
記住我
This pilot study used a non-blinded randomized control trial design with two parallel groups comparing a community-based multidisciplinary group intervention to usual care for individuals diagnosed with FM. A pilot was deemed an appropriate approach given the multi-component nature of the intervention, and that it included modifications made to our original intervention following a feasibility trial [16]. Participants were randomized into either the intervention group or control group using block randomization with a block size of four using Random Allocation Software [19]. Data collection took place over two years, between September 2017 and June 2019. The study protocol was a registered clinical trial (NCT03270449), received institutional ethics board approval on September 15 2017 (H17-01782-A010), and informed consent was obtained from all participants at enrollment.
Recruitment and participantsThe feasibility study [16] demonstrated a large effect size (r = 0.63) on the primary outcome (i.e., Patient Assessment of Chronic Illness Care (PACIC) survey) [20]. Based on this effect size, a power analysis using G*power software indicated that a sample of 60 participants, with 30 participants per group, would be sufficient to achieve 80% power with an alpha of 0.05 [21].
Participants were recruited through local general practitioner and rheumatologists’ offices, as well as through poster advertisements at medical clinics, a local hospital, local FM Facebook group, and other public online and community venues. Study inclusion criteria were: (1) formal diagnosis of FM by a physician based on their clinical assessment (and further confirmed by the study team rheumatologist); (2) resident of the small urban centre (population approximately 35,000) in British Columbia, Canada or surrounding area; (3) at least 19 years of age; (4) fluent in English or able to provide a translator; and (5) capacity to provide informed consent. The study exclusion criteria were: (1) individuals with a severe and/or chronic medical or psychiatric condition that could interfere with their ability to participate in the intervention; (2) women who were pregnant or lactating; (3) patients that did not provide permission to contact their primary health care provider; and (4) individuals who had previously participated in the feasibility study.
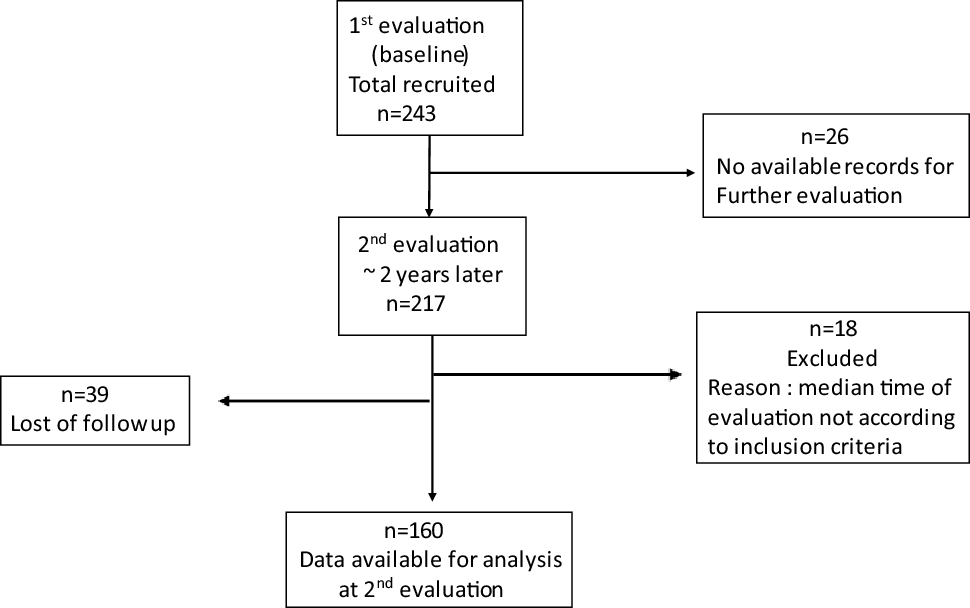
Of the 107 prospective participants screened for eligibility by the study coordinator, 60 were enrolled and randomized to either the intervention (n = 30) or control group (n = 30). Prospective participants who were not randomized (n = 47) either did not meet the inclusion criteria, were not available during the intervention hours, were waiting for formal FM diagnoses, declined to participate, or could not be contacted prior to the intervention start date. See Fig. 1 for a CONSORT flow diagram.
Fig. 1
Participant flow through the study
Intervention groupThe treatment was a community-based multidisciplinary group intervention which took place in a small urban centre in British Columbia, Canada. The intervention tested in the current study is a modified version of the original community-based intervention that was tested in an initial feasibility study [16]. As part of this feasibility study, qualitative feedback about the intervention was obtained from 11 patients and 6 health care providers; overall, feedback was positive and participants reported it was a helpful and valuable intervention. Based on participant feedback, several changes were made to the intervention (e.g., participants and health care providers both suggested adding a mental health counsellor component and as such four sessions on cognitive-behavioral therapy strategies for improving mental health were added to the intervention).
The intervention groups were made up of ten individuals per cohort for a total of three cohorts. Each cohort participated in a 10-week intervention which included once-weekly education sessions at a local community centre and twice-weekly exercise sessions at a private gym adjacent to the community centre. All participants were offered a referral for a consultation at a local sleep clinic.
During the first exercise session, participants underwent a one-on-one baseline assessment by a certified exercise physiologist or physiotherapist and were given an individualized exercise program to follow during the twice-weekly exercise sessions. Exercise sessions lasted for one hour and consisted of a personally tailored combination of aerobic, strength, and flexibility exercises. Participants were guided to adapt the intensity of the exercises based on their ability, which required attention to their own breath and body tension during the exercises. Individuals exercised in the same room as other members of their cohort.
