
Remember me





In Japanese zoos and zoological parks, measures are taken to prevent people from directly confronting big cats such as tigers and lions. However, in prior accidents, individuals have been attacked by big cats due to human errors. Big cat bites are highly lethal due to the enormous bite force of these animals [1].
We report on the trauma and psychological management of a young female zookeeper who sustained severe facial trauma and posttraumatic stress disorder from a tiger bite.
Case presentationIn Japan, 2022 was the year of the tiger. Therefore, many spectators were expected to visit the safari park to see tigers. In the morning just before the gate opened, a 26-year-old female keeper who had worked 2 years there opened the passageway door and was faced with a tiger, which was supposed to have been placed in the cage the previous night. The Bengal tiger was 2 m long and weighed 150 kg. The keeper was attacked from the rear when she momentarily turned her back. First she was bitten on the head, knocked down on the spot, dragged for 3 m, and then bitten several times on her chest and abdomen. She was moved away from the tiger by another keeper and an ambulance was called. After 5 min, the paramedics arrived and provided first aid, such as gauze compression, after which she was directly transported to our university hospital by an ambulance helicopter. Upon presentation, Glasgow Coma Scale was E3V4M6 and respiratory rate was 36/min. Tetanus toxoids 20 IU and immunoglobulins 250 U were administered to prevent infection. Due to persistent bleeding from the head (hemoglobin 10.8 g/dL) and decreased systolic blood pressure to 70 mmHg, an emergency blood transfusion was performed. The patient required 6 units of packed red blood cells and 6 units of fresh frozen plasma. Further, tracheal intubation by rapid sequence intubation was then performed.
The results of the clinical examination were as follows: Head and face: multiple lacerations on the right midface, both sides of the neck, around the ears, and on both sides of the back of the head due to tiger bites (Fig. 1); the occiput showed a degloving injury on the pericranium, leaving a gap of 5 cm in the center. Chest and back: an open wound measuring approximately 10 cm on the right anterior chest, and the mammary gland had prolapsed; some bite wounds were on the back. Abdomen: an open wound in the lower right abdomen. Extremities: lacerations due to bites on the left thigh and right thumb.
Fig. 1
Multiple lacerations in the head and face area
In the initial computed tomography (CT) scan revealed multiple open facial fractures (orbital floor, medial wall fracture, right maxillary comminuted fracture, right zygomatic fracture, nasal bone fracture, anterior skull base fracture, left orbital medial wall fracture, and left maxillary fractures) and pneumoencephalopathy due to the disruption of the frontal and ethmoid sinuses and the entire skull base (Fig. 2A, B). There was a small pneumothorax on the right side (Fig. 2C). A small gas image was detected in the abdominal cavity; however, no organ damage was observed. There were fractures in the C1 cervical transverse process fracture (Fig. 3) and the T12 and L1 spinous processes (Fig. 4). No vascular injury was observed. A 28Fr chest drain was placed in the right thoracic cavity, and a Penrose drain was placed in the abdominal cavity. Wounds found on the chest, abdomen, and extremities were washed and sutured. The initial prophylactic antibiotic was sulbactam/ampicillin for 9 days in the absence of a wound infection.
