
Remember me





Based on the investigation of the literature in Iraqi population, the analyses have been separated into three main categories. The first analysis focuses the genetic variats that showed to have been significant in risk increase in T2DM. The second analysis focuses on the dempgraphic effect and its various groups and how each group could be interconnected. Finally, the third analysis uses the information from the studies and performs a sensitivity analysis based on their population sample size and their Odd-ratio.
Genomic analysisSeveral genes associated with T2DM and related complications have been identified in the Iraqi population. The patterns of their associations with T2DM were extensively studied in Iraqi community and listed in Table 1 and further illustrated in Fig. 2.
Table 1 Identified genes that have an impact on T2DM among the Iraqi populationFig. 2
Genes and their associated population size and control size
The Vitamin D receptor gene, VDR, displayed a significantly larger number of patients (1677) compared to controls (817), indicating a potential role in T2DM pathogenesis. Vitamin D's metabolic functions may contribute to this association. ADIPOQ, which encodes the adiponectin protein, showcased a notable difference in patient (1470) and control (735) counts. Adiponectin's regulatory role in glucose metabolism underscores its importance in T2DM risk.
The FTO gene, linked to obesity, displayed substantial patient (1600) and control (800) counts. Obesity's intricate relationship with T2DM suggests FTO's potential involvement in the disease's onset. CDKN2A/B: This gene pair, associated with cell cycle regulation, exhibited a significant difference in patient (800) and control (400) counts. Its role in pancreatic β-cell function and cell cycle control could contribute to T2DM susceptibility.
The analysis highlights genes with notable differences in patient and control counts, suggesting their potential involvement in T2DM risk within the Iraqi population. These findings align with existing knowledge of metabolic and regulatory processes implicated in T2DM development. In order to further elaborate on the effect the genes have, each gene is explained with their associated reference.
ACE (gene ID: 1636): This gene was also known as ACE1, CD143, DCP, and DCP1. ACE gene positioned in chromosome 17 and encodes for angiotensin I converting enzyme. This enzyme was involved in numerous metabolic pathways, including the control of neuronal plasticity, electrolyte balance, and blood pressure [13]. Some of the Iraqi population exhibit polymorphic ACE I/D, which was associated with T2DM; furthermore, the AGT M235T allele was absent in the same population (Iraqi population) [14]. According to Dhumad [15], the DD genotype and D allele of the ACE I/D polymorphism are risks factor for T2DM. Indeed, there was an association between the presence of the D allele of this polymorphism and the development of CAN in patients with T2DM [15].
ADIPOQ: One of the key adipocyte secretory proteins most often identified in human plasma is adiponectin, which plays important functions in regulating energy balance and glucose tolerance as well as insulin sensitivity in muscle and the liver. The ADIPOQ gene, which produces adiponectin, is found on human chromosome 3q27, where three exons that span 17 kb have been identified as a susceptibility locus for metabolic syndrome and T2DM. In a Chinese population, the ADIPOQ genetic polymorphisms were linked to T2DM [16]. The findings of the study conducted by Al-saadi (2016), indicates an association between T2DM and a G276T polymorphism in ADIPOQ, which codes for adiponectin [17]. This conclusion arose from an analysis of the genotype and allele distribution of ADIPOQ rs2241766 gene in T2DM patients [18]. In addition, Algenabi (2021), identified polymorphisms in the promoter region of rs17300539 as contributing to the initiation of T2DM. Metabolic changes in diabetic patients are attributed to this polymorphism [19].
Compared to controls, there was a greater distribution of T45G polymorphisms of in ADIPOQ in T2DM patients (mean ± standard error control: 0.160 ± 0.07, T2DM patients 0.515 ± 0.06) [20]. It is considered that in the Al-Najaf Governorate of Iraq, an adiponectin receptor 2 gene SNP is implicated in causing T2DM with Cardiovascular Disease (CVD). The risk of developing of T2DM with CVD is elevated in an individuals with the homozygous genotype (TT) and heterozygous (AT) genotype of rs1106197. Furthermore, there is an association between increased risk of develop T2DM with CVD with the frequency of T allele of rs11061971. Ismail (2016), state that R2 adiponectin receptors are implicated in metabolizing TG and VLDL cholesterol [21]. The polymorphism rs266729 of the adiponectin gene, which is also implicated in causing T2DM, might affect levels of HDL and insulin, thereby contributing to CVD and metabolic syndrome [22]. By influencing the concentration of serum lipids and promoting insulin resistance, the presence of the rs2241766T > G SNP of the adiponectin gene is a T2DM risk factor for Iraqi individuals [23].
