
記住我
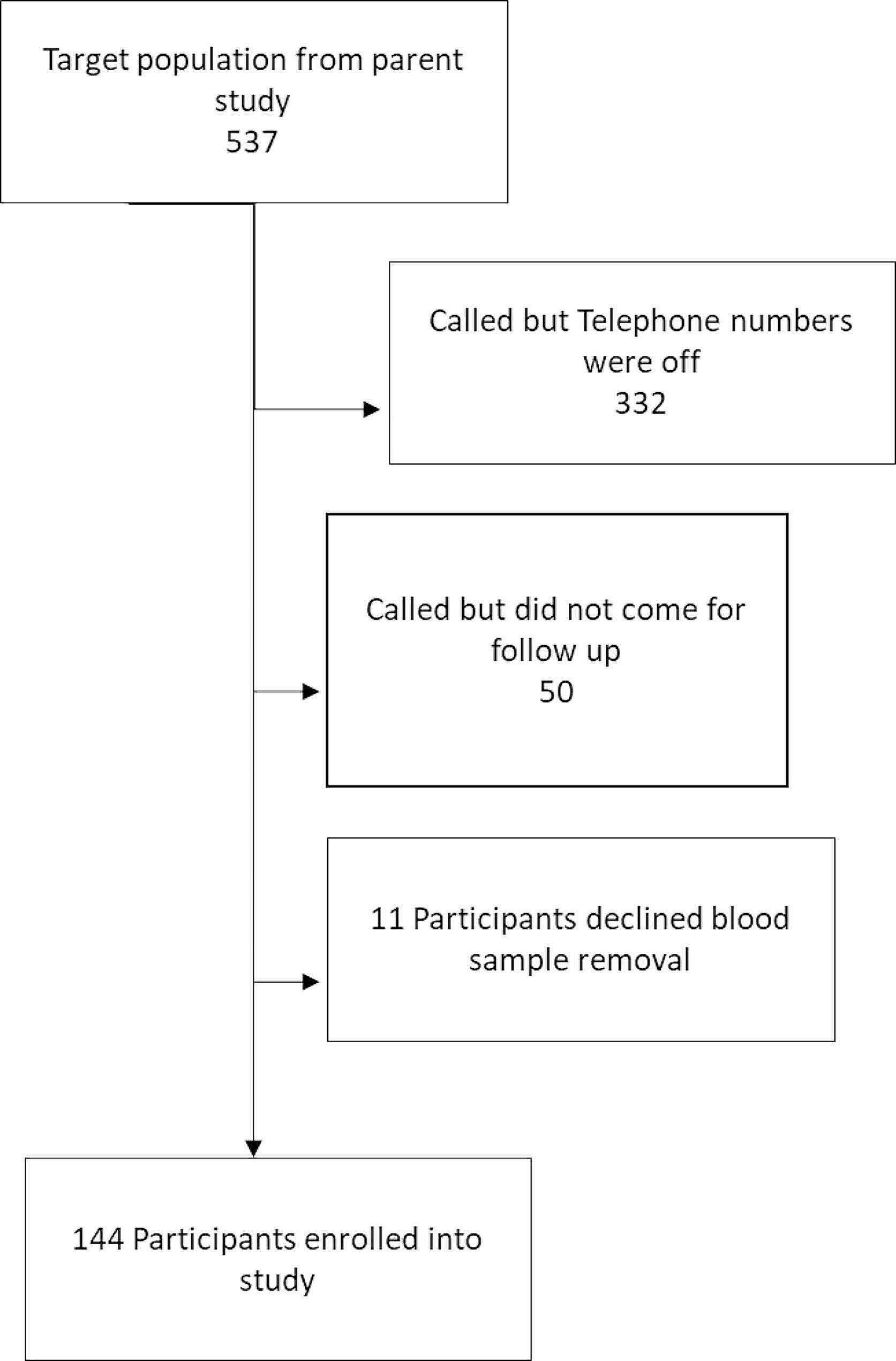





After excluding 149 participants with missing eGFR, the study population included 1795 participants (Fig. 1). Females made up 60% of the population, and the median age was 36 (Table 1).
