
記住我
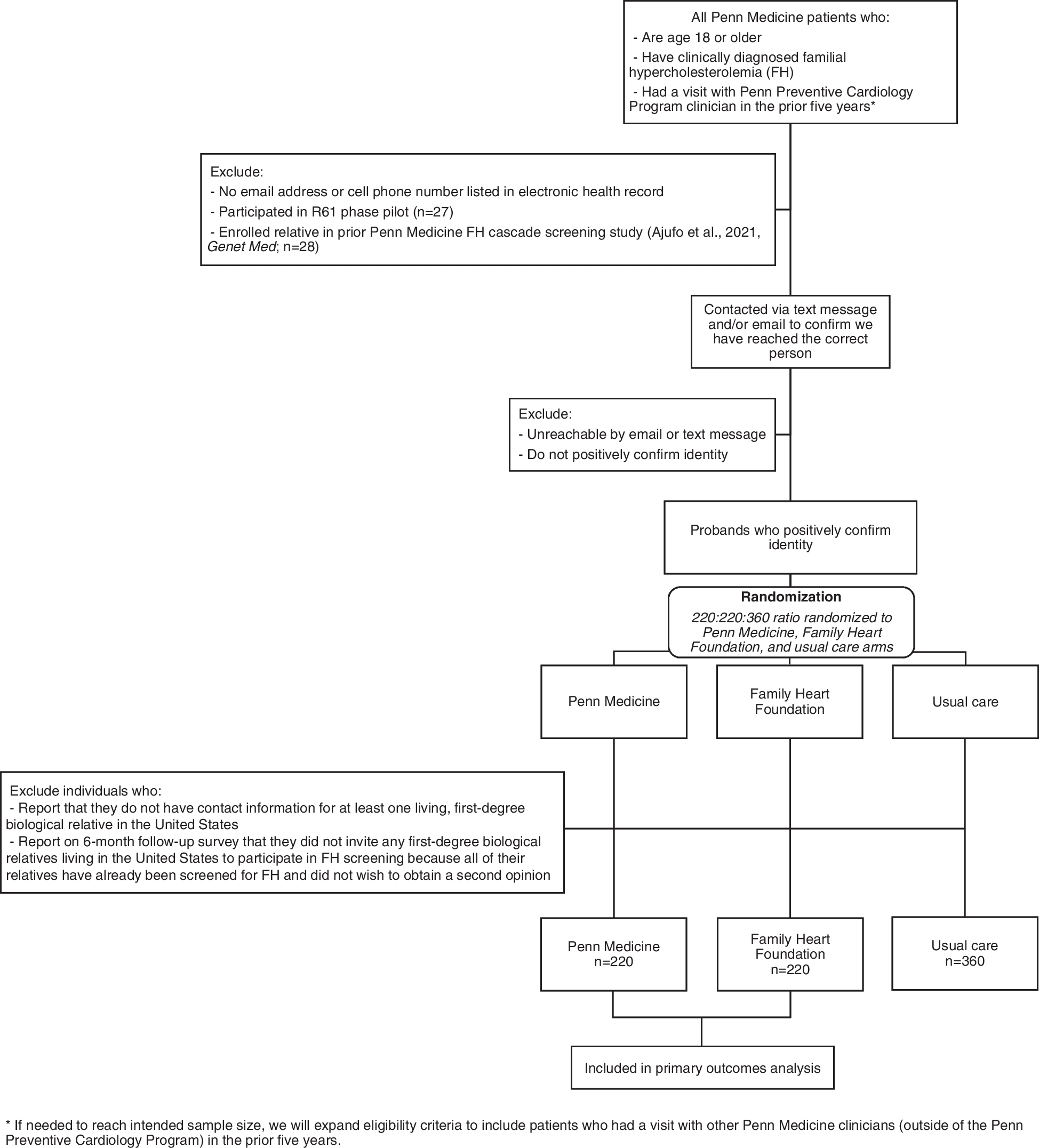








The search and screening results at each stage are shown as a PRISMA flow chart in Fig. 1. We screened unique 1124 titles and abstracts and 113 full-text documents. Of those, 59 original research papers met the eligibility criteria. The full list of included studies can be found in Additional file 2, and the record of excluded full-text studies can be found in Additional file 3.