The education component was developed based on evidence-based practice guidelines for FM and chronic pain self-management [10] and tested in a feasibility trial [16]. The 1-hour sessions took place weekly, immediately following one of the exercise sessions. Education included: four sessions focused on cognitive-behavioural strategies for improving mental health (facilitated by a doctoral student in clinical psychology and an occupational therapist, supervised by a registered psychologist), two sessions focused on reconceptualizing pain to improve exercise as well as integrating pain self-care techniques with therapeutic exercise and movement (facilitated by a physiotherapy pain specialist), two nutrition sessions (facilitated by a dietitian), and two peer support sessions (facilitated by a social worker). The total number of hours for the intervention was approximately 32.
Over the course of each 10-week intervention, a monthly healthcare provider “team huddle” teleconference sessions were conducted. These sessions provided a venue to ensure the integration of care and the opportunity to discuss issues or concerns regarding adverse events, patient care, and patient progress.
Control groupThe control groups were made up of ten individuals per cohort for a total of three cohorts running simultaneously with each intervention group. Participants randomized to the control group received usual care. In the catchment area for the current study, usual care for fibromyalgia involves a referral to a rheumatololgist. Therefore, patients assigned to the control group were referred to a local rheumatologist for a single, one hour, one-on-one consultation. During this appointment, the patient’s history was taken, a physical exam was performed, basic education about fibromyalgia was provided, and online resources for self-directed self-management were provided. At the conclusion of the study (i.e., three-month follow-up questionnaires were collected from all participants), the control group participants were offered the multidisciplinary group intervention.
Measures overviewSample characteristics including demographics (e.g., age, race/ethnicity, marital status) and clinical variables (e.g., time since diagnosis, comorbid conditions) were assessed during study enrollment. The primary and secondary outcomes were assessed prior to the intervention, immediately following the intervention, and at a three-month follow-up. The primary outcome was perceptions of quality of care and secondary outcomes were disease-related functioning, anxious and depressive symptoms, pain beliefs, and health service utilization. Consistent with guidelines secondary outcome measures were included as they lent evidence for the primary outcome [22].
Primary outcome measureThe primary outcome, patient-perceived quality of care, was assessed by the 20-item Patient Assessment of Chronic Illness Care (PACIC) survey [20]. The measure has the following five subscales: patient activation and involvement, delivery system design and decision support, goal setting and tailoring, problem-solving and contextual counseling and follow-up care and coordination. The PACIC has demonstrated adequate reliability as well as face, construct, and concurrent validity [20]. In the current research, Cronbach’s alpha ranged from 0.95 to 0.97 across timepoints.
Secondary outcome measuresThe Fibromyalgia Impact Questionnaire (FIQ) is a 20-item patient report measure which evaluates different domains of FM [23]. Seven items measure patients’ ability to do work, pain, fatigue, rest, stiffness, anxiety, and depression. Two additional items measure the extent to which patients felt good and missed work. The FIQ has demonstrated reliability and responsiveness to change in clinical studies [23]. In the current research Cronbach’s alpha ranged from 0.85 to 0.88 across timepoints.
The Hospital Anxiety and Depression Scale (HADS) is a 14-item self-report measure of psychological distress which can be divided into two subscales reflecting depressive and anxious symptoms [24]. Psychometric properties of the HADS are adequate in primary care patients and the general population [25]. In the current research Cronbach’s alpha ranged from 0.88 to 0.93 across timepoints.
The brief version of the Survey of Pain Attitudes (SOPA-B) is 30-item patient report measure which assesses attitudes and beliefs about pain with adequate psychometric properties [26]. The SOPA-B assesses seven domains including pain control, disability, medical cure, solicitude, medication, emotion, and harm. In the current research, Cronbach’s alpha ranged from 0.70 to 0.79 across timepoints.
Health care utilization data was collected from the local health authority. Specifically, the number of emergency department visits participants made six months prior to the intervention, during the intervention, and for three months following the intervention were obtained. The ED data included all reasons for visiting the ED, whether FM-related or not.
Statistical analysisAs a randomization check, demographic and clinical variables (e.g., age, gender, ethnicity, years since FM diagnosis) were compared between participants assigned to the control and intervention conditions using t-tests for continuous variables and Pearson’s chi-square or Fisher’s exact tests for categorical variables. Descriptive analyses were conducted on the demographic and clinical variables, as well as the primary and secondary outcome variables at each of the three timepoints. Patterns of missing data were analyzed using Little’s MCAR test. Following recently published guidelines no data was imputed and complete case analysis was conducted [27].
Regarding the main analyses, mixed model analyses using maximum likelihood estimation were used to assess group by time interactions. Independent sample t-tests were used to compare the intervention versus control group difference scores (baseline to post-intervention and baseline to three-month follow-up). The criteria for statistical significance was p < 0.05. Effect sizes were calculated, and can be interpreted as small (Cohen’s d ≥ 0.20), medium (Cohen’s d ≥ 0.50), and large (Cohen’s d ≥ 0.80) [28]. The preliminary descriptive and bivariate analyses were conducted using SPSS Version 27 (Armonk, NY: IBM Corp), and the main analyses were conducted using R Version 3.6.3 (Vienna, Austria: R Foundation for Statistical Computing).
留言 (0)