AHSG: The liver releases fetuin-A also referred to as a-Heremans-Schmid glycoprotein, which binds to the insulin receptor tyrosine kinase in peripheral tissues and inhibits the insulin-induced intracellular signal cascade, leading to peripheral insulin resistance. Human linkage studies of traits including metabolic syndrome and T2DM have located the locus (3q27) where the gene encoding fetuin-A (AHSG) is located. In a recent study, we also discovered a link between plasma fetuin-A levels and the risk of T2DM in a sizable sample of older persons living in the community who took part in the Cardiovascular Health Study (CHS) and were monitored for a median of 11 years [24]. Ali (2019) found a significant difference in the GC and GG genotypes of healthy individuals and T2DM patients. For those with the GC phenotype, the risk of T2DM was double that of those individuals with the GG phenotype (respective OR: 2.27, χ2 8.11 vs 0.4, χ2 9.74 [25]
APOE: The gene's product is a significant apoprotein within chylomicrons. It binds to specific receptors in the liver and peripheral cells, playing a vital role in the regular breakdown of lipoprotein components rich in triglycerides. This gene is located on chromosome 19 alongside related apolipoprotein C1 and C2 genes. Mutations in this gene lead to conditions like familial dysbetalipoproteinemia or type III hyperlipoproteinemia (HLP III), characterized by elevated plasma cholesterol and triglycerides due to impaired elimination of remnants from chylomicrons and VLDL [26]. Genetic variations in the ApoE gene, particularly in SNPs rs429358 and rs7412, could potentially act as predisposing factors for T2DM and CVD in Iraqi patients [27].
CDKN2A/B: This gene produces many transcript variants, each of which has a unique first exon. Two of the at least three alternatively spliced variants found encode proteins with structurally similar isoforms that are known to act as CDK4 kinase inhibitors. CDKN2 gene is a recognized key tumor suppressor gene that is commonly altered or deleted in some tumor types [28]. Whilst the rs2383208 SNP did not impact the disease among the Iraqi population, there is evidence that the rs10811661 SNP affects insulin levels in T2DM patients [29].
CNDP1: This gene encodes a member of the M20 metalloprotease family. The protein produced by this gene has exclusive expression in the brain and takes the form of a homodimeric dipeptidase, identified as human carnosinase. A trinucleotide (CTG) repeat length polymorphism is present in the coding region of this gene [30]. The variation (rs2887) within the CNDP1 gene indirectly contributes to the emergence of CVD in individuals with T2DM in Iraq. This variation leads to elevated serum levels of carnosinease-1, subsequently enhancing the breakdown of carnosine, thus potentially influencing CVD development [31].
ELMO1: A novel and promising candidate gene called ELMO1 (Engulfment and Cell Motility 1), which is found on chromosome 7p14.2–14.1, is responsible for cell motility and the phagocytosis of apoptotic cells [32]. Mohammed (2019), report that individuals in Kerbala/Iraqi province with polymorphisms at the rs741301 region of the ELMO1 gene are vulnerable to the T2DM complication of DN [33].
FTO: It was first discovered as a gene involved in programmed cell death. Three investigations conducted in 2007 showed a connection between body mass and differences in FTO. There are many polymorphisms known. In comparison to those without a risk allele, the 16% of people who are homozygous for the risk allele SNP rs9939609 weigh roughly 3 kg heavier and have a 1.67-fold greater risk of obesity. This connection may be noticed in people aged 7 and older and implies a particular rise in fat mass [34]. Al-Tu’ma & Obed (2018), found a significant association between the FTO gene polymorphism, rs9939609, and levels of HDL cholesterol in obese, male Iraqi T2DM patients [35]; however, no association between this polymorphism and other biochemical parameters was detected. Younus (2017), report that rs9939609 and rs17817449 polymorphisms of the FTO gene contribute to insulin resistance, increasing the prevalence of T2DM in obese patients [36]. The work by Algenabi (2021), supports those earlier findings, noting that in obese patients, rs17817449 and rs1588413 polymorphisms are effective predictive markers of developing T2DM [37]. Thus, the risk of developing of T2DM might be elevated by variations in the G276T polymorphism in the adiponectin gene.
