
記住我



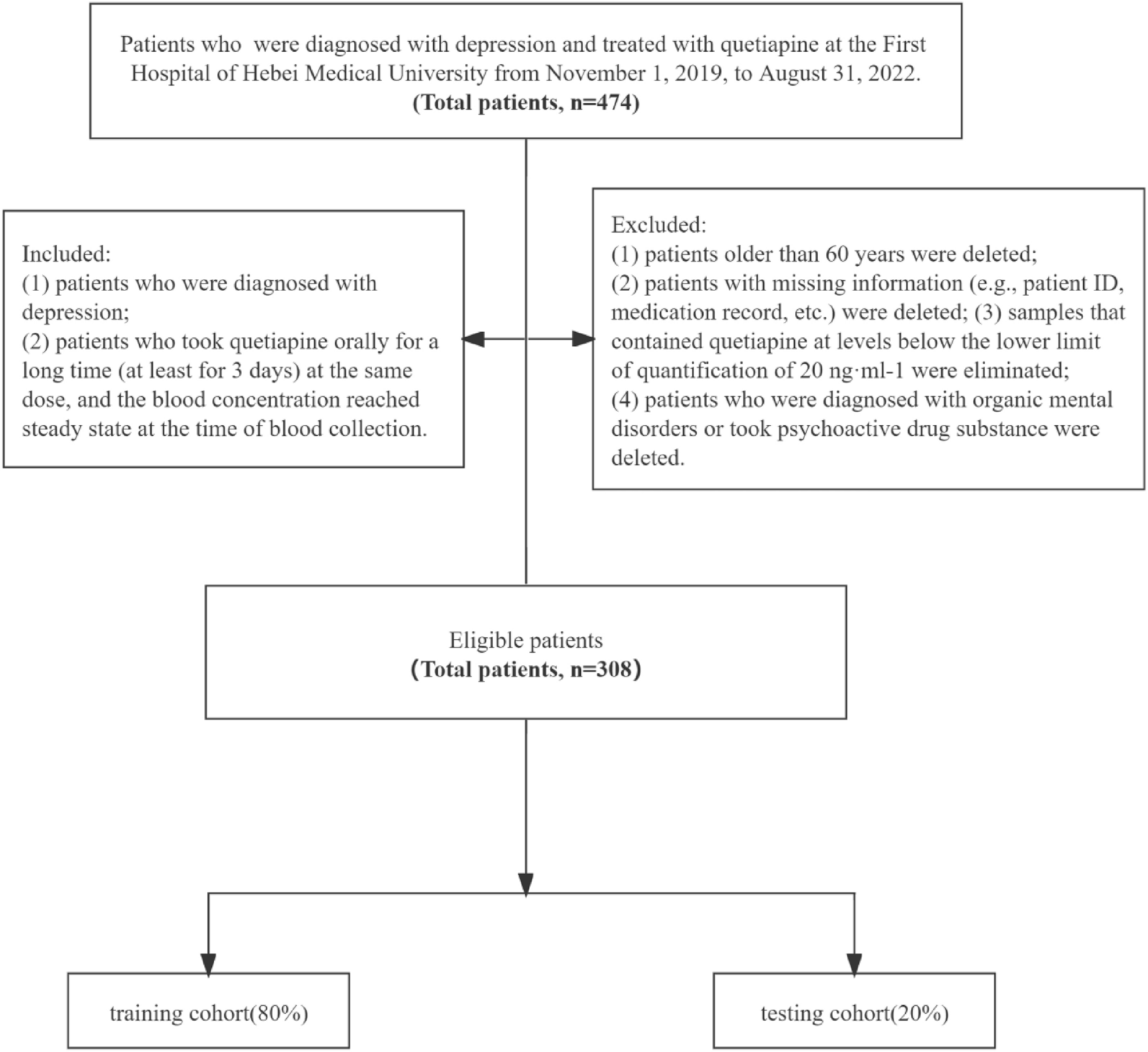
Between March 1, 2019, and June 30, 2019, at ten tertiary psychiatric specialty hospitals in Zhejiang Province, based on the number of depression patient visits and referring to inclusion/exclusion criteria, a fixed quota, competitive continuous enrollment method was employed, culminating in the inclusion of 180 patients with active depression. Utilizing a computer-generated random numbering system, 180 sequences ranging from 1 to 180 were produced. Odd numbers were assigned to the agomelatine group, while even numbers were allocated to the SSRIs group. Based on the random sequence outcomes, the 180 patients were divided into the agomelatine group and the SSRIs group, with 90 patients in each group. No specific medication was prescribed for the SSRIs group, and dosages did not exceed the recommended maximum dosage outlined in the drug manuals. At baseline, demographic data such as age, gender, and Body Mass Index (BMI) were collected from enrolled patients, along with the administration of related scales for assessment. For a detailed research procedure, refer to Fig. 1.
