Acute myeloid leukemia (AML) is a clonal hematopoietic stem cell malignancy characterized by accumulation of immature progenitor cells with arrested differentiation leading to suppression of hematopoiesis. AML is heterogeneous with respect to morphology, immunophenotype, (cyto) genetic and epigenetic signatures and responses to treatment, including patient outcomes [9].
DNMT3a encodes a DNA methyltransferase that regulates the epigenetic modification of gene expression by catalyzing the addition of a methyl group to the cytosine residue of cytosine guanine dinucleotides. DNMT3a mediates DNA methylation involved in the differentiation of hematopoietic stem cells into a predominantly granulocytic lineage. DNMT3a mutations are relatively common in myeloid neoplasia and are detected in 20% of AML patients [10].
DNMT3a mutation is the commonest aberration in clonal hematopoiesis of indetermined potential (CHIP), a pre-leukemic state associated with a very increased risk of developing myeloid neoplasm, including AML. The broad clinical context in which DNMT3a mutation occurs has made it difficult to study the prognostic effect of DNMT3a mutations in AML specifically; moreover, numerous studies have revealed varied clinical correlations among DNTM3A-mutated AML patients associated with specific variant type (e.g., R882 vs. non-R882) [11].
We aimed to study DNMT3a mutations in 20 Egyptian AML patients free from either solid or hematological malignancies and to elucidate its prognostic influence on AML disease course. Our patients were recruited from hematology units of Internal Medicine department, Ain shams University Hospitals during the period from July 2022 to April 2023.
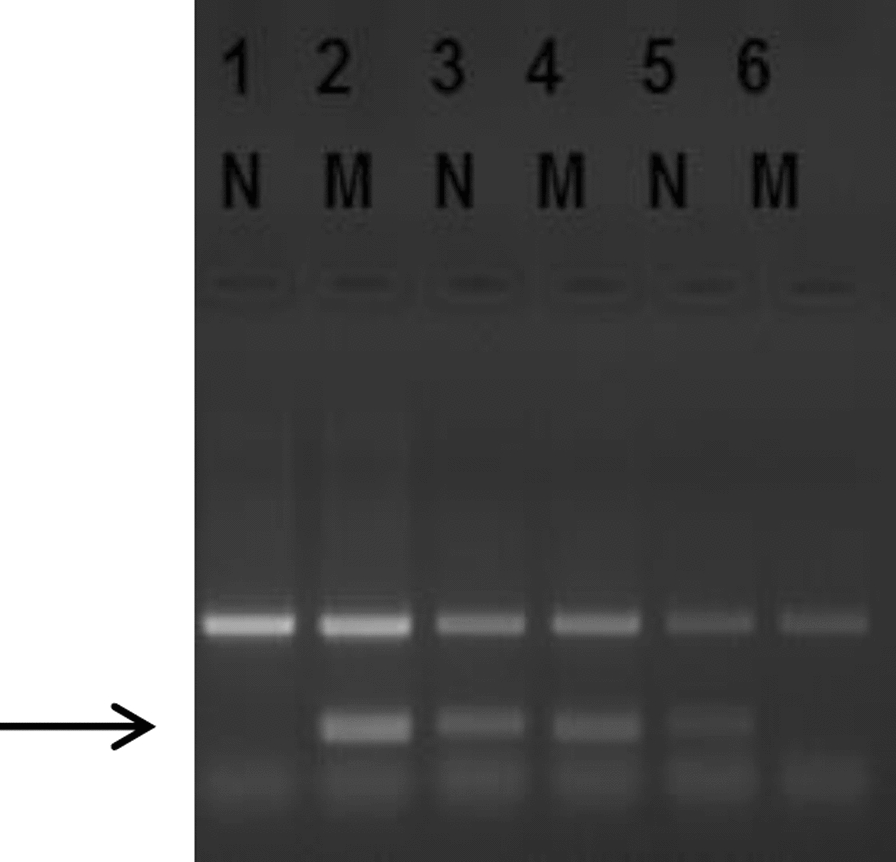
Diagnosis was based on updated WHO 2016 diagnostic criteria and its 5th edition paper. Our AML patients were then followed up to evaluate their response to induction after 28 days of chemotherapy and after 3 months both morphologically and via MRD quantification by multiparameter flow cytometry. DNMT3a hot spot exon 23 mutation was characterized using Sanger Sequencing technique.