GST (M1, P1): Glutathione S-transferase (GST) family proteins are enzymes that detoxify a variety of dangerous chemicals, such as reactive oxygen species (ROS) or xenobionts [38]. According to the current findings, T2DM patients with the GSTT1 positive genotype are afforded some protection against the risk of CAD [39]. Mahmood (2015), determined the GSTM1 positive genotype to be a CVD risk factor for patients with T2DM [40]. We found the prevalence of the GSTP1 heterozygous mutant allele Ile/Val to be lower in controls than in patients with T2DM (30% vs 40%; P = 0.01). Furthermore, the homozygous mutant of GSTP1 allele Val/Val, was not identified in any of the controls, but was found in 3.33% of T2DM patients (P = 0.001). After the onset of T2DM, GSTP1 genotypes do not influence blood lipids. Agarose gel electrophoresis was used to determine genotypes, which produces bands in the gel [41].
IL-17: The encoded protein for the IL-17 gene, which belongs to the five-member IL-17 receptor family (IL-17RA-E), is a pro-inflammatory cytokine generated by activated T cells [42]. It is considered to be an important risk factor for the onset of T2DM. Furthermore, elevated HOMA-IR values correspond to hyperglycemia, so is another T2DM risk factor [43].
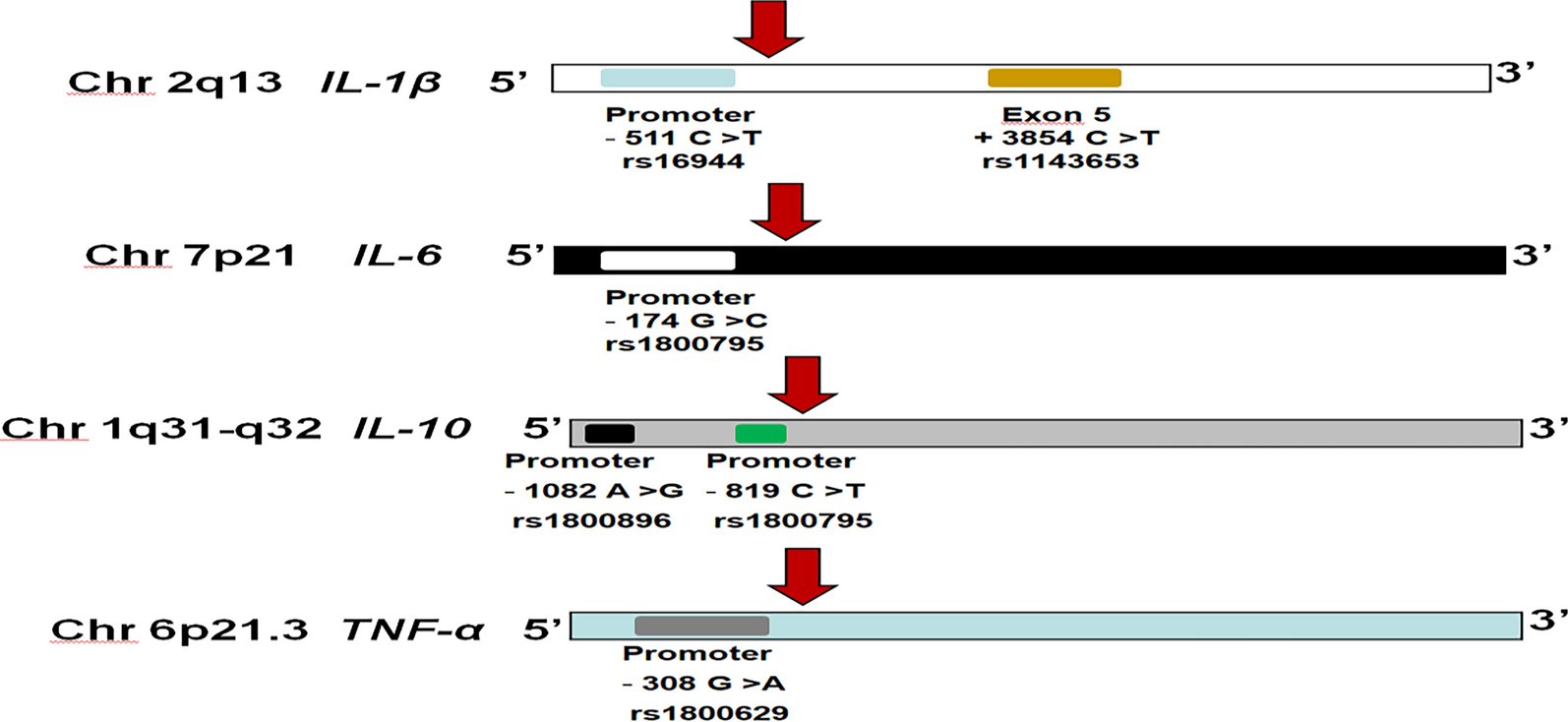
IL-10: Human IL-10 is produced by a gene on chromosome one (1q31-32). Additionally, three biallelic polymorphisms for IL-10 have been discovered at locations -1087, -824, and -597 from the transcription start site23 [44]. The IL-10 (-592A/C) gene polymorphism was identified by Hamid & Shani as being a contributor to developing T2DM [45].