Fig. 1 Inclusion and exclusion criteria, and criteria for withdrawal
Inclusion and exclusion criteria, and criteria for withdrawalInclusion Criteria: (1) Patients diagnosed with a depressive episode based on the International Classification of Diseases 10th Revision (ICD-10); (2) Diagnosis conducted using the Chinese version of the Mini-International Neuropsychiatric Interview (MINI); (3) Patients in the acute phase of a depressive episode with a total score of ≥ 17 on the HAMD-17 and a score of ≥ 3 on the Clinical Global Impression-Severity (CGI-S). Patients can be either first-episode or recurrent cases, and they should not have received antidepressant treatment or undergone Modified Electroconvulsive Therapy (MECT) or other physical therapies within the 2 weeks prior to inclusion. (4) Of Han ethnicity, both genders are acceptable, aged between 18 and 65 years; (5) Patients who have signed an informed consent form.
Exclusion Criteria: (1) Patients diagnosed with schizoaffective disorder, dysthymia, or bipolar depression; those primarily diagnosed with any other anxiety disorder within the last year; individuals with substance dependence; or those with personality disorders. (2) Carriers/patients of hepatitis B or C viruses; those with liver function abnormalities, cirrhosis, or active liver disease; (3) Patients with serious cardiac, cerebral, renal, or endocrine organ diseases or any other significant physical ailment. (4) Patients for whom previous standardized treatment with agomelatine was ineffective, or those who have been unsuccessfully treated with a full dose and full course of ≥ 2 antidepressants during the current episode. (5) Patients whose current depressive episode has lasted for more than 2 years. (6) Those with evident suicidal intentions or behaviors, with a score of ≥ 3 on the third item (suicidal thoughts) of HAMD. (7) Lactating or pregnant women, or those planning to conceive during the trial period, or those unable to employ safe and effective contraceptive measures.
Withdrawal Criteria: (1) Patient revokes their informed consent; (2) Non-compliance with study medication or therapeutic interventions during the research; (3) Persistent elevation of alanine aminotransferase (ALT) levels exceeding three times the upper limit of normal that cannot be ameliorated by hepatoprotective medications; (4) Emergence of manic shift, psychotic symptoms such as hallucinations or delusions, or disorders of consciousness; (5) Pregnancy.
This study was approved by the Ethics Committee of Huzhou City's Third People's Hospital (Ethical Approval Number: 2019 Ethics Review No. 028). All research participants or guardians are required to sign an informed consent form before participating in the study.
Medication protocolPatients in both groups were administered variable doses of agomelatine tablets (Jiangsu Hansoh Pharmaceutical Co., Ltd., National Medicine Approval No. H20143375, Batch No.: 160901. Specification: 25 mg/tablet) or SSRIs (including: Citalopram, Escitalopram, Paroxetine, Fluoxetine, Sertraline).
The study group received agomelatine tablets with an initial dose of 25 mg/day, taken once daily before bedtime. Two weeks later, based on the patient's therapeutic response and tolerance, the dosage may be adjusted to 50 mg/day, taken once daily before bedtime. The control group was treated with SSRIs. The specific choice of medication was not mandated, with all doses based on the recommended starting doses in the drug's package insert, taken once daily after breakfast. Subsequently, depending on the patient's individual response to the medication and the drug's half-life, the drug dosage can be titrated every 1–2 weeks, but the maximum daily dose should not exceed the recommended limit mentioned in the package insert.