Our results revealed that overall DNMT3a mutations were present in 25% of our patient consistent with Park et al. [6] findings who detected DNMT3a mutations in approximately 20% of AML cases. While it was present in 20% among cytogenetically normal AML in our study, Park et al. [6] found that it increased to 29.5% when analysis was restricted to CN-AML which might be due to bigger sample size of his study (n = 142).
In addition, Ley et al. detected DNMT3a mutations in approximately 20% of AML cases [12]. Interestingly, Loghavi et al. found DNMT3a mutations in up to 48% of their studied population which may be due to the variety in the ethnic group of her study which included Hispanics, African and Asian individuals [13].
In our study R882 mutation was positive in 10% of cases which is almost similar to Yuan et al. where 8.51% carried the DNMT3a R882 mutation [14] and Blau et al. where they found DNMT3a R882 in 11% of their subjects [2]. Fifty percent of the R882 group were R882C mutated and 50% R882H mutated, where Yuan et al. found that 72% of R882 mutated cases were positive for the R882H mutation, 25% with the R882C mutation, and 3% cases with the R882P where [14]. Ethnicity mostly played an important role in that difference where Yuan studied Chinese population.
Regarding Gender and age, our results showed no significant difference in the distribution of gender within the groups. Similarly, age analysis indicated no significant variance (p = 0.461) among the group. In contrast, Loghavi et al. found that patients with DNMT3a mutation were significantly younger (median 56.0 vs. 62.0 years; p = 0.025) and mostly were women (65.7% vs. 46.9%; p = 0.045), similar to what was also found by El-Rhman et al. whose patients were significantly younger (p = 0.005) [13, 15]. Our smaller sampling size might have played role in this, where Loghavi et al. and Rhman et al. bigger sample sizes might have marked that difference (n = 178 and 100, respectively) [13, 15]
Similar to El-Rahman et al., our study showed no significant difference with respect to liver and spleen enlargement [15].
In our study, platelet count (PLT) demonstrated a significant difference (p = 0.024), with R882 mutation showing higher levels which may give a link between R882 mutation and higher platelet count, which is similar to what Veninga et al. found and attributed it to methylation error of the mutation affecting megakaryopoiesis [16]. Mean hemoglobin levels (Hb), total leukocyte count (TLC) and peripheral blast percentage exhibited no significant variance. In this aspect, Hou et al. had higher WBC, blast, and platelet counts than DNMT3a-wild patients (P value 0.0018, 0.0012, and 0.0001, respectively) where Chen et al. showed only highly significant difference in TLC (< 0.0001) with no significance Hb, PLT and peripheral blast percentage. El-Rhman et al. showed only significance in TLC and peripheral blast count (0.03 and 0.02, respectively) [15, 17, 18].
Immunophenotyping analysis among the three mutation groups revealed that most markers, including CD19, CD36, CD7, CD56, CD33, CD13, CD14, CD117, CD64, CD34, and HLA-DR, exhibited no significant differences among the mutation groups. Obviously, Myeloperoxidase positivity was significant among the groups (0.05), which may be due to small sample size. However, it is similar to Kamijo et al. who found that DNMT3A mutation was more likely to be present in the MPO-low group (p = 0.001) [19].