Table 1 Total study population demographicsCKD prevalenceThe overall prevalence of CKD was 8.6% (Table 2). Males had a higher prevalence of CKD than females (12.5% vs. 6.1%). CKD was based on proteinuria alone in 30% of cases. Stage 3 CKD was most common (46% of CKD), while Stages 4 and 5 CKD were less common (16% and 8% respectively) with a much higher proportion of males in these higher stages. Of the 155 participants with CKD, 100 (65%, or 5.6% overall prevalence) had high-grade proteinuria or traditional CKD risk factors while 55 (35%, or 3.1% overall prevalence) were classified as suspected CKDu.
Table 2 Prevalence of CKD and CKD awarenessOnly 22% of participants with CKD reported a personal history of CKD (Table 2). Although awareness increased at higher stages of CKD, 4 participants with Stage 5 CKD and 18 with Stage 4 CKD did not report a history of CKD. Awareness was low among participants with both traditional CKD (25%) and suspected CKDu (16%).
Comparison of groups with no CKD, CKD from traditional causes, and suspected CKDuThe groups differed significantly in most demographic variables. We observed a higher proportion of males in both the traditional CKD group (52%) and the suspected CKDu group (67%) compared to the non-CKD group (40%) (Table 3). The CKD groups were older (median age 48 years for traditional CKD and 44 years in CKDu) than the non-CKD group (33 years) and higher proportions classified as extremely poor, or poor compared to the non-CKD group. Illiteracy rate was 20% in the CKDu group versus 13% in the traditional CKD group and 6% in the non-CKD group. A higher proportion of the suspected CKDu group lived in rural zones, and 38% obtained water from a well compared to 29% in the traditional CKD group and 19% in the non-CKD group. Reported daily water intake was highest in the suspected CKDu group, but soda intake, current alcohol use, and history of drug use did not differ between groups. NSAID and diuretic use was highest in the traditional CKD group. Exercise and eating fresh foods were rare overall.
Table 3 Comparison of demographics, health behaviors, medical history, and occupation by CKD category (no CKD, CKD with traditional risk factors, and suspected CKDu)Drinking well water was reported in 296 participants in the included groups. Almost half (47%) of participants using well water reported no treatment, and 48% reported using only chlorination treatment for their well water. Only 14 (5%) reported boiling, using a household filter, or other treatment to their drinking water. Type of water treatment did not differ significantly between the group with traditional CKD, CKDu, and no CKD (p = 0.85). Most of the wells (175, 75% of wells with data available) were hand-dug, while 25% were machine-drilled, and this did not differ by CKD category. There were 113 (39%) wells reported to be close to agricultural fields, which did not differ between groups (p = 0.92). The most common reported crops were peanuts (44), corn (21), sugar cane (19), sesame (15), and yuca (16). This did not differ between CKD categories except sugar cane, which was proportionally more common in the traditional CKD group than the others (p = 0.045).
The distribution of diabetes, hypertension, and kidney stones history largely reflects the study design (Table 3). Self-reported history of urinary tract infections (UTIs) was more common in the traditional CKD (65%) group than the suspected CKDu (50%) and the non-CKD groups (49%). Participants with a history of UTIs had a median of one infection in the past year, and a notable 41% of males reported a history of UTIs. Family history of CKD was highest in the traditional CKD group and almost equivalent in the suspected CKDu and non-CKD group.