During the study, symptomatic treatment can be administered for adverse reactions caused by the medication. Medications that were being used to treat existing somatic diseases before study inclusion can continue to be co-administered. However, during the study period, concomitant use of other antidepressants, anti-anxiety medications, antipsychotics, mood stabilizers, thyroid hormones, etc., is prohibited. The use of any systemic psychotherapy other than supportive psychotherapy is not allowed, nor is the use of MECT or other physical therapies. If necessary, short-term combined use of low-dose benzodiazepines or zopiclone is permitted but not for more than a week, to avoid affecting the observation and analysis of the patient's inherent circadian rhythm.
Primary research toolsIn addition to employing scales such as HAMD-17, HAMA, and PSQI, the following instruments were also utilized:
The SHAPS [22] is a tool for assessing anhedonia, encompassing domains of interest/entertainment, social interaction, sensory experience, and eating. It comprises 14 items, with a total score ranging from 14 to 56. A higher score indicates a greater degree of anhedonia.
The MFI-20 [23] consists of five dimensions: general fatigue, physical fatigue, reduced activity, reduced motivation, and mental fatigue. It encompasses 20 items, with scores ranging from 20 to 100. A higher score signifies a higher level of fatigue.
The MEQ [24, 25] is an instrument for categorizing the natural inclination of sleep/wake circadian rhythms. The questionnaire contains 19 items, with scores ranging from 16 to 86. Scores of 16–41 indicate evening-type, 42–58 intermediate-type, and 59–86 morning-type. A higher score indicates a higher degree of morningness, while a lower score indicates a higher degree of eveningness.
Efficacy and safety assessmentAt baseline and at the ends of weeks 2, 4, 8, and 12, patients were assessed using HAMD-17 and HAMA; simultaneously, patients conducted self-evaluations using SHAPS, MFI-20, MEQ, and PSQI. Among these, the SHAPS, MFI-20, PSQI, and MEQ scales were designated as primary efficacy indicators, while the HAMD-17 and HAMA scales were set as secondary indicators.
Throughout the treatment, descriptive records of various patient complaints and observed adverse reactions were maintained and evaluated using the TESS, a tool for assessing the frequency and severity of adverse reactions caused by the medication. TESS consists of 24 items that ranging from 0 to 4 scores, with a higher score indicating a more severe adverse reaction. At baseline and at the ends of weeks 4, 8, and 12, routine blood tests, urinalysis, liver and kidney functions, thyroid function, a complete set of sex hormones, and electrocardiograms were conducted.
Psychological scale assessments were carried out by two physicians from each center with intermediate or higher professional titles in psychiatry. Unaware of the patients' group allocations, they conducted cross-over blind assessments, achieving a consistency test Kappa value of 0.89.
A reduction rate of > 50% in the HAMD-17 total score pre- and post-treatment was deemed effective, and a HAMD-17 total score ≤ 7 was considered clinical recovery. An increase in serum ALT or AST levels beyond the upper limit of the normal range indicated liver function abnormality, while an elevation of serum ALT or Aspartate Aminotransferase (AST) greater than three times the upper limit of the normal range was considered a significant liver function abnormality.
Statistical methodsStatistical analysis was performed using SPSS 22.0 software. The study employed a full analysis set (FAS) for data analysis, using the last observation carried forward (LOCF) method to supplement missing data, such as scores from HAMD-17, HAMA, SHAPS, etc. Quantitative data were expressed as mean ± standard deviation (x ± s). Inter-group mean differences were analyzed using the t-test. Count data and remission rates were expressed in frequencies (percentages) with inter-group rate comparisons made using the χ2 test. As baseline scores and center-specific effects could influence subsequent score changes and inter-group differences, and considering that baseline scores were assessed before the intervention, the baseline values of HAMD-17, HAMA, SHAPS, MFI-20, MEQ, PSQI scales, and individual center effects were treated as covariates. Repeated measures analysis of variance was conducted to compare group effects on the scores from these scales at various visitation points. If the sphericity assumption wasn't met, a Greenhouse–Geisser test was conducted after adjusting degrees of freedom. The test level α was set at 0.05.
留言 (0)