IL-23: A member of the IL-12 family, IL-23 has two components, p40 and p19, and is generated by dendritic cells, monocytes, and macrophages. Th17 effector cells can grow and remain active as a result of IL-23 attaching to its heterodimeric receptor. The receptor may be seen on the surface of macrophages, monocytes, dendritic cells, and lymphocytes. While the p19 subunit of IL-23 has a distinct and strong affinity for IL-23R, the p40 subunit of IL-23 is shared with IL-12. IL-23R is involved in the initiation and maintenance of IL-23/IL-17 signal transduction; changes to the signaling pathway may result in the deregulation of the inflammatory response [46]. Al-Badri (2022), determine that GT and TT of SNP (rs1884444G/T) promoted the risk of T2DM and oral fungal infection [47].
IL-4, IL-6: IL-4 gene produces a pleiotropic cytokine by T cells that have been stimulated. The interleukin 4 receptor is a ligand for this cytokine. The interleukin 4 receptor binds to IL13 as well, which may help explain why these two cytokines have many similar roles [48]. IL-6 gene produces a cytokine that aids in B cell development and inflammation. Additionally, it has been demonstrated that the encoded protein functions as an endogenous pyrogen that can cause fever in persons with autoimmune disorders or infections. The interleukin 6 receptor alpha is the place where the protein is largely generated, where it is released into the serum and triggers a transcriptional inflammatory response. Numerous inflammation-related disease conditions, such as susceptibility to diabetes mellitus and systemic juvenile rheumatoid arthritis, are linked to the activity of this gene. Infections with viruses, such as COVID-19 [49]. According to the works by Shehab and Khdaer there is an association between heterozygous GC genotypes and T2DM. Also, a robust relationship was identified between the levels of IL-6 and T2DM and IR groups. Specifically, the incidence of T2DM and IR are elevated with the CC variation of IL-6 (-174) 9 [50, 51].
KCNJ11: The potassium channel gene KCNJ11, which belongs to that family, is found at 11p15.1 and lacks an intron. An inward-rectifier potassium ion channel is encoded by this gene (Kir6.2). The KATP channel is made up of the Kir6.2 proteins and the high-affinity sulfonylurea receptor 1 (SUR1). The ABCC8 gene, which is adjacent to the KCNJ11 gene, encodes SUR1. The Kir6.2 proteins is a 390 amino acid protein having intracellular N- and C-terminals and two transmembrane domains (M1 and M2). The KATP channel in the plasma membrane of pancreatic beta cells is structurally made up of four high-affinity SUR1 subunits that envelope the pore, which is formed by Kir6.2 tetramers. Via glucose metabolism, that channel regulates insulin secretion and synthesis [52]. Although an association has been determined between the E23K; rs5219 SNP and T2DM, more research is need to establish the strength of that association [53].
KCNQ1: The slow delayed rectifier current (IKs) that occurs after the repolarization of the cardiac action potential is caused by the KCNQ1 gene, which encodes the α-subunit of the voltage-gated potassium channel Kv7.1. Pathogenic missense variations frequently show a dominant-negative impact that can be attributed to interference with the wild-type (WT) subunits translated from the non-affected allele because the KCNQ1-encoded -subunits tetramerize during Kv7.1 channel construction [54]. From a sample of the Iraqi population, Al Hussieny determined that rs2237892, and rsl51290 polymorphisms of this gene are T2DM risk factors [55].
LEP: This gene produces a protein that is released into the bloodstream by white adipocytes and is crucial for maintaining the balance of energy. The brain's leptin receptor binds to circulatory leptin, activating the signaling pathways that prevent overeating and encourage energy expenditure. This protein also was associated with the control of immunological and inflammatory responses, hematopoiesis, angiogenesis, reproduction, osteogenesis, and wound healing. It plays several endocrine roles [56]. Consistent with the findings of Musafer (2022), our study found a robust association between rs11761556 and rs12706832 SNPs and T2DM. These SNPs could be used as biomarkers for the early detection of T2DM [57].
