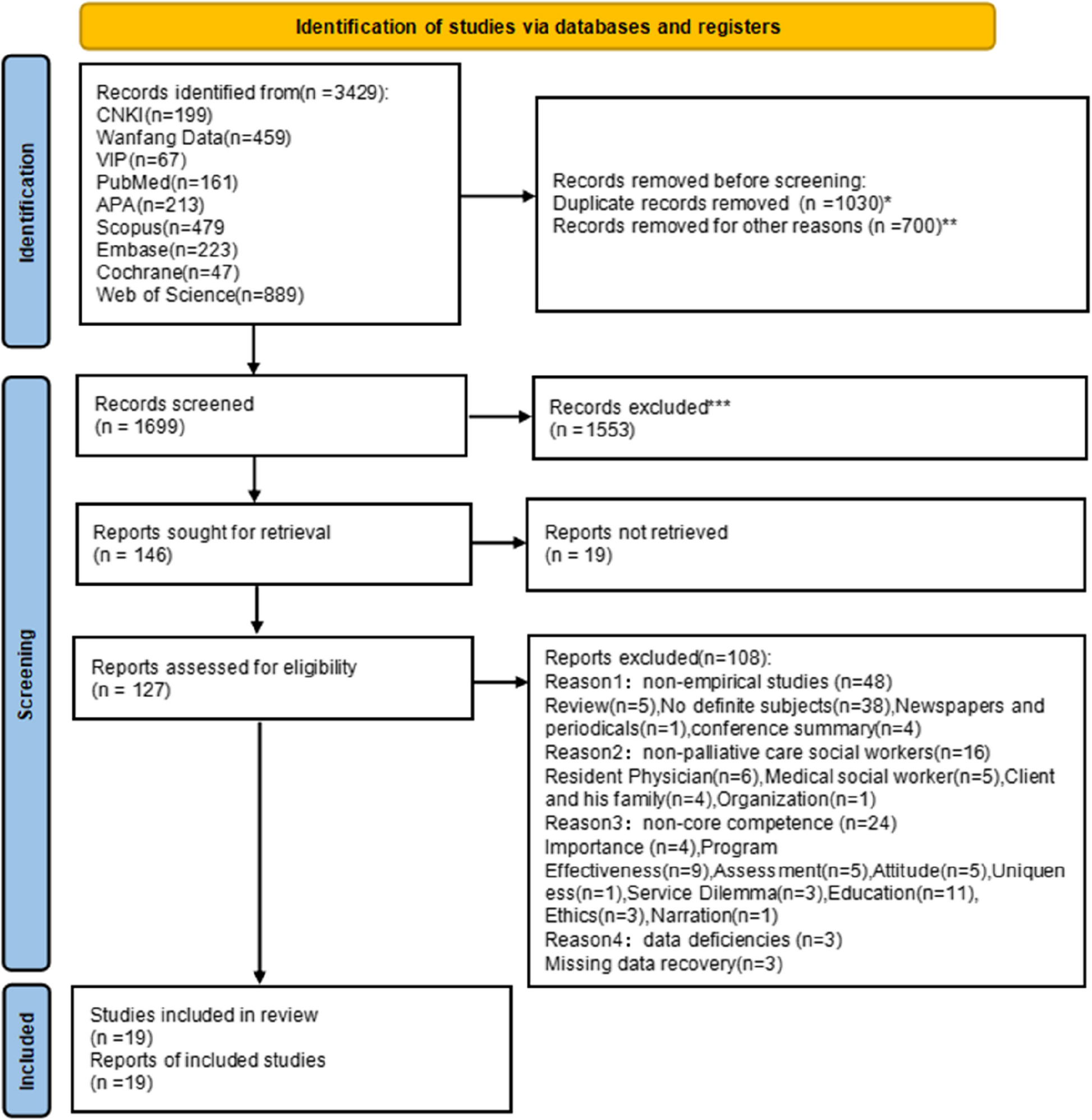
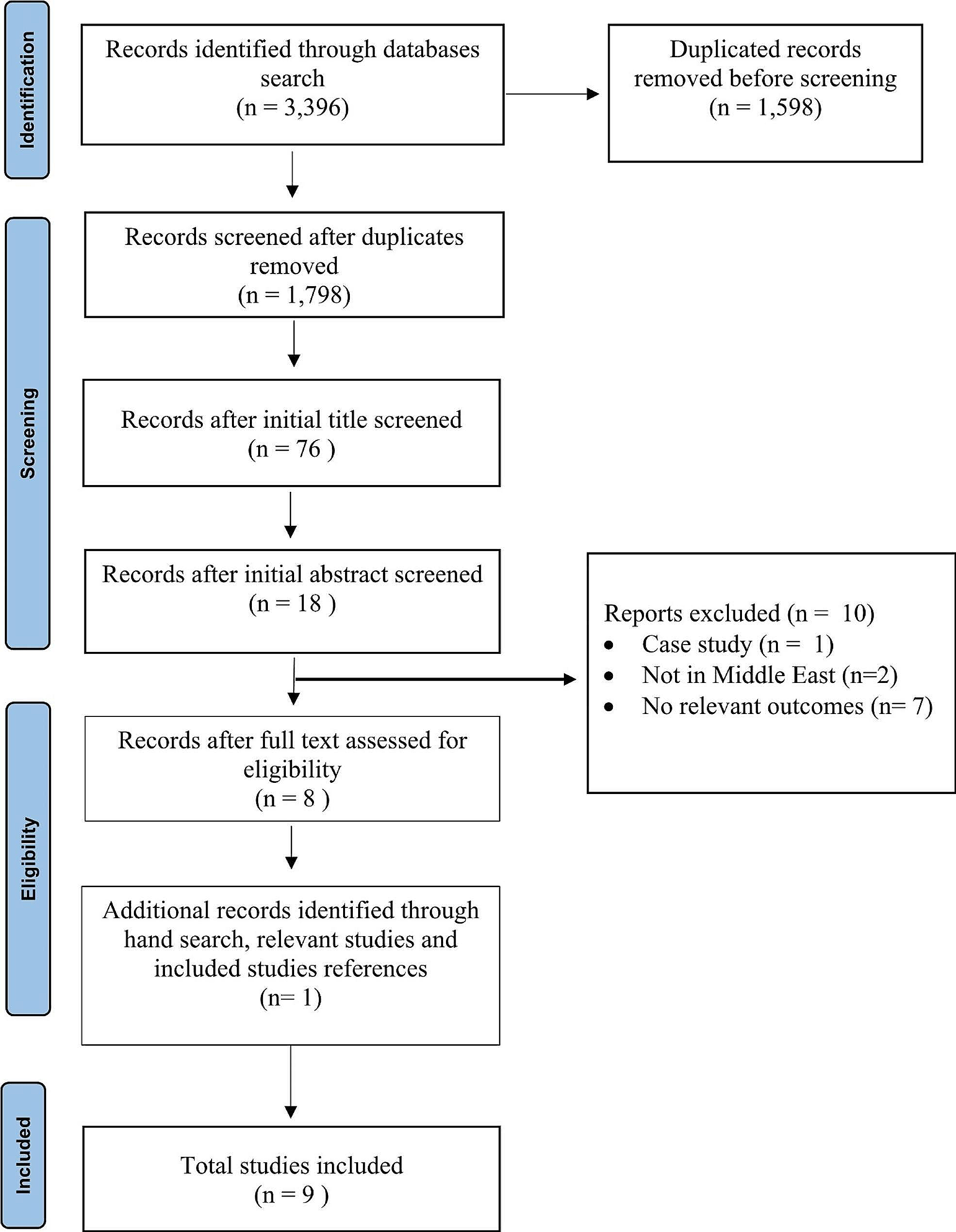
The Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) was utilised as a guide to frame the literature search (See Supplementary Material). The initial database and manual search generated 391 titles and abstracts. After reading all of the abstracts (and full text as necessary), ten studies met the inclusion criteria. All literature that met the inclusion criteria are outlined in Table 1.
