
記住我
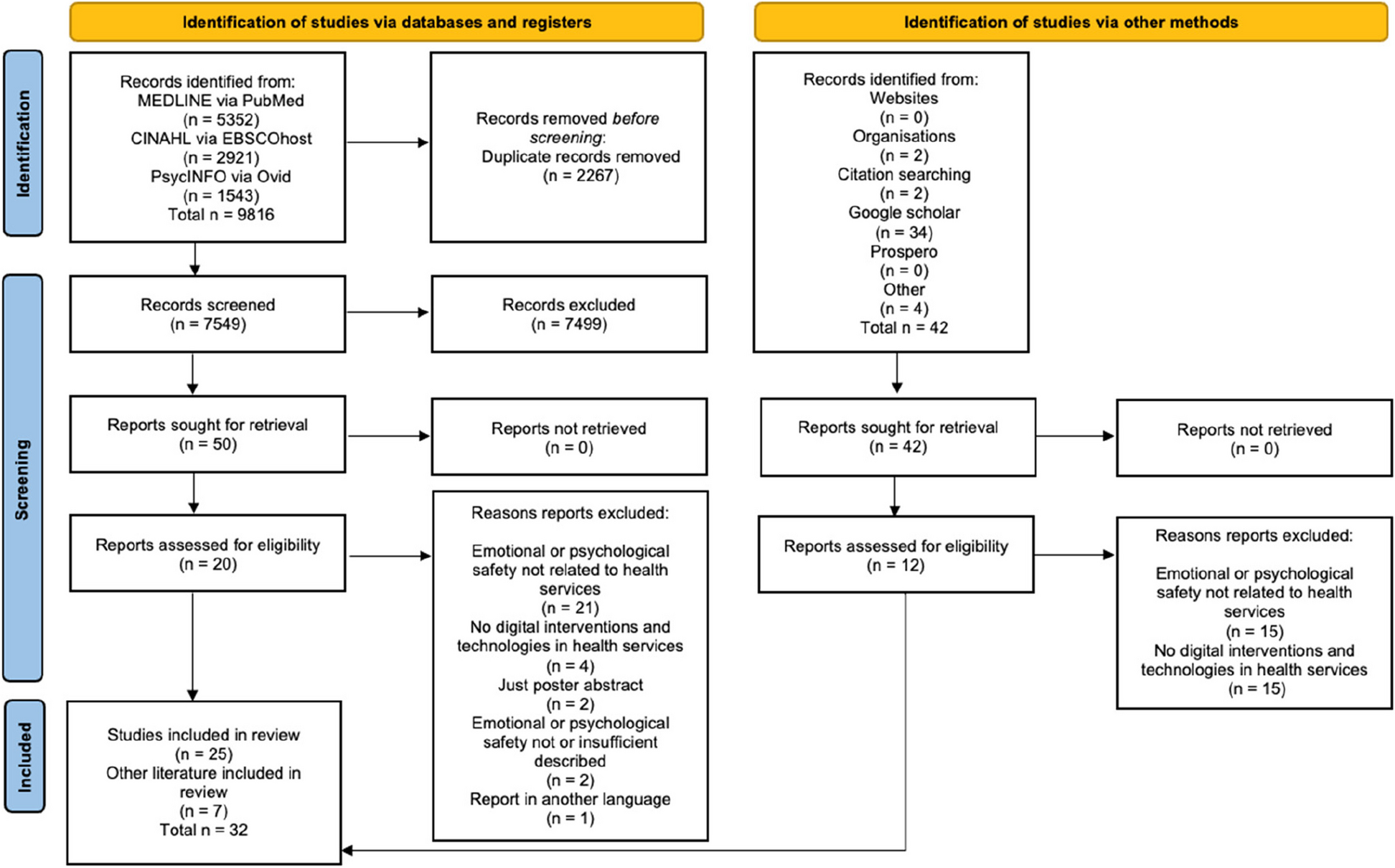






Our initial electronic database search generated 4626 titles. After searching and removing duplicates, 4508 titles remained. During the first round of screening, we excluded 4481 titles and reviewed the remaining 27 titles in more detail. Of the 27, 24 were excluded for reasons elaborated in Appendix 2 and three studies were included in the overview of systematic reviews [39, 43, 52]. Figure 1 below elaborates on the study screening and selection process.
Fig. 1
PRISMA flow chart for reviews identified and included in the review
Summaries of individual reviewsLopez et al, [39]Lopez et al. [39] stated that the aim was to ‘identify school-based interventions that improved adolescent contraceptive use’ [39] searched five databases. They also searched trial registries for recent trials. The study included twenty-one trials, but only the five studies that measured unintended pregnancy were included in this review. All five studies were cluster randomised control trials based in schools. The students were aged between 13 and 18 years. Four out of five studies occurred in the global north: two in the USA (Coyle [18], Kirby [36]) and two in the UK (Wight [76], Stephenson [65]) cited in [39, 69] South African study is the only exception. One study evaluated the effect of a school-based intervention that combined active learning, information provision, and skill development to reduce unsafe sexual behaviour and unwanted pregnancies and improve the quality of sexual relationships (Wight [76]), cited in [39]. Another study examined skills-based HIV, sexually transmitted Infections (STI) and pregnancy prevention curricula. It compared this to standard school-based activities related to the prevention of HIV, STI and pregnancy implemented by presenters from community-based agencies (Coyle [18]), cited in [39]. Another study addressed unwanted teen pregnancies holistically and looked at an interactive programme that addressed choice, body development, contraception and parenthood [69], cited in [39].