Cytogenetic analysis revealed positivity in 35% of all our AML cases with t(15:17) and inv(16) each representing 10% of the cases, t(8;21) representing 15% of cases and rest of cases are negative cytoFISH analysis. As regards DNMT3a mutated cases, only one case of the mutated DNMT3a had positive inv(16) by FISH, where the rest were FISH negative. To our knowledge, AML with inv(16), and inv(3)/t(3;3) rarely harbored the DNMT3a mutation, and this is the first reported case of DNMT3a mutation in AML with inv(16). This is similar to Park et al. who stated that DNMT3a mutations were more frequently identified in patients with cytogenetically normal (CN)-AML (p = 0.0112). In addition, Laghavi et al. notably found that none of their patients had recurrent AML-associated cytogenetic abnormalities. Similarly El-Rhamn et al. concluded that DNMT3a occurred exclusively in CN-AML. Yet, cytogenetics FISH revealed no significant difference among our study groups (0.536%) [6, 13, 15]
As for response to induction therapy, the mean bone marrow (BM) blast percentage was significantly different among the groups (p < 0.001), with R882 Mutation group exhibiting a notably higher mean (6.0%) compared to DNMT3a wild (1.3%) and non-R882 mutation (2.3%) implementing resistance to standard chemotherapy. This was reflected on treatment response, where the distribution of patients achieving partial remission (PR) was significantly different (p = 0.038), with 100% in R882 Mutation group achieving PR; while, Groups DNMT3a wild and non-R882 mutation showed lower PR rates. Minimal residual disease (MRD) blast percentage did not show a significant difference among our groups. This is coinciding with Yuan et al. where the pointed that DNMT3a R882 mutations might enhance chemoresistance to induction regimens including anthracyclines. Compared to patients without R882 mutations, those DNMT3a R882 mutations positive patients showed a significantly lower CR rate after the first cycle of induction therapy (28.77% vs. 42.48%, p = 0.023). This could be explained by Park et al. who stated that pre-leukemic hematopoietic clones with DNMT3a mutations may be resistant to leukemic therapy and may lead to further clonal expansion during remission, and may eventually cause recurrent disease [6, 14].
After 28 days of follow-up post-induction, 75% of all our patients achieved complete response (CR), 20% achieved partial response (PR) out of which 75% are DNMT3a mutated, and 5% of all patients succumbed to treatment-related mortality which was DNMT3a wild type.
After a 3-month follow-up, 50% of all our patients maintained CR, 40% exhibited PR where half of them were DNMT3a mutated patients and 10% faced mortality where half of them was R882 mutated which represents 20% of all DNMT3a mutated patients. The follow-up after 3 months indicated a significant difference in PR rates among our groups (p = 0.034), with R882 Mutation group having higher relapse rates. In addition, Kaplan Meier survival analysis showed poor survival rate for R882 mutated group. Coinciding with our results, Park et al. concluded that DNMT3a mutated AML showed poor OS and event-free survival (EFS), compared to that from the DNMT3a wild-type AML (p = 0.0484 and p = 0.0012, respectively) and they analyzed the prognostic effect of DNMT3a mutations in CN-AML and found that the DNMT3a-mutated CN-AML showed poorer OS and EFS compared to that shown by the DNMT3a wild-type CN-AML (p = 0.0376 and p = 0.0019). Similarly, Loghavi et al. concluded that in their study group, patients with DNMT3a mutations had worse outcomes than those with wild-type DNMT3a. El-Rhaman et al. suggested in their study that DNMT3a mutations were accompanied by worse outcome including significantly shorter OS and EFS and are an independent factor of worse outcome in younger patients with cytogenetic normal AML (CN-AML) [6, 13, 15].
However, Yuan et al. indicated that in spite of the association between DNMT3a R882 mutations and worse outcome, it is obscure whether the mutations are associated with response to anti-leukemic therapies, and whether DNMT3a mutant types at amino acid 882 or allele burden influence prognosis of AML which had been rooted to dependency on DNMT3A R882 mutant-allele ratio [14].




Comments (0)