Table 1 Published research included in scoping reviewDesign of studies
All studies except one were qualitative and used a range of methods including interviews (n = 2), focus groups (n = 1), ethnography (n = 1) and secondary analysis from previously undertaken research (n = 5). The other study was quantitative. This study used data from a national study to undertake multivariate analyses. The CASP quality appraisal and AXIS tool results for the research included in this literature review are presented in tables (See Supplementary Material S1 and S2). All the studies clearly stated aims for their research and utilised appropriate research designs to address these aims. However, inconsistencies existed in whether the researchers articulated whether ethical issues had been attended to or if the relationship between researcher and participants had been considered. All included research was identified to have made valuable contributions to understanding palliative care in relation to people’s identity complexity.
Countries
The studies included in this review came from a range of countries including USA (n = 3), Canada (n = 5), Nepal (n = 1) and South Africa (n = 1). Whilst eight of the ten studies are in North American countries, we recognise that the range of countries included represent diversity in the type, focus, provision and availability of palliative care and services.
Study samples and participant characteristics
The included literature addressed different groups including Medicare beneficiaries, palliative providers, family caregivers, Black male caregivers, people who are LBGQTI + , people with a diagnosis of HIV/AIDs and, what authors described as, people experiencing ‘structural vulnerability’ [50,51,52,53,54,55,56,57,58,59]. Some researchers involved a variety of participant groups in their studies. Five of the ten studies included participants who were patients (actual or potential), six studies incorporated paid caregivers (carers or health professionals) and five studies included unpaid caregivers (family or other support). Despite the wide variety of people who were researched using an intersectional approach, common topics of power, heterogeneity of people within the health system and barriers to palliative care were illuminated across the studies.
Focus area of studies
Most studies focused on aspects of their participant’s identity in relation to palliative care access and experience. Two studies explored the experiences of people who are LGBQTI + in relation to hospice and palliative care [50, 59]. One of these, by Baskaran and Hauser [49], focused on an NGO care provider who provides a palliative care programme for the LGBQTI + community in Nepal. The other focused on the lived experience of older LGBQTI + individuals in the healthcare system in Ontario, to highlight participant’s concerns associated with end of life [59]. Two studies explored experiences of people who are structurally vulnerable in relation to palliative care [53, 57]. One study by Stajduhar and colleagues [57], explored issues and experiences of accessing palliative care for people experiencing life-limiting illness and structural vulnerabilities. The other study focused on the settings of healthcare provision, how they shape access and experience of palliative care for people who are structurally vulnerable [57]. Hutson explored the health access and end of life concerns for people living with HIV/AIDS in Appalachia, USA [55]. Several studies focused on the intersection of gender and other identities in relation to palliative care [51, 58]. One of these examined the intersectional impact of race and gender on care quality at the end of life [58]. The other by Dworzanowski-Venter [51], focused on the intersection of gendered work norms and class status. This research explored how class and social norms shape the masculine identities of black males working in the feminized role of health caregiver in South Africa. Other studies also explored caregiving in relation to palliative care [52, 54, 56]. One investigated how frontline palliative care providers understand diversity of family caregivers and how this shapes their end-of-life caregiving experience in Canada [52]. Another study focused on socio-environmental factors, and how they facilitate family palliative caregivers’ capacities for resilience in the home setting [54]. Liu and colleagues [55] explored the differences in caregiving burdens for people with dementia across the intersectionality of race and gender.
Interpretation of Intersectionality
See Table 1 for a full articulation of how each researcher defined and/or interpreted intersectionality in connection with their study. Researchers understood intersectionality to be either a theory [53, 58], a framework [56], a lens of understanding [54, 57], an analytical tool [51], or an approach [52]. Three of the studies did not define intersectionality explicitly [50, 55, 59] with two of these only using intersectionality within findings. Hutson recognised intersectionality related to a participant’s lived experience related to the multiple oppressions that they had experienced during their lifetime [55]. Baskaran and Hauser identified intersectionality as a theme within findings which acknowledged the lived experience for people living with multiple, simultaneously oppressive identities [50].
Investigation of intersectionality approach in studies
How each researcher utilised intersectionality in their study has been compiled in the intersectionality identification framework (see Table 2).