Two studies looked at peer-led interventions. The first peer-led interventions evaluated the impact of HIV (AIDS) and pregnancy prevention with activities focused on delaying intercourse and increasing contraception (Kirby [36]), cited in [39]. The second assessed a school-based peer-led sex education programme that focused on improving the quality of sexual relationships, STI and pregnancy prevention (Stephenson [65]), cited in [39].
Mason Jones et al. [43]Mason Jones stated the aim was ‘to evaluate the effects of school-based sexual and reproductive health programmes on sexually transmitted infections (such as HIV, herpes simplex virus, and syphilis), and pregnancy among adolescents’ [43] searched six bibliographic and two conference databases. The study included twenty-one trials, but only the six studies that measured unintended pregnancy were included in this review. All six studies were cluster randomised control trials based in schools. The students were aged between 13 and 18 years of age. Three studies were in sub-Saharan Africa (Duflo [22], [59], Cowan [16]) cited in [43]. Two in Europe (Henderson [30], Stephenson [65]) cited in [43] and one in Latin America (Cabezón [12]) cited in [43].
Teachers delivered interventions in four studies. The first, Cabezón [12], cited in [43], evaluated the Teen STAR programme, stressing abstinence, fertility awareness, and the psychological and personal aspects of sexuality. Contraceptive use was not recommended. The second, Henderson [30], cited in [43], looked at the effect of a teacher-based programme that advised students to delay sexual intercourse and encouraged condom use. The third was Duflo’s [22], cited in [43] trial that evaluated a teacher-delivered programme promoting abstinence until marriage. Ross [59], cited in [43], reviewed a teacher and peer assistant-led programme to provide knowledge and skills to delay sexual debut, reduce sexual risk-taking and increase appropriate use of health services.
Peer educators delivered two studies. Cowan [15], cited in [43], was delivered by professional peer educators whose HIV prevention activities adapted the ‘MEMAkwa Vijana’ programme, which included modules focused on self-awareness, communication, self-belief and gender. This was delivered alongside programmes to improve communication between parents and children and increase support for adolescent reproductive health. Stephenson [65], cited in [43], a trial that looked at trained peer educators who delivered sessions that focused on sexual communication and condom use, knowledge about pregnancy, STIs (including HIV), contraception and local sexual health services.
Oringanje et al. [52]The [52] review aimed to assess the effects of primary prevention interventions on unintended adolescent pregnancies. Oringanje et al. [52] searched ten electronic databases and three trial registers. The review contained fifty-three studies, but only eight that measured unintended pregnancy were included. Four were randomised control trials, and the remaining four were cluster randomised control trials. The study participants were aged between 12 and 19 years old. Five studies were in the USA (Herceg-Brown [31], Morrison-Beedy [48], Philliber [53], Howard [33], Kirby [36]) cited in [52]. For the remaining studies, Cabezon [12] took place in Chile, Wight [76] in Scotland, and Bonell [11] in England cited in [52].
All eight studies took a holistic approach to preventing unintended pregnancy. Four studies occurred within the school setting (Howard [33], Kirby [36], Stephenson [65], Cabezón [12]) cited in [52]. Cabezon [12], Howard [33] and Kirby [36] cited in [52] all delivered in-person sessions on health/STI education, skills building and contraceptive education. Similarly, Wight [76] cited in [52] delivered health/sex education, skills-building and contraceptive education. However, in this case, it was primarily delivered through interactive video.
Summary across reviewsThe included reviews reported results from 19 studies, of which four were included in more than one review (Cabezón [12]; Kirby [36]; Stephenson [65]; Wight [76]) cited in [39, 43, 52]. We did not remove the duplicates for this review but included them as individual trials. We had the following study designs: fifteen cluster randomised controlled trials and four individual randomised controlled trials.
Population and settingsThe primary target audience for all the studies included in the selected systematic reviews was adolescents. The age group started at 12–13 years; the overall upper limit was 19 years (Morrison-Beedy [48], cited in [52]). Three studies included male participants (Philliber [53], Kirby [36], Wight [76]) cited in [39, 52]. One study was unspecific (Howard [33] cited in [43, 52]). Sixteen out of 19 trials were in a school setting, and one was community-based. The setting was unclear for two studies included in this review (Morrison-Beedy [48], Philliber [53] cited in [52]). Eight trials were USA-based. Two trials were based in Chile, England, Scotland and the UK and one in Kenya, South Africa, Tanzania and Zimbabwe. Thirteen studies were conducted in high-, three in middle-, and three in low-income countries (LICs). Of the 19 studies included in the three reviews, four were conducted between 1986 and 1997, ten were between 2002 and 2008, and five were conducted between 2008 and 2015. All of the included reviews are at least 7 years old, and 74% were performed at least 10 years ago.
Teenage pregnancy prevention interventionsWe reviewed the nineteen studies and attempted to identify groups using the review author’s description. All interventions included sex education; therefore, studies were grouped based on additional intervention characteristics. We identified eight different adolescent pregnancy prevention intervention types or groups. All reviews did not contribute data to all categories but did contribute to at least one group.
Skills buildingInterventions that provide instruction, practice or other activities that are designed to help the target audience build and enhance their skills, i.e. teachers deliver better SRH classes or academic tuition for adolescents.
Two reviews [39, 52] reported data from five different studies (Coyle [18], Howard, [33]; Kirby, [36]; Wight, [76]; Philliber, [53]).
Wight [76] (cited in [52]) identified teachers’ lack of sex education training as a barrier to the effective delivery of sex education classes. This paper investigated whether a teacher training intervention primarily delivered through an interactive video that combined active learning, information provision and skill development would improve adolescent SRH outcomes. Coyle [18] (cited in [
留言 (0)