
記住我
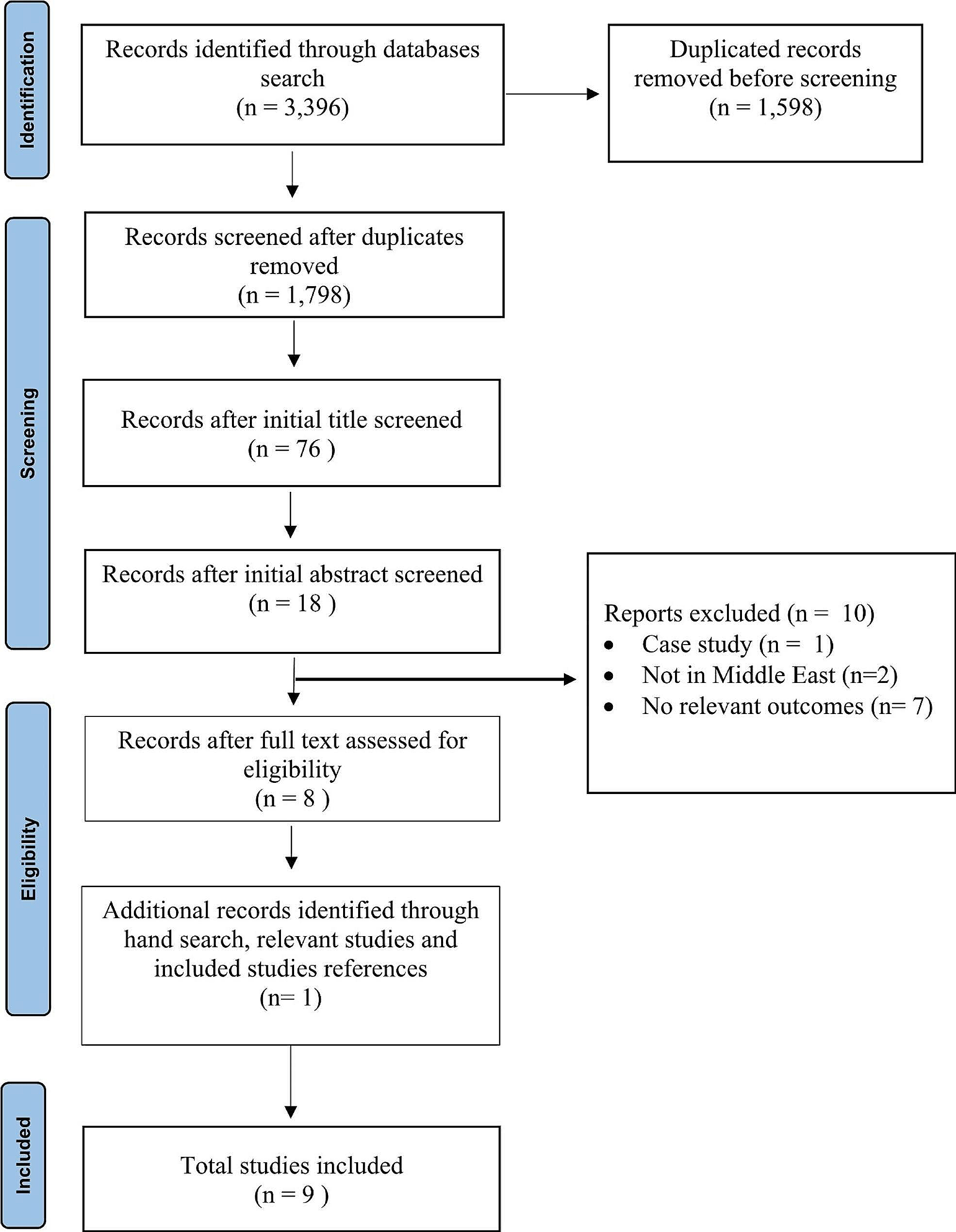







The search strategy identified 10,873 references, although only 166 full text articles were retrieved (Fig. 1). Thirty-seven studies were identified from the database searches and had their data extracted [2, 17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52]. Another six studies were identified from handsearching / researcher’s bibliography [53,54,55,56,57,58]. The studies identified included 23 generic symptom studies [18, 20,21,22, 25, 26, 29,30,31,32, 40,41,42,43,44,45,46,47, 52,53,54,55,56], eight symptom cluster studies [34,35,36,37,38,39, 57, 58], nine oral symptom / problem studies [17, 19, 23, 24, 27, 28, 33, 50, 51], and three xerostomia-specific studies [2, 48, 49]. Several “duplicate” records were identified amongst the retrieved full text articles: some were conference abstracts, some articles reporting “early” results, and some articles reporting different analyses / subsets of results. Table 1 shows studies reporting clinical features of xerostomia in patients with advanced cancer, and includes references for relevant assessment tools [59,60,61].