Table 2 Investigation of included studies using the intersectionality research integration identification frameworkThere was difference across the studies regarding the extent to which researchers integrated intersectionality. The studies by Dworzanowski-Venter [51] and Liu and colleagues [53] utilised intersectionality as a theoretical framework underpinning the study and it was integrated into the research question, design, analysis, findings and discussion. Suntai and associates [58] used also used intersectionality as a theoretical framework underpinning their quantitative study. They employed univariate, bivariate and multivariate analyses to uncover intersectional interactions between race, gender and quality end of life care. The three studies by Giesbrecht and colleagues were secondary analyses of larger data sets where intersectionality was not part of the original objective [52,53,54]. All applied intersectionality in the analysis phase. Stajduhar and colleagues [57] utilised intersectionality as underpinning their definition of structural vulnerability and in the analysis to explain the complex interactions between social difference and identity. Three of the ten research studies identified intersectionality only as a theme or aspect in the findings or discussion [50, 55, 59].
Findings related to intersectionality, access and experience of palliative care
There was wide recognition across the studies that palliative care services and health systems (across and within different countries) are complex, siloed and often difficult to navigate. Services often do not easily cater to the heterogeneity of people that they aim to serve, especially when people ‘do not fit’ societies’ norms or expectations. Several studies identified that the experience of multiple intersecting stigmatised identities for people is linked with differing kinds of struggles in life and results in often diverse end of life needs and preferences [50, 53, 57]. Being different and having differing needs to the normative stereotypes of a patient can cause people to become ‘invisible’ to the health system [53, 57, 59]. Moreover, identities outside the norm may not be openly acknowledged, welcomed or advocated for by health professionals [50, 53, 55, 57, 58]. Subsequent fear of discrimination, being judged around lifestyle and associated lowered self-worth leads people to avoid seeking care [53, 55, 59]. This alongside with structural/system stigma means options for accessing and receiving palliative care for these people become limited [53, 57]. For example, two studies identified that palliative care services were often discontinued for people when they or their contexts were deemed ‘risky’ [53, 57]. Stajduhar and colleagues [52] recognised that social services often then attempted to fill the health system care provision gaps when care was denied. This often involves working outside policy and practicing covertly to ensure care needs are met.
Perceived norms of roles also influence palliative caregiving capacity and ability to receive support. Whilst women are more likely to take on the caregiver role [52, 56], societal assumptions about gender and the feminized role of caregiving do not reflect the diversity of caregivers [51, 52, 56]. Dworzanowski-Venter [51] found paid male caregivers faced social stigma for performing work most often associated with women, in contrast the status of professional insulated male oncology nurses in her study from being ‘forgotten men’ within society. The studies revealed family palliative caregivers live with identity complexity with intersections of age, gender, ethnicity, family contexts, employment status and socio-economic status [52, 54, 56]. Furthermore, a person’s intersecting identities and social location led to wide variety of caregiving experiences and its consequences, including resilience, burden and burnout, economic and health inequity [52, 54, 56]. The family caregiver role led to financial burden for many. Giesbrecht and colleagues [52] identified that women family caregivers were often ineligible for government financial support, as they were often stay at home parents or working part-time. In contrast, Liu and colleagues [56] found black male caregivers are more likely to experience greater financial burden compared to white female caregivers.
A person’s living environment and socioeconomic status were shown to impact on access and provision of palliative care. Safe and secure homes situated in urban locations increase the ability to be able to access and receive palliative care [52,53,54, 57]. People with lower socio-economic status who in rural areas find it more difficult to access resources that are needed to provide care for someone at home, such as equipment, medication, formal respite and home care support [52,53,54]. Reduced resources and access to support often results in the cessation of palliative care community services [52, 57], leaving no option for care apart from the hospital environment [52].
Power and status were strong aspects across the studies in relation to access, utilisation and experience of palliative care. Marked power differences were identified across the studies between palliative clinicians and patients [53], between clinicians and caregivers [51] and between palliative care settings and patients [53]. The professional power and status that clinicians hold was a stark contrast to the experience of powerlessness for patients who had experienced discrimination related to their intersecting identities across their lifetime [53, 59]. People experiencing overlapping forms of oppression and associated powerlessness, often experience social pressure to conform to normative society constructs of ‘patients’ in healthcare settings [55]. This in turn negatively impacts on their confidence to ask questions, disclose and receive information and ultimately have end-of-life care needs and preferences met [53, 59].



Comments (0)