LEPR: This gene produces a protein that belongs to a member of the gp130 family of cytokine receptors, which are reported to activate cytosolic STAT proteins to promote gene transcription. This protein is a leptin receptor that regulates fat metabolism and participates in a brand-new hematological pathway necessary for healthy lymphopoiesis. Obesity and pituitary dysfunction have been linked to mutations in this gene [58]. According to Ahmed & Ghali (2017), susceptibility to T2DM is indicated by the presence of the rs1137101 (Q223R) polymorphism in the LEPR gene. This could also be exploited as a biomarker for T2DM [59].
LEP 2548 G/A: Unclear evidence links LEP/LEPR to overweight/obesity and the associated metabolic abnormalities. These outcomes can be the result of unknown gene-environment interactions. But in Iraqis Individuals in Erbil who have elevated serum concentrations of leptin and carrying the A allele carrier may be at greater risk of developing T2DM [60, 61].
MCP-1: On chromosome 17's q-arm, several cytokine genes are grouped, including MCP-1. A subfamily of secreted proteins known as chemokines has a role in both inflammatory and immunoregulatory processes. Based on the configuration of the mature peptide's N-terminal cysteine residues, the superfamily is subdivided into four subfamilies. The CC subfamily, which includes this chemokine, is distinguished by two adjacent cysteine residues. For monocytes and basophils, but not for neutrophils or eosinophils, this cytokine has chemotactic action. It has been linked to the pathophysiology of illnesses including psoriasis, rheumatoid arthritis, and atherosclerosis which are characterized by monocytic infiltrates. It binds to the CCR2 and CCR4 chemokine receptors. The coronavirus 2 infection that causes severe acute respiratory syndrome is linked with increased expression of the encoded protein [62]. A significant relationship was determined between the rs1024611 polymorphism and greater DFU susceptibility in Iraqi T2DM patients. Compared to T2DM patient without DFU, the frequency of AG and GG genotypes was higher in those with DFU [63].
MIR-196A2: MicroRNAs (miRNAs) are small (20–24 nt) non-coding RNAs that influence the stability and translation of mRNAs to regulate gene expression in multicellular animals post-transcriptionally [64]. Jameel (2019), study identified the association between the miR-196a2 polymorphism and T2DM [65].
PD-1: negatively controls the immunological response. acts before or inside of the negative regulation of apoptosis, the negative rule of tolerance induction, and the positive regulation of apoptosis. it is situated on the plasma membrane's outer side. is seen in the retina. used to research systemic lupus erythematosus and dilated cardiomyopathy. This gene's human ortholog (s) has been linked to lupus nephritis, hepatitis B, hepatitis C, and various autoimmune diseases [66]. The data from Rasheed (2020), point to the A allele of PD-1–538 G/A being a possible risk factor for developing T2DM. Compared to other genotypes of this polymorphism, the GG variant is linked to elevated serum levels of sPD-1 [67].
PPARG: A nuclear receptor belonging to the peroxisome proliferator-activated receptor (PPAR) subfamily is encoded by this gene. PPAR-alpha, PPAR-delta, and PPAR-gamma are the three subtypes of PPARs that are recognized. This gene produces the PPAR-gamma protein, which controls the development of adipocytes. PPAR-gamma has also been connected to the pathophysiology of several illnesses, including cancer, DM, atherosclerosis, and obesity [68].
The results showed that the distribution of genotypes and alleles frequencies at (rs1801282) SNP of PPARG gene, as related with CC, CG, and combined CG + CC genotypes, G allele seems to be a protective allele, therefore, the presence of both heterozygous and homozygous mutants may reduce the risk of T2DM (the frequency of CG + GC mutants were 68% in apparently healthy control individuals and 50% in T2DM patients). In contrast, there is a wild CC genotype (50 versus 32% in T2DM and control group, respectively, X2 = 6.93; P < 0.01; OR = 1.272) [69].
SOST: Sclerostin is a secreted glycoprotein that shares sequence similarities with the DAN (differential screening-selected gene aberrative in neuroblastoma) family of bone morphogenetic protein (BMP) antagonists and has a C-terminal cysteine knot-like (CTCK) domain. This gene’s loss-of-function mutation is linked to the autosomal-recessive condition sclerosteosis, which results in progressive bone overgrowth [70]. Ali (2021), state the risk of CAD is high in T2DM patients who have the T allele and increased plasma concentrations of sclerostin [71].