Fig. 1 Table 1 Studies reporting clinical features of xerostomia in patients with advanced cancerAssessment
Table 1 Studies reporting clinical features of xerostomia in patients with advanced cancerAssessmentThe three xerostomia specific studies involved small numbers of patients (median: 70; range: 16–120) [2, 48, 49]: two were quantitative (with one using a validated / non-specific assessment tool, i.e. Memorial Symptom Assessment Scale / MSAS) [2, 48], whilst one was qualitative [49]. The nine oral symptom / problem studies involved somewhat larger numbers of patients (median: 104; range: 50–669) [17, 19, 23, 24, 27, 28, 33, 50, 51]: all were quantitative (with three using validated / non-specific assessment tools, i.e. Oral Symptom Assessment Scale / OSAS, Edmonton Symptom Assessment System / ESAS—Norwegian version, and MSAS) [17, 28, 50]. It should be noted that there is no validated xerostomia assessment tool for this cohort of patients.
EpidemiologyXerostomia prevalence varied widely in the studies identified in this review (median: 72.15%, range: 40.4–91.0%). Alsirafy et al. reported that only one patient reported this symptom on open questioning, although 57% patients gave a positive response on systematic assessment (with 43% of these patients reporting “moderate” / “severe” intensity) [22]. Other authors reported similar findings in this group of patients [62].
The identified studies reported minimal information on the risk factors for xerostomia (e.g. demographics, cancer diagnosis, performance status, comorbidities). There is some data to suggest that xerostomia may be more prevalent in females [20, 40], in younger patients [41], and in Caucasians versus African Americans in this population [42].
Xerostomia appears to be common in all groups of patients with cancer, including patients with haematological malignancies [23, 43], and patients with sarcomas [44]. There is better data to suggest that xerostomia is more prevalent in patients with a poor performance status [45, 46], and equally that xerostomia is more prevalent in patients at the very end-of-life [31, 47]. However, the association between xerostomia and limited prognosis is inconsistent [63].
The identified studies also reported minimal information on the aetiology of xerostomia. Davies et al. (2001) reported 97.5% patients were receiving medications that are known to cause xerostomia, and that the median number of such drugs used was 4 (range 0–9) [2]. Other authors have reported an association with the use of anticholinergic drugs [41], opioid analgesics [41], and chemotherapy drugs [23].
Symptom clustersTable 2 shows studies reporting physical and/or psychological symptom clusters involving xerostomia [34,35,36,37,38,39, 57, 58]. The symptom clusters identified varied from study to study, and also varied within study (depending on the outcome measure chosen, and the statistical method utilised). It should be noted that there are many other studies reporting physical and/or psychological symptom clusters in patients with advanced cancer, but which did not include the symptom of xerostomia [64].
Table 2 Studies reporting symptom clusters including dry mouth in patients with advanced cancerDavies et al. (2021) examined oral symptom clusters, and reported that xerostomia did not cluster with other oral symptoms when using prevalence data, but did cluster with taste disturbance when using frequency data (Spearman’s rank correlation coefficient = 0.6) [17]. No analogous studies were identified in the literature.
Clinical featuresTable 1 shows studies reporting the clinical features of xerostomia. It demonstrates that it is usually a frequent symptom [2, 17, 21, 56], is often moderate-to-severe in intensity [2, 17, 19,20,21,
留言 (0)