Fig. 1 Characteristics of sources of evidence
Characteristics of sources of evidenceEight out of 59 included studies used quantitative methodologies, 33 qualitative, and 18 mixed methods. Twenty-four were conducted in the USA, 7 in the Netherlands, 6 in Sweden, and 4 in Canada, Australia, and England. The remaining 10 studies were conducted in other countries. The year of publication ranged from 1998 to 2022 (median = 2017). The study aims reflected high variability in the scope of investigations, ranging from those interested in implementation processes and evaluation, through stakeholder perspectives and experiences, to comparative and regional analysis. Descriptive data about the included studies are presented in Table 1.
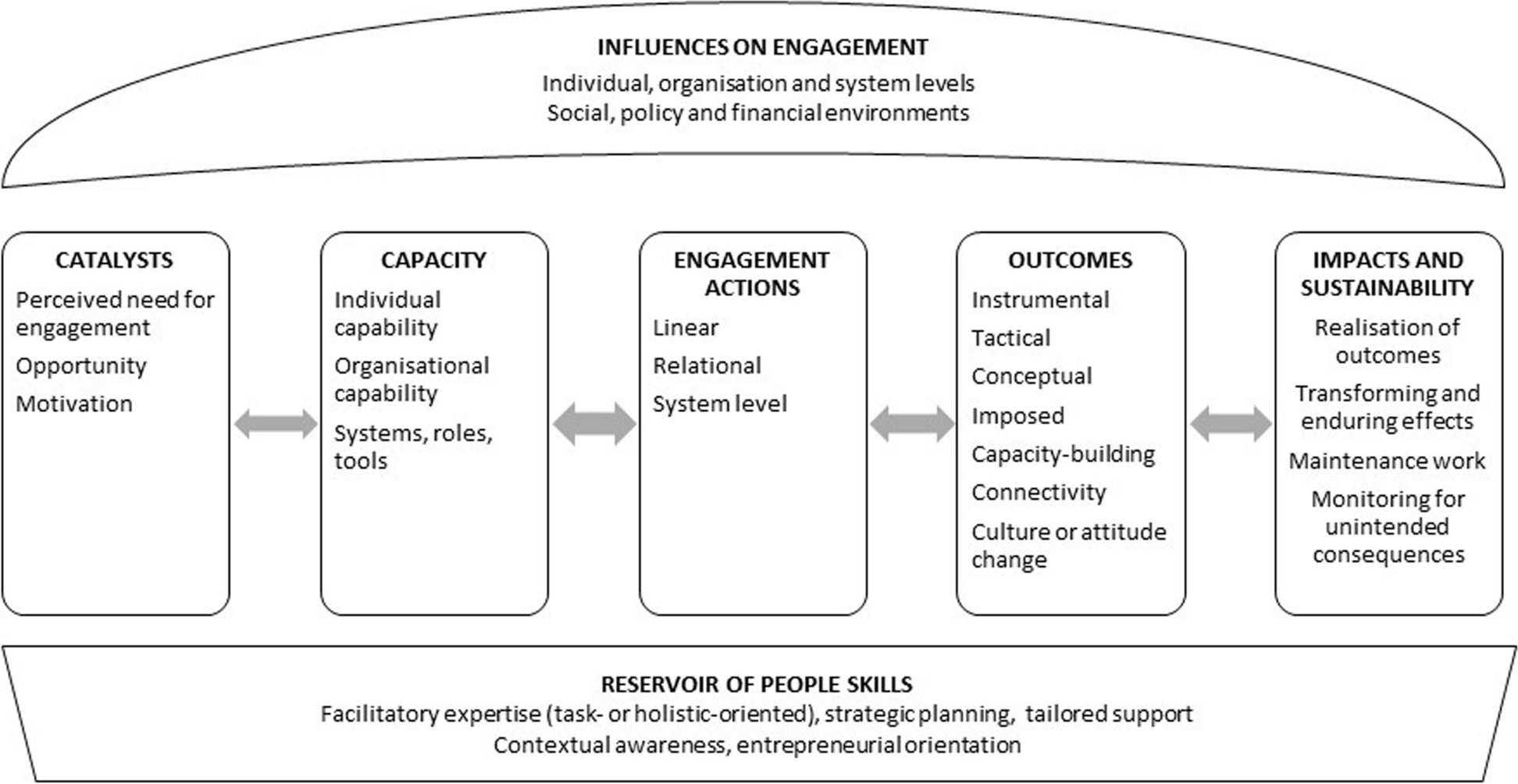
Table 1 Descriptive characteristics of included studiesTable 2 displays the characteristics of evidence sources, presenting the frequency of observations and the sources by thematic categories. Table 2 also shows the frequencies of observations for each determinant cross-tabulated by each implementation outcome. Implementation stood out as the dominant outcome, covered in 46 articles, while adoption and penetration/reach were discussed in 29 and 26 of the articles, respectively. Sustainment found the least attention (n = 16). The data prominently showcased local determinants, including work infrastructure (n = 34), mission alignment (n = 33), and culture (n = 29), emphasizing their significance in the adoption and implementation phases. Of these, mission alignment was highly prevalent in sustainment articles. The concept of agency leaders was discussed in 38 articles, and their role was highly present in adoption, implementation, and sustainment articles. Researchers (n = 11) and political/administrative decision-makers (n = 25) were most frequently cited in articles concerning sustainment and penetration/reach. They had in common their frequent association with national strategies (n = 25), while the former was more often associated with evaluation, monitoring, and feedback (n = 25) and the latter with financing (n = 41). Discussion on sustainment and penetration/reach also frequently associated with national strategies, legislative context (n = 31), and financing. External support professionals (n = 20) were relatively highly represented in the articles on sustainment. Figure 2 is a diagram that depicts the relative positions of categories and directions of influence between them in a conceptual model.
Table 2 Frequency of observations and sources of evidence: frequencies presented in total and divided into facilitators and barriers by implementation outcomeFig. 2
Associations between the systems of evidence-to-practice, external contextual determinants, and implementation outcomes: a conceptual model