Fig. 2
Computed tomography (CT) images. A 3D reconstruction of the initial CT scan showing multiple open facial fractures. B Head CT scan showing pneumoencephalopathy due to disruption of the frontal sinus (arrow). C Chest CT scan showing a small pneumothorax on the right side
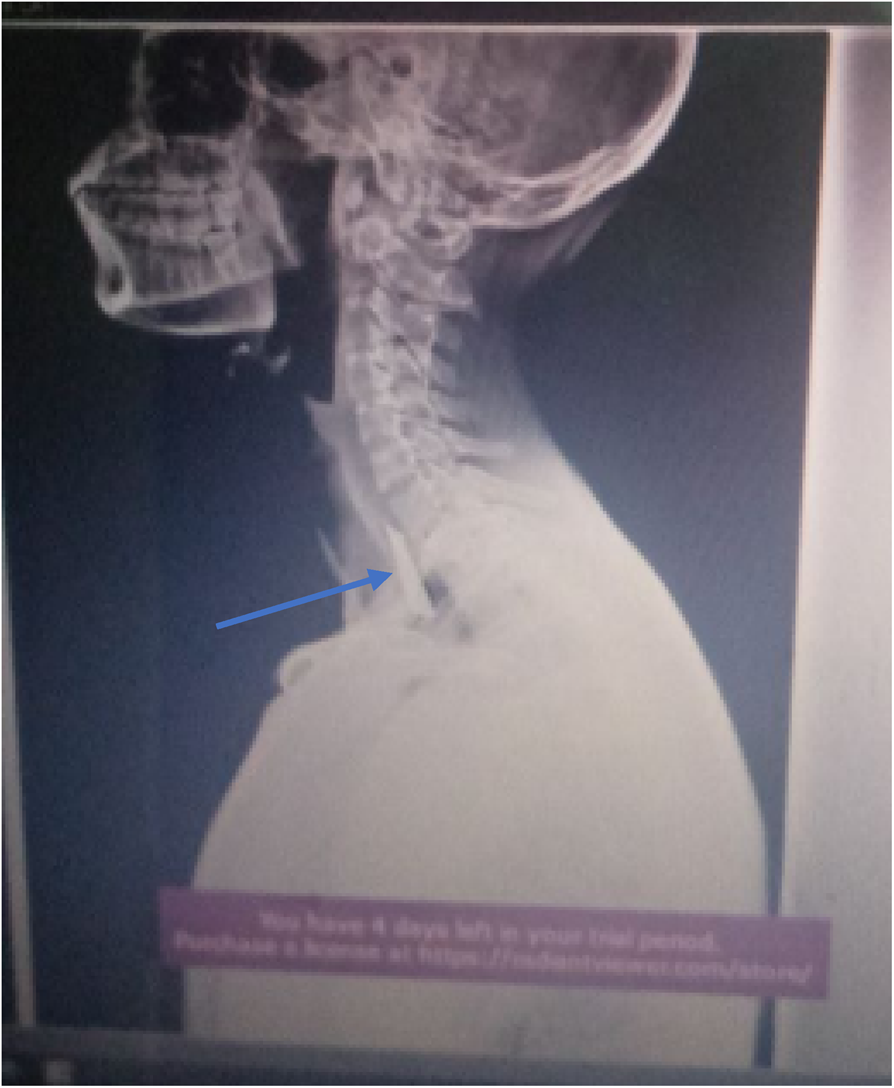
Fig. 3
Cervical spine computed tomography scan: C1 cervical transverse fracture (arrow)
Fig. 4
Thoracolumbar spine computed tomography scan: T12 and L1 spinous process fractures
Emergency surgery was initiated 5 h after arrival at the hospital. A large amount of saline was used to wash the head and face to remove as many fine bone fragments as possible. The prolapsed right eyeball was restored due to optic nerve damage, and the upper and lower bulbar conjunctiva were intact and maintained continuity; however, the eyeball was exposed due to contracture of the right upper eyelid. To maintain the facial shape, only the third largest bone fragment was fixed to a titanium plate. The right zygomatic frontal suture was fixed using a straight 6-hole microplate with a 4-hole 5 mm screw. The suprafrontal suture was fixed with a 4-hole 5 mm screw in a 5-hole Y microplate. The bilateral full-thickness injury of parotid gland and masseter muscle injury were suspected to result in bilateral facial nerve palsy. Skin suturing was performed without soft-tissue repair. No skin defects were observed.
Two Penrose drains were placed in the right anterior chest and one in each of the left lower abdomen, left hip, left groin, and left ilium.
On the day after the surgery, the patient was extubated. Two days after the surgery, enteral nutrition was initiated, and the chest tube was removed. Three days postoperatively, the patient experienced nightmares, underwent psychiatric treatment, and was diagnosed with an acute stress reaction; eszopiclone 3 mg was initiated. Oral intake was initiated on the fifth postoperative day, and the patient was discharged from the intensive care unit.
Fourteen days after the injury, open reduction of the zygomatic fracture was performed. In addition, because the eyelid could not be closed on the right inner canthus side, orbital and nasal bone reconstructions were performed. The patient was doing well and was discharged 21 days after the injury.
The patient was readmitted to the hospital and underwent surgery for removal of the right mandibular muscle process and right mandibular scar in the Oral Surgery Department because of concomitant contracture-induced trismus. After that, she continued to visit the hospital, and although the root of her nose was slightly shifted to the right side, she regained her cosmetic appearance and her oral intake has improved (Fig. 5).
Fig. 5
Postoperative result after 7 months show the root of her nose was slightly shifted to the right side
Five months after being discharged from the hospital, she began complaining of flashbacks and nightmares of the scene at the time of the accident. The patient was diagnosed with posttraumatic stress disorder by a psychiatrist and started on sertraline 50 mg and has been improving since then.
Regarding facial nerve palsy, only the mandibular branch remained on the right side, and only the mandibular branch was completely paralyzed on the left side. Right buccinator muscle branch reconstruction surgery was considered; however, 7 months after being discharged from the hospital, he was able to lift his right eyebrow, and the movement of the orbicularis oris muscle also improved.
Comments (0)