e & f).
Table 3 Comparison of 18F-FDG PET/CT and 18F-FAPI PET/CT for the extrahepatic lesionsFig. 5
A 62-year-old male patient (Patient No. 13) with HCC (moderately differentiated) was confirmed by biopsy. Compared with 18F-FDG PET/CT, 18F-FAPI PET/CT revealed more intrahepatic subfoci (white arrow in axial images) and more lymph node metastases (red arrow in axial, coronal images). There was a lymph node in right upper mediastinum, showing low-uptake in 18F-FAPI but intense uptake in 18F-FDG, final pathological findings confirmed inflammatory
18F-FDG PET and 18F-FAPI PET in evaluation of distant metastasisA total of 66 distant metastatic lesions in 9 patients were confirmed based on the reference standards. There was no statistically significant difference in sensitivity between 18F-FAPI PET/CT and 18F-FDG PET/CT in detecting distant metastatic lesions [42 (63.6%) vs 46 (69.7%), P = 0.58)] (Supplementary Fig. 1g).
Regarding the 3 patients with bone metastasis, 18F-FAPI PET had a significant lower sensitivity than 18F-FDG PET [66.7% (16/24) vs. 100% (24/24), P = 0.004], and 18F-FDG PET/CT showed higher SUVmax and TBR than 18F-FAPI PET/CT in bone metastasis evaluation (median SUVmax: 11.0 vs 3.0, P = 0.0007; median TBR: 24.15 vs 6.3, P = 0.0014) (Table 3). Only one patients was diagnosed with peritoneal metastasis (17 lesions, Patient 22 Supplementary Table S1). In contrast to the SUVmax, the differences between 18F-FAPI and 18F-FDG imaging were significant quantified by the TBR (median SUVmax: 4.8 vs 3.9, P = 0.0731; median TBR: 5.3 vs 1.7, P < 0.0001) (Table 3).
Changes in staging and therapeutic managementIn the initial assessment of 59 patients, 18F-FAPI imaging detected primary HCC tumors in 16 patients with 18F-FDG-negative. These patients received the available treatment as early as possible since 18F-FAPI detected the primary lesion [11 patients were treated with surgery or ablation; 4 patients with transcatheter arterial chemoembolization (TACE) plus systemic therapy; and 1 patients with TACE plus systemic therapy plus radiotherapy]. With more intrahepatic subfoci revealed by 18F-FAPI PET than 18F-FDG PET/CT, the TNM staging was upgraded in 12 patients (12/59, 20.3%) (four from IB to II, eight from II to IIIA). As a result, instead of the previously planned surgical treatment, four patient received TACE and systemic chemotherapy, while eight patients received palliative systemic treatment and radiation (Table 4 and Fig. 6).
Table 4 Comparison of 18F-FDG PET based and 18F-FAPI PET based TNM restagingFig. 6
Overview of impact of 18F-FAPI PET/CT on staging and therapeutic management in HCC, therapeutic management was altered in 31 of 67 individuals
Among the other 8 patients with recurrence, 18F-FAPI PET identified 18F-FDG-negative locally recurrent tumors in 4 patients (50%) (Table 5), resulting in cancellation of dynamic review and administration of surgery or ablation treatment (Fig. 6).
Table 5 Comparison of 18F-FDG PET and 18F-FAPI PET in post treatment patients
Comments (0)