External contextual determinantsPolicies and laws: national strategies and systemic integrationNational or regional strategies were described as promoting the uptake and implementation of IPS [38] and appeared to be backed by administrative decisions about responsibility-sharing or funding. These policies included national mental health strategies [39], guidelines [40], and agreements on implementation support issues [18, 19]. The IPS model was perceived as a contributor to the strategic goal of implementing the recovery approach and serving as a vehicle for producing system reform at national and regional levels [18]. Congruence with other national policy goals and frameworks, such as social inclusion [39] and participation [41], was found to facilitate the incorporation of IPS principles into national mental health care policies. Systematic approaches in providing implementation support could support national strategies [42] whereas a mismatch between overarching national strategies and a lack of programs to implement IPS to achieve the goals of these strategies was reported to lead to lower penetration or adaptation of the IPS model [39, 43, 44].
One feature of the national strategies was the aim of expanding the clientele from persons with severe mental disorders such as psychotic disorders to those with any mental disorder, leading to implementing IPS in various care settings, e.g., forensic or psychiatric housing programs [45, 46]. The implications of different work infrastructures on implementation are discussed in a separate section below (work infrastructure).
Policies and laws: legislative contextLegislative contexts concerning mental health and employment were reported to impact the implementation of the IPS model. Laws that mandate employment services for individuals with severe mental illness [47] or policies redirecting services from activities not following the IPS model [48] increased the adoption of IPS programs. On the other hand, the availability of competing practices [49,50,51], procedures mandated by policies but not supported by research, such as work capacity assessments [52,53,54] or mandated lengthy referral processes [54], were reportedly at odds with the implementation of IPS with adherence to model guidelines. Social insurance criteria that excluded clients based on expected employment outcomes [55] or received benefit types [56] were also reported as barriers. The policy of allocating decision-making and management of services to local authorities was reported to hinder adoption due to low prioritization at the local level [41]. Laws and regulations related to sharing client information and access to data and mandated use of multiple information systems were reported to complicate the implementation of IPS [44, 57, 58]. Legally mandated limitations on using data could be circumvented by strategic actions by the administrative authorities or local leaders [18, 44].