The most common current occupation was homemaker for females (42% of females) and agricultural worker or student for males (18% and 17% of males, respectively). The suspected CKDu group had the highest proportions currently working in agriculture and with a lifetime history of working in agriculture compared to the other groups (Table 3). The suspected CKDu group also had the longest median time of working in agriculture (20 years). History of fainting or experiencing heat exhaustion at work did not differ between groups. Among 112 females with a history of working in agriculture, there were 3 with traditional CKD and 3 with suspected CKDu. Many females (66) performed tasks that included cutting crops or wood, with the largest number cutting cotton. Other tasks females performed commonly were seeding and weeding. Self-reported history of heat exhaustion was similar between male and female agricultural workers.
Median BMI was highest in the traditional CKD group (28) and lowest in the suspected CKDu group (24) (Table 4). Overall, there was a high prevalence of overweight, obese, or extremely obese individuals. The CKDu group had the highest uric acid levels in both males and females. When results were stratified by CKD stage, uric acid was still higher in the CKDu group, although the difference was no longer significant (Supplemental Figs. 1 and 2).
Table 4 Health assessment and measurements by CKD categoryFig. 2
Odds ratios and 95% confidence intervals for the multinomial logistic regression model for CKD with traditional risk factors and suspected CKDu. The reference group is participants with no CKD. Lower socioeconomic status represents a change in one classification per previously defined criteria. Well water source is compared to a public water system. Abbreviations: CKD: chronic kidney disease. CKDu: Chronic kidney disease of unknown etiology. UTI: urinary tract infection. BMI: body mass index
A higher proportion of participants in the suspected CKDu group had CKD Stages 4 and 5, with a median eGFR of 40 ml/min/1.73 m2 compared to 51 ml/min/1.73 m2 in the traditional CKD group (Table 4). Among 1137 with available data from dipstick urinalysis, almost half of participants in the traditional CKD group have proteinuria (48%) compared to only 16% in the CKDu group. Urinary leukocyte esterase was common (> 20%) in both CKD groups.
The final multinomial logistic regression model included the prioritized covariates (sex, age, socioeconomic status), plus BMI (as a continuous variable), water source (well or public water system), family history of CKD (yes or no), and history of UTI (yes or no) (Fig. 2). Variance inflation factors were all < 1.2, indicating no collinearity of covariates in the final model. Male sex was associated with increased odds of both traditional CKD (OR 2.38, CI 1.51–3.74) and suspected CKDu (OR 3.36, CI 1.80–6.26). A 10-year increase in age was associated with an increased odds of both traditional CKD (OR 2.25, CI 1.85–2.75) and suspected CKDu (OR 2.18, CI 1.71–2.77). Lower socioeconomic level was associated with higher odds of traditional CKD (OR 1.35, CI 1.04–1.76), but was not significantly associated with suspected CKDu (OR 1.29, CI 0.91–1.82). A family history of CKD was strongly associated with higher odds of traditional CKD (OR 2.04, CI 1.31–3.19) but was not significantly associated with suspected CKDu (OR 1.33, CI 0.71–2.51). Similarly, a history of UTIs were associated with traditional CKD (OR 1.83, CI 1.16–2.89) but not with suspected CKDu (OR 1.18, CI 0.65–2.13). Having a well as opposed to a public water system increased the odds of suspected CKDu (OR 2.26, CI 1.21–4.20) but was not significantly associated with traditional CKD (OR 1.62, CI 0.98–2.68). A five unit increase in BMI was associated with 0.4 lower odds of developing CKDu (OR 0.60; CI 0.43–0.82), while BMI was not significantly associated with traditional CKD (OR 0.96; CI 0.80–1.15).
The indeterminant CKD group (n = 351) was excluded from the above analysis, but we performed an analysis for both 1) the indeterminant group included as an outcome and 2) the indeterminant group included in the no CKD group (Tables S1, S2, S3 and S4). We developed a multinomial logistic regression model for both analyses, and found the odds ratios were similar for most variables, but the covariate of agricultural work history remained significant and was included in the final model when the indeterminant group was included as an outcome (Tables S5 and S6). History of agricultural work was protective for traditional CKD (OR 0.52 CI 0.29–0.92) when indeterminant CKD group is included as a separate group (Table S5).
留言 (0)