TNF: A multifunctional proinflammatory cytokine from the tumor necrosis factor (TNF) class is encoded by this gene. Mostly macrophages secrete it. It can bind to and work through the TNFRSF1A/TNFR1 and TNFRSF1B/TNFBR receptors. Numerous biological processes, including cell division, proliferation, apoptosis, lipid metabolism, and coagulation, are regulated by this cytokine. TNF has been connected to several illnesses, including cancer, autoimmune disorders, insulin resistance, psoriasis, rheumatoid arthritis, ankylosing spondylitis, and TB [72].
Al-Hilali (2015), found insulin resistance in T2DM patients to be significantly greater than controls. The researchers noted a correlation between insulin resistance and the AA genotype with an A allele polymorphism. Whilst our work, supports the earlier findings of the A allele being associated with susceptibility to T2DM, we found the G allele to confer protection against the disease [73]. Mousa (2018), suggests that the A allele of the TNF-α gene could contribute to the prevalence and susceptibility Al-Muthanna and Baghdad province’s population to T2DM [74, 75].
TGF-β1: (transforming growth factor-beta) superfamily of proteins' secreted ligand is encoded by this gene. This class of ligands binds different TGF-β receptors, causing the recruitment and activation of transcription factors from the SMAD family that control gene expression. The encoded preproprotein is either found in a latent form made up of a mature peptide homodimer, a LAP homodimer, and a latent TGF-β binding protein, or it is found in an active form made up primarily of the mature peptide homodimer. The mature peptide can combine with other TGF-β family members to create heterodimers. The production and activation of other growth factors, including interferon-gamma and tumor necrosis factor, can be modulated by this encoded protein, which also controls cell proliferation, differentiation, and growth [76]. The C allele of TGF-β1 gene in codon 25: + 915*G/C was linked to greater risk of T2DM polymorphism, while the G allele appears to offer protection against the disease. However, Hussein found the risk of T2DM was increased in GG and CC genotypes; this risk was not observed in the GC genotype [77]. The study by Nuhiar suggests TGFβ1 gene polymorphisms to be implicated in the incidence of T2DM in the population of Thi-Qar [79].
TCF7L2: encodes a transcription factor with a high mobility group (HMG) box that is essential for the Wnt signaling pathway. The protein has been linked to the regulation of blood sugar levels. An increased risk of T2D is linked to genetic variations of this gene. For this gene, many transcript variants have been discovered that encode various isoforms [79]. Genotyping of 212 participants was conducted using a cost- and time-effective, high-throughput tetra-primer amplification refractory mutation system-polymerase chain reaction (Tetra ARMS-PCR) assay. The results indicate an association between TCF7L2 rs7903146 polymorphisms and the risk of T2DM. Among Kurdish Iraqi people, the T allele appears to promote the individual’s susceptibility of developing T2DM [80]. None of the controls in Omran study expressed the TT genotype of rs12255372(G/T), which was determined to be an important risk factor for developing T2DM [81]. According to Hassan (2018), the rs12255372 (G/T) polymorphism makes the Al Najaf population vulnerable to T2DM [82]. Data from Mohammed (2021), point to a robust relationship between rs7908486 and obesity; this gene could be used as an effective early detection biomarker of obesity [83]. Ahmed (2019), claim that TCF7L2 gene genetic polymorphisms were influential in females in Iraq developing T2DM. In contrast, data obtained by Abdullah, failed to find a role for TCF7L2 gene polymorphism rs4506565 T/A, with no significant differences being detected in any of the codominant, dominant, over dominant, recessive, and additive models. Of the parameters considered by the dominant model, only age shows a significant difference [84, 85].
VCAM-1: It is a member of the Ig superfamily that produces a cell surface sialoglycoprotein when the endothelium is stimulated by cytokines. This type I membrane protein may contribute to the development of rheumatoid arthritis and atherosclerosis by mediating leukocyte-endothelial cell adhesion and signal transmission [86]. The findings of Salman (2017), Study indicate that A/G genotype was more prevalent in the control group than the patient group. Furthermore, he found that compared to the A allele, the G allele of the VCAM-1 (rs3783605 A: G) SNP made a greater contribution to causing T2DM [88]; thus, among the population of Iraq, it could be as a potent risk factor for T2DM.
PON1: Discovered for its detoxifying potential, serum paraoxonase (PON1) is presumed to counteract organophosphorus compound toxicity. The lower activity of PON1 is thought to increase suscepti
Comments (0)