FinancingThe availability of funding was critical for adopting and implementing IPS across the settings. National or regional development projects were often used in the adoption phase [59, 60]. Sustained direct funding schemes through health ministries or other governmental organizations were used to increase the use or adoption within the service system or provide the necessary flexibility to implement the model as intended at the local level [38, 48, 60]. A state-level funding mechanism was associated with statewide uptake of the model [49]. Payments based on achieved results were reported to facilitate sustained implementation [49, 61]. Many studies reported that a well-managed transition from projects to sustained programs was a critical period.
Specific funding mechanisms were reported as barriers to the successful implementation of IPS. Payment models that were based on specific medical diagnoses rather than outcomes [62, 63] and separate or divided sources of funding [18, 41, 42, 51] hindered the implementation. Set or predefined funding duration to funding [41, 46, 57, 59, 64], restrictions on financing employment services as health services [51, 65], and rules that penalize short employment contracts [51] were also perceived to impact the quality of implementation negatively. Funding contracts covering a broader set of programs could include criteria conflicting with the IPS fidelity criteria [50, 63].
Training and technical assistanceTraining and technical assistance were reported to facilitate the implementation of IPS. Sources for training and assistance included support from national, state, and regional organizations [66, 67] and IPS/EBP development projects [42, 68], as well as openly available guidelines and training material provided by the program’s developers [55]. These supports reportedly helped those putting the model into practice with goal setting and providing a sense of purpose [44, 50], helped providers to work systematically according to protocols and improved their knowledge of evidence-based practices [44, 68], and provided opportunities to share knowledge and experiences with other sites [55]. Agency leaders [44] and staff [62, 69] were reported to benefit from initial training and assistance [65].
Evaluation, monitoring, and feedbackNational, state, and regional organizations [19, 42, 67] and outside experts were used to conduct evaluations and monitoring of the implementation of IPS that were often reported in conjunction with training and technical assistance. Routinely assessing implementation was perceived to help ensure that the model is implemented as intended over time [62], and imposing continuous evaluation by agency leaders may increase the probability of the sustainment of the program [70]. In some cases, fidelity above a certain threshold was used as a prerequisite for funding by national or regional decision-making organizations [71]. Disseminating the results on the effectiveness of IPS reportedly increased the model's adoption [18], and evaluations and monitoring were used to motivate leaders to maintain or reinstate high-fidelity services [40]. In contrast, the lack of results from monitoring or evaluations could discourage agency leaders from following national guidelines that promoted the use of IPS [46].
Local factors affected by external contextMission alignmentBoth the recovery approach [41, 59, 63, 72] and evidence-based policy commitment [69, 73] were reported to facilitate the reorienting of organizational goals to be consistent with IPS implementation and sustainment. The shift in organizational goals was associated with the de-implementation of vocational services that lacked evidence-based support and were supported by structural changes and financial arrangements through administrative decisions [74].
The non-alignment with organizational goals was reported to hinder the model’s implementation. The model could be at odds with existing organizational goals based on traditional medical or vocational services [75, 76]. These goals could be mandated by existing rules and regulations [53]. Challenges were reported when collaborating partners from different organizations had different goals in their respective organizations [52, 53, 60, 77], which could lead to giving lower priority to collaborating with the IPS team [52, 70].
CultureAcceptance of the model by the professionals, professional norms, and local attitudes was reported as important for the uptake and implementation of the model. Understanding the program logic [60, 73] and recognizing unmet user needs [72, 78] were associated with the changes in acceptance of the model and professional norms. Several studies found that influencing practitioners’ professional norms and attitudes was an important goal during the adoption period. During this time, practitioners could learn about the rights and needs of users, the benefits of IPS, and community resources; changes in these attitudes would lead to better implementation results [55, 58, 72,
留言 (0)